
Abstract
Abstract
Background
Pathologic or spontaneous fractures are recognised causes of morbidity in children. There is a paucity of data on their aetiology and patterns in African children.
Methods
A combined retrospective and prospective study of 47 children aged 15 and below with pathologic fractures of long bones seen from January 2000 to December 2006. The setting was the Orthopaedic and Traumatology department of the Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria.
Results
A total of 47 patients with a mean age of 5.3 years ± SD with pathologic fractures of 50 long bones were seen and treated. The most commonly affected bones were the femur (28%), tibia (28%) and humerus (26%). Chronic osteomyelitis following inadequately treated acute haematogenous osteomyelitis was the commonest cause of pathologic fractures (74.5%). The mean duration of fracture union was 6.8 ± 2.3 months and the outcome was satisfactory in 91.4% of cases.
Conclusions
The aetiology of pathologic fractures in the African population is different from their causes in Caucasian children. Chronic osteomyelitis following inadequately treated acute haematogenous osteomyelitis continues to plague many children in our environment.
Introduction
Pathologic or spontaneous fractures, though not as common as in adults, are recognised causes of morbidity in children. They are fractures through weak or diseased bones of abnormal composition, and most of the causes are benign [1]. The commonest cause of pathologic fractures in Caucasian children in most reports is simple or unicameral bone cyst [1–4]. This is most common in the humerus and proximal femur. Other causes are nonossifying fibroma, fibrous dysplasia, aneurysmal bone cyst, congenital pseudarthrosis of the tibia and osteogenic sarcoma [3, 4]. Fractures are also common in children with cerebral palsy, especially the nonambulant child on anticonvulsant therapy [5].
Pathologic fracture is a serious complication of osteomyelitis in children. It is especially common in chronic osteomyelitis of long bones in young patients with sickle cell disease [6, 7]. Chronic osteomyelitis is a debilitating disease that is common in developing countries. It is characterised by the formation of massive sequestra and involucra, with extensive destruction of bone. Pathologic fractures from these are slow to heal, and many heal with deformity. Acute osteomyelitis of long bones secondary to community acquired methicillin-resistant staphylococcus aureus has also been reported to cause pathologic fractures [8].
There is paucity of data on the aetiology and patterns of pathologic fractures in African children. This communication, a combined retrospective and prospective study of pathologic fractures in children seen at our centre, is an effort to bridge this gap. This would provide a database and enable us to identify factors that may influence the pattern and prognosis in pathologic fractures in children in our environment, with a view to instituting appropriate preventive measures.
Patients and methods
This is a combined retrospective and prospective study of all children aged 15 and below with pathologic fractures of long bones seen in the department of Orthopaedic Surgery and Traumatology of the Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria. The study covers the period from January 2000 to December 2006. Permission for the study was obtained from the Research and Ethics Committee of the hospital. The data extracted from the medical records of each patient were age, sex, presenting symptoms and signs, bone(s) affected, underlying pathology in the bone(s), laboratory features such as haemoglobin genotype, blood chemistry where indicated, biopsy results, microbiology of sinus swabs, X-rays of the limbs, treatment modality, duration of treatment and outcome. Diagnosis was based on clinical and plain X-ray features, with microscopy, culture and sensitivity results of intraoperative specimens where necessary.
All the patients with pathologic fractures of long bones, irrespective of aetiology, seen from January 2004 to December 2006 were prospectively studied. Those with chronic osteomyelitis and discharging sinuses had both sinus and intraoperative specimens sent for microscopy, culture and sensitivity to guide therapy. The patients were followed up for 2 months to 6 years. The data were analysed using standard statistical methods with the Statistical Package for Social Sciences (SPSS) Version 11.0.
Results
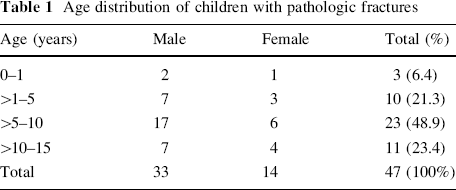
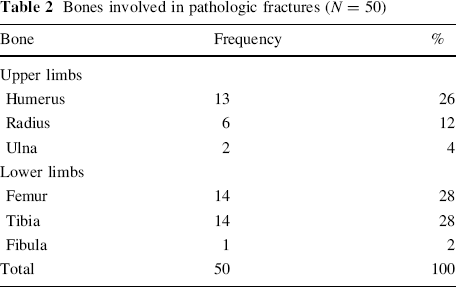
A total of 47 patients with pathologic fractures of 50 long bones were seen and treated during the study period. Their ages ranged from 9 months to 15 years (mean 5.3 years ± SD). There were 33 males and 14 females (M:F 2.4:1) (Table 1). The most common presenting features were pain (100%), swelling (85%), inability to use the affected limb (100%), discharging sinuses (74%, all patients with chronic osteomyelitis) and recurrent fever (42%). One infant, aged 9 months, presented with recurrent fractures from osteogenesis imperfecta. Table 2 shows the frequency of involvement of the long bones. The most commonly affected bones were the femur (28%), tibia (28%) and humerus (26%). Three patients had bilateral humeral, femoral and tibial shaft fractures respectively.
Age distribution of children with pathologic fractures
Bones involved in pathologic fractures (N = 50)
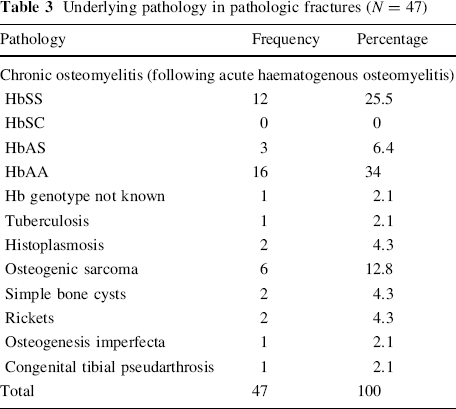
The underlying pathology or causes of pathologic fractures are shown in Table 3. Chronic osteomyelitis was the commonest cause (74.5%) (Figs. 1, 2). Other causes were osteogenic sarcoma, rickets, simple bone cysts and congenital pseudarthrosis. Amongst the patients with chronic osteomyelitis, 32 (91.4%) followed inadequately treated acute haematogenous osteomyelitis, whilst two (5.7%) had African Histoplasmosis (humerus [Fig. 3] and femur) and one (2.9%) had tuberculosis of the femur. The diagnosis of chronic osteomyelitis following inadequately treated acute haematogenous osteomyelitis was easily made based on the history of fever at onset, obvious sinuses with purulent discharge and the characteristic radiologic features of sequestra and involucra (Figs. 1, 2). The diagnostic challenge was in distinguishing tuberculosis and histoplasmosis from malignant bone tumour (Fig. 3). The haemoglobin genotypes of the patients are also shown in Table 3. Twenty of the 32 patients with chronic osteomyelitis had their aetiologic bacterial agents isolated. S. aureus was isolated in 16 (80%), proteus in two (10%), E. coli in one (5%) and klebsiella in one (5%).
Underlying pathology in pathologic fractures (N = 47)

Pathologic fracture of distal femur from chronic osteomyelitis

Pathologic fracture of proximal humerus (undisplaced) from chronic osteomyelitis in a patient with sickle cell disease

Pathologic fracture of distal humerus from African histoplasmosis
The treatment modalities are shown in Table 4a. Twenty-two fractures with obvious sequestra had sequestrectomy and curettage with excision of the sinus tract where necessary. This was followed by either cast immobilization or traction. The fractures of the two patients with African histoplasmosis healed following administration of ketoconazole and cast immobilization.
Treatment and outcome in pathologic fractures from chronic osteomyelitis (N = 35)

The duration of fracture union ranged from 2 months to 60 months (mean 6.8 ± 2.3 months).
The outcome was satisfactory (fracture union without residual discharging sinuses) in 32 patients (91.4%) (Table 4b). There was no mortality in the series. Two patients still had persisting sinuses in spite of fracture union.
Discussion
The most common cause of pathologic fractures in the population studied was chronic osteomyelitis. This is in contrast to what obtains in Caucasians, where benign bone lesions, especially unicameral bone cyst, are the commonest cause [1–4]. Only two patients had pathologic fractures of the humerus from bone cyst. The most commonly affected bones in pathological fracture are femur, tibia and humerus. The prevalence of chronic osteomyelitis as a cause of pathologic fractures in children is related to its prevalence in growing children and adolescents in most parts of Africa [6, 7, 9–12]. This results from misdiagnosis of acute osteomyelitis as pyomyositis by many general and family physicians, and therefore inadequate treatment, in our part of the world. The increasing patronage of traditional bone setters is also a factor. This causes delay in presentation to appropriate medical facilities. As a result of the delay in diagnosis and institution of appropriate treatment, chronicity sets in, with destruction of the structure of the bone. This leads to spontaneous fracture (Figs. 1, 2). The high prevalence of osteomyelitis may also be related to the prevalence of sickle cell disease in Nigeria [7, 10, 11]. Amongst the patients with pathologic fractures from osteomyelitis whose haemoglobin genotypes were known, HbSS constituted 12 of 31 cases (38.7%). Patients with sickle cell disease are prone to osteomyelitis as a result of splenic hypofunction (from autosplenectomy following frequent splenic infarction during vaso-occlusive crisis) and defective opsonins [13]. Marrow hyperplasia with marked cortical thinning and osteoporosis as a result of increased haematopoietic demand to compensate for haemolytic anaemia predisposes the sickle cell disease patient to pathologic fractures.
The diagnosis of chronic osteomyelitis complicating an inadequately treated acute haematogenous osteomyelitis is usually straightforward, especially when there are discharging sinuses with or without fever. However, the diagnosis of chronic osteomyelitis caused by tuberculosis or fungi (e.g. histoplasmosis) may be difficult, as the features may resemble those of a malignant bone tumour. The case shown in Fig. 3 was initially clinically diagnosed as a malignant tumour of distal humerus. It was the histology of the incisional biopsy that gave it away as African Histoplasmosis. The lesion resolved after a course of ketoconazole. The most common aetiologic bacterial isolate in pathologic fractures complicating chronic osteomyelitis was S. aureus, even amongst patients with sickle cell disease. This is consistent with the findings of other workers [9, 11, 13, 15].
The management of pathologic fractures from chronic osteomyelitis presented a formidable challenge in our experience. Unlike the fractures from rickets and bone cysts that united within the expected period, almost all the fractures from chronic osteomyelitis in this series took longer periods to heal (mean 6.8 months ± 2SD). One patient took 5 years to heal! Many of them presented with copious purulent discharge from the fracture site. There was marked osteoporosis in association with sequestra and involucrum in most of our patients (Figs. 1, 2). In some the involucrum was so little that sequestrectomy had to be delayed to avoid marked segmental bone defects. Such cases were usually immobilized with plaster casts or traction until enough involucrum had formed and the continuity of the bone restored. Sequestrectomy would then be carried out. Furthermore, pathologic fractures from chronic osteomyelitis from discharging sinuses are not amenable to the usual methods [1–3] of treating pathologic fractures from noninfective causes. All these put together would lead to delay in fracture union, and healing with deformity (Fig. 4). Chronic osteomyelitis continues to be a debilitating disease in Nigeria. In spite of the evolution of different treatment methods [14, 15], only marginal improvement has been achieved in its prognosis. Two of our patients still had persisting discharging sinuses at the time of writing this report. The best approach is to find ways of reducing the chronicity of the disease by prompt and adequate treatment of acute osteomyelitis. The primary health care and family physicians to whom these patients usually present in the acute stage should be educated on the clinical features of acute haematogenous osteomyelitis, to enhance early diagnosis and proper referral. The activities of quacks and traditional bone setters should be of grave concern to our governments in Africa.

Malunited femoral fracture following chronic osteomyelitis
In conclusion, the aetiology of pathologic fractures in Nigerian children is much different from the causes in Caucasian children. Chronic osteomyelitis following acute haematogenous osteomyelitis as a result of missed diagnosis or inadequate treatment continues to plague many children in our environment with dire consequences. Efforts should be directed at early diagnosis of acute osteomyelitis and adequate treatment.