
Abstract
Abstract
Purpose
There is not always a good outcome after a femoral varus osteotomy (FVO) in those with Legg-Calvé-Perthes disease (LCPD), even when the severity warrants surgical treatment. The purpose of this study was to find arthrographic indicators for decision making regarding the likely surgical outcome of a FVO.
Methods
We used an image of an abduction position during preoperative arthrography under general anesthesia that simulated the post-operative relationship between the femoral head and the acetabulum. In the image, we defined two indicators of how deeply the deformed epiphysis was contained within the acetabulum: an acetabular head index in abduction and an epiphyseal slip-in index. Finding the contact point between the top of epiphysis and acetabulum was the key for the epiphyseal slip-in index measurement. In 37 patients (38 hips) who underwent FVOs based on our inclusion criteria, these two indices were measured retrospectively and were analyzed for a correlation with surgical outcome. Surgical outcome was evaluated using a combination of three factors: sphericity of the femoral head (Stulberg's classification), acetabular cover (acetabular head index), and the slope of acetabular roof.
Results
The outcome was acceptable in 20 hips (52.6%) and unacceptable in18 hips (47.4%). There was a statistically significance difference in epiphyseal slip-in index between the acceptable group (21.9 ± 2.8%) and the unacceptable group (15.0 ± 4.4%) (P < 0.0001). An index of 20% or more determined a safe zone for predicting an acceptable outcome with 80% sensitivity, 89% specificity, and a 7.2 likelihood ratio. However, the acetabular head index in abduction showed no such statistical significance.
Conclusions
In this study, we found that the epiphyseal slip-in index was a reliable indicator for predicting the effectiveness of a FVO. It is worth measuring this index when a surgeon is considering a FVO for a patient with severe LCPD. (Level of Evidence Level III.)
Keywords
Introduction
Surgical indications for treatment of patients with Legg-Calvé-Perthes disease (LCPD) have been discussed previously by several authors [1–3]. Each author decided to perform operations on patients with severe LCPD based on his/her own criteria, which may include age at onset, radiological findings (Herring's or Catterall's classification), or prolonged limitation of range of hip motion [4–6]. A femoral varus osteotomy (FVO) has become the most prevalent method for the surgical treatment [1, 3, 7–9]. However, this has not always produced good results in past studies [10–12]. Reasons for such poor outcomes include an onset of more than 9 years, a Herring's class C, an advanced stage of fragmentation at surgery, and pre-operative hinge abduction. But these factors, except hinge abduction, could not always preclude a FVO. Hinge abduction involves serious deformity of the femoral head, and containment cannot be achieved with abduction in arthrography. Axer et al. stated that arthrography can help in making the final decision and in more precisely tailoring the osteotomy angle to the demands of the particular pathological condition in the hip [13]. However, even if no hinge abduction is confirmed, the surgical outcome is not always acceptable. It would widely spread from a good configuration in both the femoral head and the acetabulum to some remaining deformity in either the femoral head or the acetabulum. Therefore, there is a need to precisely evaluate the degree of containment during arthrography in order to decide whether or not to perform a FVO.
The purpose of this study was to find arthrographic indicators for decision making regarding likely surgical outcome of a FVO.
Methods
Between 1990 and 1999, from a total of 106 LCPD patients, 37 (38 hips) underwent FVOs. The surgery rate was 34.9%, which was similar to the generally accepted rate for poor outcomes treated conservatively in Perthes’ disease [4, 14]. There were 34 male and 3 female patients. Of these, 29 were unilaterally affected and 8 bilaterally affected. Of the 8, 1 underwent FVOs on both sides, and the remaining 7 only on one side. The average age at diagnosis was 8.4 ± 1.9 years and the average time from onset to surgery was 3.5 ± 3.0 months. FVOs were performed within 3 months of onset in 20 hips, 3–6 months in 11, and after more than 6 months in 7. The 19 patients who underwent operations 3 months or more after onset were at first treated conservatively with a Tachdjian-type brace or were just observed. The average ages at surgery and at the latest follow-up were 8.7 ± 1.9 years and 18.5 years, respectively. All patients had reached maturity at the final follow-up. Our surgical decision was decided on the basis of inclusion criteria before the healing stage, which were either an age of at least 8 years at onset and Herring's class B [5] or Catterall's III [4] with subluxation (more than 3 mm difference from unaffected side) or persistent limitation of the range of hip motion, or all ages with Herring's class C or Catterall's IV [3].
Retrospectively, we focused on the image of the hip in a 40° abduction position during preoperative arthrography that had been performed under general anesthesia at the necrotic stage in 32 hips and at the regenerative stage in 6 hips, which simulated the post-operative relationship between the femoral head and the acetabulum. The 40° abduction reflected about a 100° post-operative varization that we aimed for during the operation. In the image, we defined two indices as indicators of how deeply the deformed epiphysis was contained within the acetabulum: an acetabular head index in abduction (AHI-abd) and an epiphyseal slip-in index (ESI). The AHI-abd was measured in the same manner as a conventional AHI in the neutral position (Fig. 1). The ESI was defined as the ratio of the horizontal distance (parallel to the inter-teardrop line) between the lateral edge of the bony acetabular rim and the top (tangential point) of the epiphysis slipping into the acetabulum in 40° abduction to the acetabular depth (the horizontal distance between the tip of the teardrop and the lateral edge of the bony acetabular rim) (Fig. 2). Finding the contact point between the top of the epiphysis and acetabulum was the key for measurement of ESI. When the contact point was unclear and delineated as a short flat line rather than a point, the mid-point of the line was used for the measurement. The caput index was also measured [15]. These measurements were performed using Image J 1.33u software (National Institutes of Health, USA).
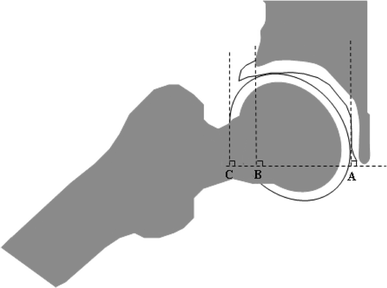
Acetabular head index in abduction. The index was calculated as AHI-abd = 100(A−B)/(A−C), where A−B is the horizontal distance between the most medial surface of the head and the lateral margin of the bony acetabular rim in abduction and A−C is the horizontal distance between the most medial surface of the head and the most lateral surface of the head in 40° abduction
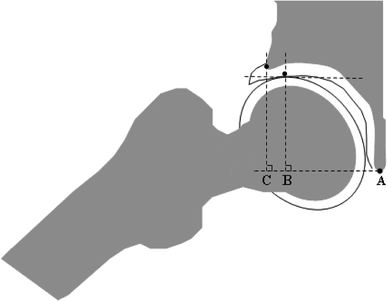
Epiphyseal slip-in index. The index is calculated as ESI = 100(B−C)/(A−C), where A−C is the horizontal distance between the lateral margin of the bony acetabular rim and the tip of the tear drop (acetabular depth), and B−C is the horizontal distance from the lateral margin of the bony acetabular rim to the tip (tangential point) of the epiphysis slipping into the acetabulum in 40° abduction
Two staff surgeons (M.K., T.S.) and one resident (Resid) measured the AHI-abd and ESI separately to minimize inter-observer error. The two staff surgeons measured the two values in the same series of patients again 1 month later to evaluate intra-observer error. One staff surgeon had 31 years of experience in orthopedic surgery and the other had 19 years. Care was always taken to keep patients’ pelvises level on coronal and transverse planes throughout the whole process of arthrography. Symmetrical obturator foramina and width of iliac wings gave us good confirmations for proper projections.
Final outcome was radiologically evaluated with the combination of the following three factors: sphericity of the femoral head (Modified Stulberg's classification [6]), acetabular cover (acetabular head index; AHI [16]), and the slope of acetabular roof (SAR [17]). We modified the Stulberg's classification by separating class III into two subclasses. Patients with class IIIa had a difference of 1–2 mm using Mose's method, and patients with class IIIb had a difference of 3 mm or more in aspherical congruency. Class I or II, indicating a completely spherical femoral head, is indicated as 0 mm when using Mose's method. Patients were evaluated as “acceptable” if they met the following three conditions simultaneously: Stulberg's class I, II, or IIIa; 75% or more of AHI; and positive SAR (>0°). All other patients were evaluated as “unacceptable”.
A statistical analysis was performed using the Mann–Whitney U-test. The intraclass correlation coefficient was used to assess the intra- and inter-observer errors (SPSS Inc., Chicago, Illinois). A P value of <0.05 was considered significant.
Results
Over-all results
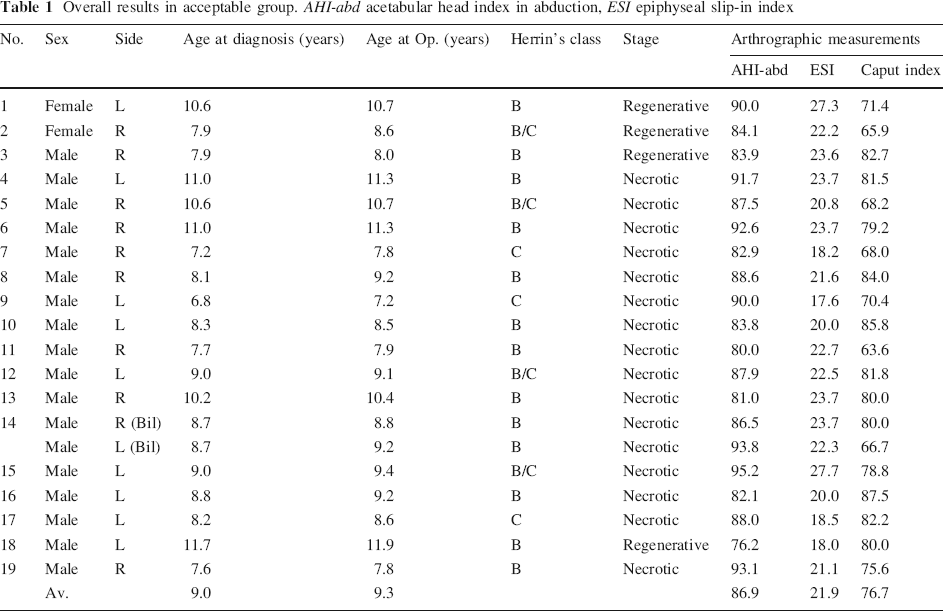
Overall results in acceptable group. AHI-abd acetabular head index in abduction, ESI epiphyseal slip-in index
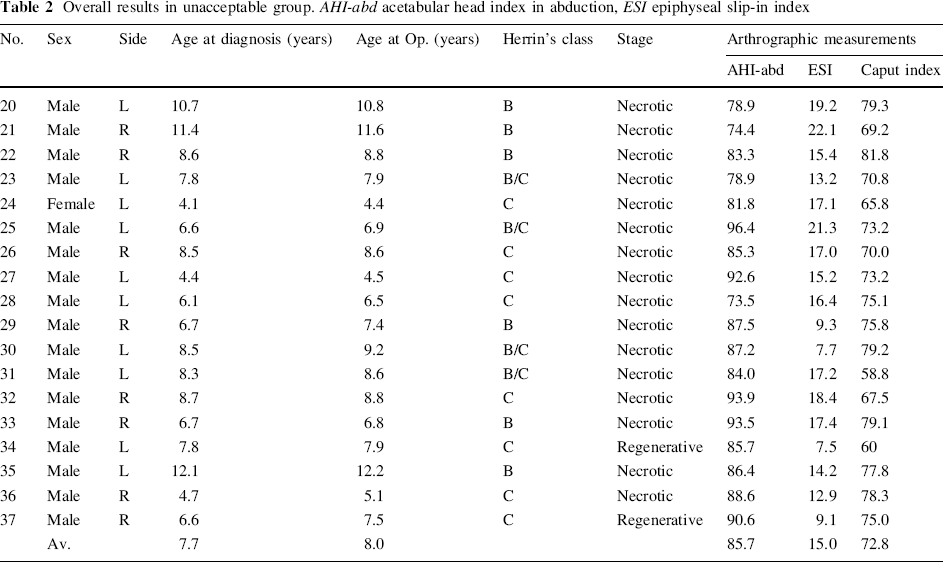
Overall results in unacceptable group. AHI-abd acetabular head index in abduction, ESI epiphyseal slip-in index
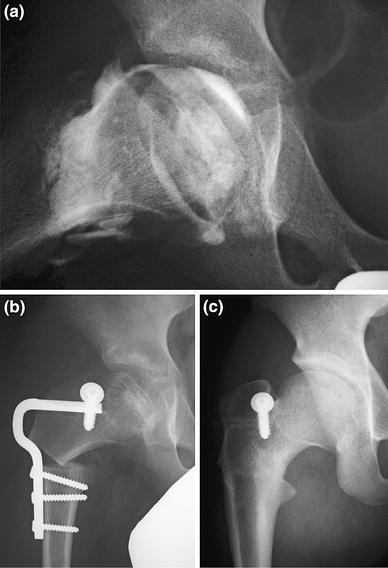
Case 13 in acceptable group. 10.4-year-old boy with Herring's class B (Catterall's type III).
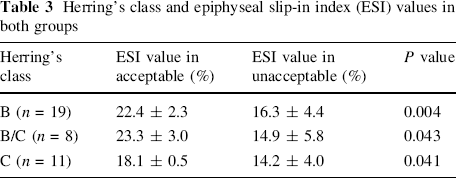
Herring's class and epiphyseal slip-in index (ESI) values in both groups
Cut-off value for prediction
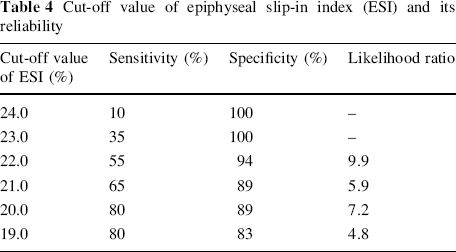
We provisionally designated six cut-off values of ESI, corresponding to every 1% difference in the range from 19 to 24% for the 21.9 ± 2.8% mean value in the acceptable group, to separate hips likely to be classified as acceptable or unacceptable. We performed statistical analyses for sensitivity, specificity and likelihood ratio for each cut-off value (Table 4), and also showed a Receiver Operating Characteristic (ROC) curve (Fig. 4). Patients with an ESI of at least 20% were likely to have acceptable outcomes and patients with an ESI less than 20% were likely to have unacceptable outcomes. The sensitivity of this cut-off value was 80% and the specificity was 89%. The calculated likelihood ratio was 7.2. Furthermore, a 20% cut-off value with a sensitivity of 0.8 and specificity of 0.89 showed the closest point to the top left corner in the ROC curve.
Cut-off value of epiphyseal slip-in index (ESI) and its reliability
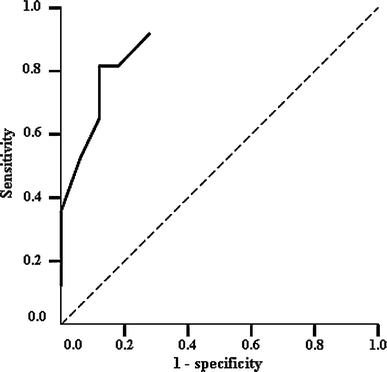
Receiver Operating Characteristic (ROC) curve. The optimal cut-off value was the closest point to the top left corner. This corresponded to a 20% cut-off value with a sensitivity of 0.8 and specificity of 0.89
These results showed that an ESI of 20% or more was the most reliable parameter for predicting a good surgical outcome of a FVO.
Intra- and inter-observer reliability
The intra-observer intraclass correlation coefficients for each of the two staff surgeons were 0.99 (95% CI, 0.98–0.99) (MK) and 0.99 (95% CI, 0.98–0.99) (TS) in measurement of the ESI. The inter-observer intraclass correlation coefficient for the three raters was 0.98 (95% CI, 0.96–0.99). These results indicated acceptable intra- and inter-observer reliability.
Discussion
When compared with natural history studies or studies of non-containment methods, Aksoy [10] and Noonan [12] concluded that FVOs provided better results in patients younger than 9 years of age. Joseph [11] concluded that the benefits of a FVO were most evident when the operation was performed either in the stage of avascular necrosis or in the early stage of fragmentation. Those findings have generally supported our decision making about FVO, but even so the criteria do ensure good a surgical outcome. However, hinge abduction was the only basis for excluding a FVO. Surgeons considering this technique have to perform preoperative arthrography and at least have to confirm that no hinge abduction appears in the abduction position, although its absence does not ensure good surgical outcomes.
We used an image of an abduction position during preoperative arthrography under general anesthesia that simulated the post-operative relationship between the femoral head and the acetabulum. Arthrographic analyses in LCPD have been reported often so far. The aims have been to observe the cartilaginous configuration of the epiphysis and the acetabulum in the neutral position. Rarely has the configuration been examined in the abduction position [19–22]; although screening of hinge abduction has been done, it was quite qualitative and subjective [23].
The ESI cut-off value we have proposed indicated how deeply the deformed epiphysis was contained within the acetabulum in abduction. Hinge abduction must have a negative value of ESI as a quantitative and objective parameter. The cut-off value of 20% had 80% sensitivity, 89% specificity and a 7.2 likelihood ratio, which means that there is less chance of surgical failure when using this criterion rather than other cut-off values. Patients with an ESI of at least 20% are about seven times more likely to be classified into the acceptable group. Furthermore, the ROC curve verified that the 20% ESI was the most reliable indicator for decision making of FVO. Thus, the 20% ESI cut-off will define a safe zone for obtaining acceptable results. This ESI cut-off is a reliable indicator for creating more remodeling effects in both the epiphysis and acetabulum after a FVO.
In our previous review of the comparative study of FVOs versus conservative treatment, surgical treatment produced better results for the sphericity of the femoral head and the acetabular cover than conservative treatment [3]. However, the acetabular roof did not reform nicely. Presumably, this phenomenon resulted from incomplete containment effects in which a not-deeply located top of the epiphysis interfered with the acetabular rim. Therefore, if a FVO is performed in patients who have at least 20% ESI, and the epiphysis is located deeply in the acetabulum, we can expect both a spherical femoral head and a well-reformed acetabulum that will protect the affected hip from osteoarthritis in adulthood.
Only 3 of 11 patients with class C were classified into the acceptable group, and all 3 had ESI values less than 20% of (average 18.1 ± 0.5%). Patients with class C were unlikely to have ESI values of 20% or more. This is consistent with the fact that patients with Herring's class C rarely had a good outcome, even with surgical treatment. However, the ESI values of class C patients in the acceptable group were significantly different from those in the unacceptable group (Table 3). It is possible that a better estimate of ESI values could provide an indicator for better surgical outcome, even in patients with class C. Further investigations should be continued with larger numbers of class C patients.
The degree of surgical varization should be chosen only after obtaining at least 20% of ESI in pre-operative arthrography. The targeted varization was usually about 40°, resulting in 100–105° of post-operative femoral neck angle, which is recommended by some authors [24, 25]. The post-operative neck-shaft angle with the average of 110.5°, slightly bigger than the targeted one, resulted mainly from post-operative remodeling in both the epiphysis and femoral neck. Also, epiphysiodesis of the greater trochanter was performed simultaneously with a screw fixation or drilling method to prevent a high trochanter, because 40° of varization might be considered as excessive varus. Nevertheless, if the Trendelenburg gait appeared due to a high trochanter afterwards, the advancement of the greater trochanter was considered. We have performed the advancement of greater trochanter in about 10% of our patients so far, but very few patients needed further valgus osteotomies due to excessive varus. Although the reduction of hip abduction necessarily occurred after the FVO, it gradually improved to at least 30° abduction within 1 year after surgery.
We concluded that our surgical outcomes were not satisfactory in resolving 47% of the hip injuries. However, this study has clarified an exact indicator for predicting good surgical outcomes of FVOs based on the findings of pre-operative arthrography. The ESI value was the most reliable parameter for the indication of FVOs, and an ESI of at least 20% defined a safe zone for acceptable surgical outcomes of FVOs. Therefore, the ESI value is worth measuring when a surgeon is considering a FVO for a patient with severe LCPD. We believe it is necessary to adopt a new treatment strategy for patients with an ESI less than 20%.