
Abstract
Intractable ulcers often occur following primary diseases and have a significant impact on the quality of life of affected subjects. The medical treatments now available include compression and continuous debridement or additional interventions such as advanced wound dressings, local or systemic antibiotics with a mild benefit for the patients in the long term. In this report, we describe the use of autologous micrografts obtained by Rigenera® procedure in the management of two cases of intractable ulcers showing good outcomes for both patients approximately after 30 days from intervention. In the first case, a 74-year-old male with a diagnosis of Fournier’s gangrene who underwent several interventions showed a rapid wound epithelization after micrografts application. In the second case, a 63-year-old male affected by a left hallux ulcer with a diagnosis of chronic osteomyelitis also showed a gradual reduction in the ulcer approximately after 1 month from micrografts application.
Introduction
Intractable ulcers and osteomyelitis are pathological conditions with a significant impact on the quality of life of affected subjects and with a complex management. Standard therapy includes compression and continuous debridement or additional interventions such as advanced wound dressings, local or systemic antibiotics, and venous surgery has been extensively investigated.1,2 Furthermore, various types of vacuum-assisted closure therapy and continuous negative pressure wound therapy devices have been used for proliferation of granulation and wound cleansing. 3 In this study report, we describe the use of Rigenera® procedure to treat two referral patients, one affected by an intractable ulcer resulting from Fournier’s gangrene and another affected by foot osteomyelitis. Rigenera procedure is a clinical protocol based on the use of autologous micrografts obtained by mechanical disaggregation of small piece of tissues through a device called Rigeneracons (Human Brain Wave SrL, Italy). The micrografts thus obtained are enriched with progenitor cells and are able to maintain a high cell viability and regenerative potential.4,5 The concept of micrografting was introduced by Meek 6 and is based on the evidence that smaller grafts have a greater regenerative potential due to less distance between them and a lesser distance for epithelial migration. Several protocols were further developed to improve the grafts’ expansion rate and to accelerate wound epithelialization, such as expanded mesh skin grafts 7 and more recently minced expansion grafts (MEGs). 8
Case 1
Current medical history
In August 2017, a 74-year-old man feeling ill and with a fever was found collapsed on the street and was immediately taken to a nearby hospital. Diagnosed with Fournier’s gangrene and with a past medical history of hemodialysis due to diabetes and chronic renal failure, the patient underwent debridement and bilateral orchiectomy under general anesthesia 3 days after the recovery. Another debridement under general anesthesia was performed at a later date, and the patient received a split thickness skin graft (donor site: left thigh), resulting in 70% of graft failure. Five successive skin grafts and/or sclerotherapy were performed, but the wound proved to be intractable. Wound culture indicated the presence of methicillin-resistant Staphylococcus aureus (MRSA) 3+ and Pseudomonas aeruginosa 3+. Continual negative pressure wound therapy was conducted to induce wound closure; however, the wound did not heal, and the patient was referred to our department in January 2018.
After a few days of wound cleansing at our department, the patient under general anesthesia underwent debridement and cleansing of ulcers in the perianal and left groin (Figure 1(a) and (b)). This was followed by a buried chip skin graft, and Rigenera procedure was performed using dermal micrografts (Figure 1(c) and (d)). Briefly, a dermis graft of 1 × 0.5 cm2 was collected and disaggregated by Rigeneracons medical device adding 1.2 mL of sterile saline solution, as previously described. 9 After the disaggregation, 1.0 mL of micrografts suspension was collected and injected into the granulation (approximately 0.1 mL of micrografts suspension per 1 cm2).
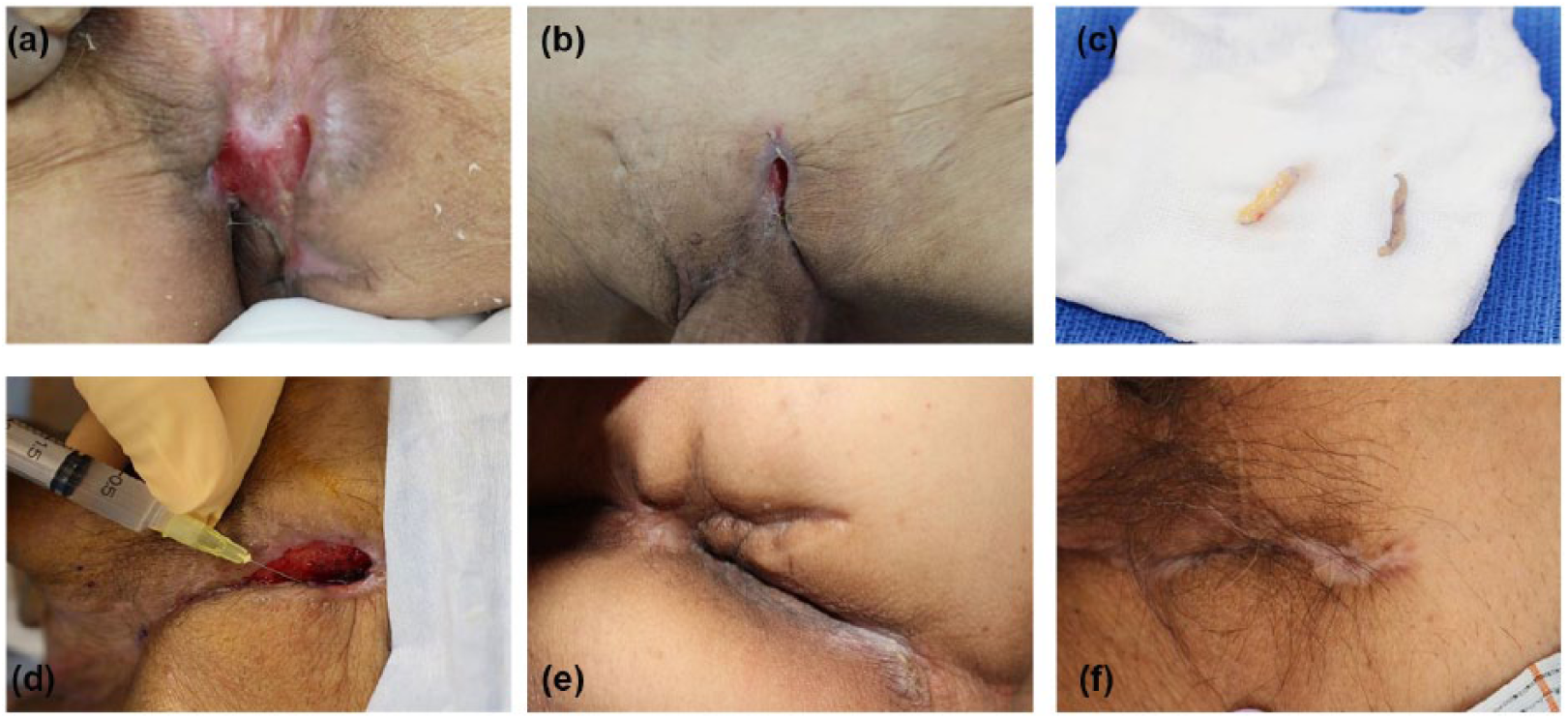
Case 1: (a, b) Initial diagnosis shows intractable ulcer of the perineum. (c) Dermis and epidermis harvested from the groin area. (d) Micrografts were injected into the ulcer area. (e) Buttocks: rapid contraction and complete recovery after treatment. (f) Pubis: rapid contraction and complete recovery.
Thereafter, the wound areas showed rapid contraction and epithelization (Figure 1(e) and (f)), and the patient was transferred back to the initial hospital in March for rehabilitation. The patient was discharged from the hospital at a later date, and at follow-up in June, no recurrence has been observed.
Case 2
In October 2017, a 63-year-old man, affected by a left hallux ulcer with a past medical history of diabetes and vitreous hemorrhage, visited a nearby plastic surgery hospital and was given a conservative treatment consisting of a topical drug prescription and functional orthotics for decompression. The treatment showed no improvement, and the patient came to our hospital as an outpatient in March 2018. An ulceration was formed on the sole of the left hallux, and bone destruction was observed under X-ray inspection (Figure 2(a) and (b)). The diagnosis was a chronic osteomyelitis requiring invasive surgical treatment; therefore, the patient was hospitalized. On admittance day, skin perfusion pressure of foot dorsum was 52 mm Hg and foot sole was 115 mm Hg, showing good measurements. The day after, skin of the ulcer on the left hallux was resected in a spindle shape after administering conduction anesthesia, and a curettage was performed on the interphalangeal joint using Luer forceps, which was then cleansed with saline solution (Figure 2(c)). Dermal tissue was harvested from the left groin area, and dermal micrografts were obtained by Rigenera procedure (Figure 2(d)). As reported above, a dermis graft of 1 × 0.5 cm2 was collected and disaggregated by Rigeneracons medical device adding 1.2 mL of sterile saline solution, obtaining 1.0 mL of micrografts suspension that was injected into the granulation tissue (approximately 0.1 mL of micrografts suspension per 1 cm2).

Case 2: Ulcer of left hallux. (a) Image of ulcer. (b) X-ray control reported bone destruction. (c, d) Intraoperative procedure with debridement and micrografts injection. (e) Artificial dermis was sutured over the injected area. (f) Complete recovery seen after approximately 1 month. (g, h) X-ray control after 1 and 9 months from micrografts application.
The defective area of the bone and soft tissue was filled with AQUACEL® Ag, and artificial dermis was sutured over it (Figure 2(e)). During perioperative period, MRSA was detected in the wound culture, and the patient was put on oral linezolid treatment. On the seventh day post-surgery, oral medication was switched to Baktar, and then Dalacin. At the same time, gradual reduction in the ulcer was confirmed (Figure 2(f)). After 8 days, the patient was put on walking aid with heel load. During this time, the wound continued to show progressive reduction. At the end of April, the wound healing was progressing satisfactorily, and the patient, still keeping on topical medication and decompression, was discharged from the hospital. Wound healing was confirmed during outpatient revisit at the end of May and, to date, no recurrence has been observed. Furthermore, we performed an X-ray analysis after 1 and 9 months from micrografts application to evaluate the arrest or progression of bone destruction. We reported no significant difference after 1 month (Figure 2(g)), but after 9 months, we observed a bone regeneration in the hallux proximal phalanx (Figure 2(h)).
Discussion
Prior to coming to our hospital for medical treatment, both patients initially underwent treatments over a few months for intractable ulcer and osteomyelitis at other plastic surgery hospitals, without any visible healing. After thorough management of the infected wound sites, and, after confirming that there were no drop in skin perfusion pressure of the foot, debridement and necrotomy were performed. This was followed by the Rigenera procedure, with healing observed in approximately 1 month. Previous studies have described the clinical effectiveness of this protocol in the management of chronic wounds, such as dehiscences and ulcers,6–9,12–14 and the results reported for Case 1 are in line with other authors who have already reported the role of micrografts in the reactivation of wound healing resulting from Fournier’s gangrene. 10
The clinical healing processes for intractable ulcer cases experienced at our department show a characteristic wound contraction. In Case 2, the patient’s hallux healed, leaving the length of the toe shorter. This may possibly be seen as a drawback, but considering the fact that the chronic osteomyelitis wound failed to epithelialize for a few months prior to this treatment, the wound contracture is not considered to be a major issue and may be that myofibroblasts growth occurs more easily.
In vitro investigations are necessary to better elucidate the role of dermal micrografts in the healing process, even if in vivo studies have reported that micrografts are able to stimulate transforming growth factor (TGF)-1 production in early phase granulation, as well as myofibroblast proliferation, neovascularization and collagen accumulation. 11
Conclusion
Although various factors may be involved, chronic ulcers not only consume medical resources but also contribute to an increase in medical costs itself. In this case report, we described good outcomes for two intractable ulcers treated with micrografts. Long-term follow-up cases and other comparative studies, that is, comparing micrografts to other skin graft techniques, are to be expected in the future to confirm their benefits.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.