
Abstract
Abstract
Purpose
Computed tomography (CT) is the current imaging standard for confirming the diagnosis of a calcaneonavicular coalition. The purpose of this study was to evaluate three-dimensional (3D) multi-planar CT images of calcaneonavicular coalitions and adjacent tarsal relationships, compared to controls, in order to obtain an understanding of the 3D anatomy for classification and as an aid to surgical resection.
Methods
All patients who underwent CT of bilateral feet at our institution to evaluate a suspected calcaneonavicular coalition between 9/2005 and 3/2008 were retrospectively reviewed. Seventy-four feet (37 patients) were included in this analysis. In addition, 12 patients with a presumed normal calcaneonavicular relationship, who underwent CT of bilateral feet for various other diagnoses, were included as a control cohort. Seven measurements were performed on the 3D reconstructions to quantify the shape of the coalition (dorsal and plantar widths of the calcaneal and navicular contributions, coalition depth of the calcaneal and navicular contributions, and coalition length). The coalitions were classified into four types based on their appearance and their relationship to adjacent tarsal bones.
Results
32/37 patients (86%) were noted to have bilateral involvement (69 coalitions). Coalitions were categorized into four types: Type I (forme fruste)—28%, Type II (fibrous)—23%, Type III (cartilaginous)—45% and Type IV (osseous)—4%. The average shape of the coalition was found to be a curved wedge, which was on average 16 mm wide dorsally, 7 mm wide on the plantar surface, 10 mm in length, and 25 mm in depth.
Conclusions
3D CT reconstructions enabled the classification of the spectrum of calcaneonavicular coalitions. The shape of the cuboid was found to correlate with the extent of ossification. In Type I or II coalitions, the cuboid extended medially plantar to the fibrous connection. In more complete Type III or IV coalitions, the cuboid was “squared off” and remained lateral to the osseous bridge. An understanding of the 3D anatomy is important when diagnosing milder forms of coalitions, and during resection in order to avoid iatrogenic injury to the calcaneus, head of the talus, or cuboid.
Introduction
Tarsal coalitions were originally described by Zuckerkandl in 1877 [1]. The accepted theory for the etiology of tarsal coalitions was first proposed by Leboueq in 1890 [2] and later confirmed by Harris [3]. Fetal foot dissections performed by Harris revealed the failure of differentiation and segmentation of the mesenchymal anlage of two or more hindfoot bones during the embryonal period.
An abnormal coalescence (osseous or non-osseous) of the calcaneus with the tarsal navicular bone may be present in more than 50% of patients with a tarsal coalition [4]. An osseous calcaneonavicular coalition is most often diagnosed with conventional radiographs using a 45° medial oblique image of the foot [5–8]. A non-osseous calcaneonavicular coalition can, however, be more difficult to appreciate on plain X-rays. Computed tomography (CT) has recently become the “gold standard” for diagnosing coalitions, as it allows for bilateral comparison and permits better characterization of the extent of joint involvement, the composition and location of the coalition, and the degree of degenerative change of the affected and adjacent joints [9–11].
Recently, three-dimensional (3D), multi-planar reformatted CT images have allowed physicians to further evaluate the bony relationships of the foot [12, 13]. A thorough analysis of 3D reconstructions of calcaneonavicular coalitions and an evaluation of their utility in surgical planning have not, however, been performed previously. Therefore, the purpose of this study was to evaluate calcaneonavicular coalitions and adjacent tarsal relationships, compared to controls, using multi-planar reformatted CT images to obtain a 3D understanding of the anatomy for classification and as an aid to surgical resection.
Materials and methods
In this study approved by the Institutional Review Board, a retrospective review was performed of all patients who underwent CT of bilateral feet at our institution to evaluate a suspected calcaneonavicular coalition based on physical exam and radiographic findings between September 2005 and March 2008. Thirty-seven patients (29 males and 8 females) with an average age of 13 ± 2 years (range: 9–19 years old) met the inclusion criteria. 3D reconstructions of all 74 feet were analyzed.
A cohort of patients with a presumed normal calcaneonavicular relationship who presented to our institution with foot or ankle complaints, and were evaluated with CT of bilateral feet during the same time period, were also included in this analysis. Twelve patients (7 males and 5 females) with an average age of 12 ± 3 years (range: 7–17 years old) were included in the control cohort. 3D reconstructions of all 24 feet were analyzed. The diagnoses in this cohort of patients included: symptomatic accessory navicular, pes planovalgus, foot or ankle fractures, and calcaneal cyst.
The principal clinical examination findings thought to be indicative of a calcaneonavicular coalition included: reduced subtalar motion (inversion and eversion), reduced ankle plantar flexion (usually ≤ 10°), and a palpable, commonly tender, bony ridge (coalescence) distal to the sinus tarsi. As per the senior author's clinical pathway, conventional radiographic imaging of bilateral feet was performed for all patients prior to obtaining advanced imaging. To ensure quality CT imaging, age-appropriate sedation was administered as needed in the younger patients.
CT image acquisition
A General Electric (GE) LightSpeed Volumetric CT scanner (General Electric, Milwaukee, WI, USA) was used to perform all examinations. According to the Tarsal Coalition Protocol at our institution, all patients were positioned supine on the examination table with both feet flat against a positioning box. The patients were scanned feet first from the bottom of their feet proximally through their ankle joint. All examinations were performed without intravenous contrast, and the total examination time was less than 10 min in all cases. Helical scanning with a 0.625-mm section thickness was used in all cases. The field of view was centered over the foot, with 120-kV, 120- to 200-mA and 0.5-s helical scans performed. The raw axial 2D CT data were uploaded to a GE Advantage workstation and volume rendering software (version 4.3) was used to reconstruct the sagittal and coronal planes using a standard algorithm (Fig. 1). 3D reconstructions were generated after selecting the appropriate density threshold for bone (usually 180 Hounsfield units).

Three-dimensional reconstruction of a foot with a near-complete calcaneonavicular coalition (white circle)
Image processing and data acquisition
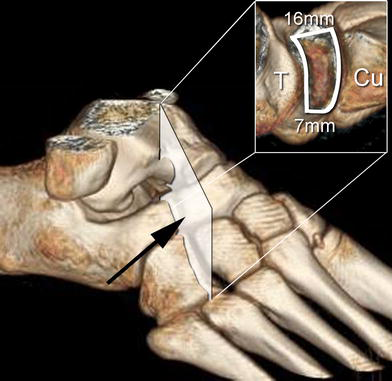
All examinations were reviewed by the three co-authors. 3D reconstructions of each foot were cropped (Fig. 2) to isolate the relationships between the calcaneus and navicular and two adjacent tarsal bones (talus and cuboid). Seven measurements were performed on each cropped 3D reconstruction. Navicular and calcaneal widths were measured on both the dorsal and plantar surfaces of the coalition. The width of the navicular contribution to the coalition was measured at the medial border of the lateral cuneiform–cuboid joint (Fig. 3). The width of the calcaneal contribution to the coalition was measured along the lateral border of the cuboid–calcaneal joint (Fig. 3). The distance between these two width measurements was determined to be the length of the coalition. Lastly, the depth or thickness of the coalition was also measured for both the navicular and calcaneal contributions (Fig. 4). All measurements were performed digitally using the volume rendering software, which had been electronically calibrated on image acquisition.
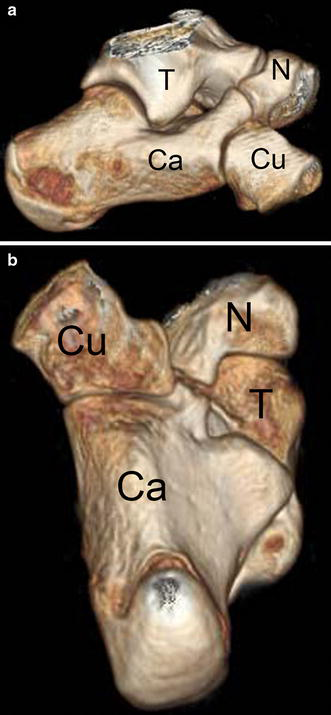
Lateral (
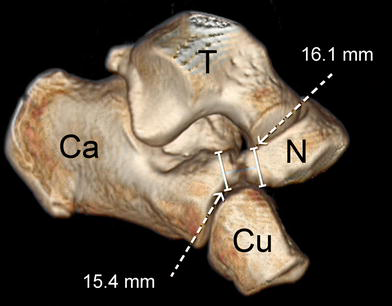
Measurements of coalition width for the dorsal surfaces of the calcaneus (Ca) and navicular (N) contributions
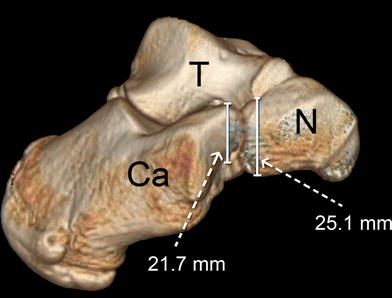
Measurements of coalition depth for the calcaneal (Ca) and navicular (N) contributions
Results
Thirty-two patients (86%) were noted to have bilateral calcaneonavicular involvement, resulting in 69 CT identified coalitions.
CT measurements
Seven measurements were performed using the 3D reconstructions of the 69 feet with CT identified coalitions (Table 1). The average width of the calcaneal and navicular contributions on the dorsal surface of the coalition were 15.9 ± 1.3 and 15.5 ± 1.6 mm, respectively. On the plantar surface of the coalition, the widths of the calcaneal and navicular contributions were 7.0 ± 0.9 and 6.7 ± 1.1 mm, respectively. The average length of the coalition measured 10.6 ± 0.9mm. The depth or thickness of the coalition was also measured. The calcaneal portion averaged 25.0 ± 1.6mm, while the navicular portion averaged 24.4 ± 1.8mm. The resulting shape of the coalition was determined as a curved wedge with an average dorsal width of 16 mm, plantar width of 7 mm, depth of 25 mm and length of 10 mm.
Measurements performed on cropped 3D reconstructed CT images
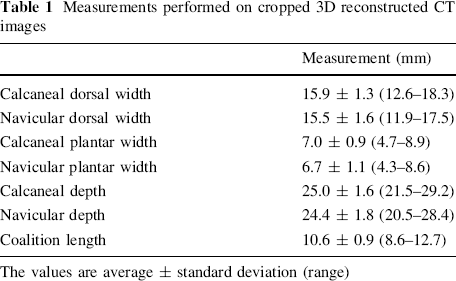
The values are average ± standard deviation (range)
Calcaneonavicular coalition classification
Analysis of the 3D anatomy of the calcaneus and navicular bones and their relationship to the talus and cuboid allowed for the classification of calcaneonavicular coalitions based on the appearance of the coalition and the shape of the cuboid. Figure 5 demonstrates representative images of cropped 3D reconstructions of the four distinct types of calcaneonavicular coalitions identified in this study, compared to normal.
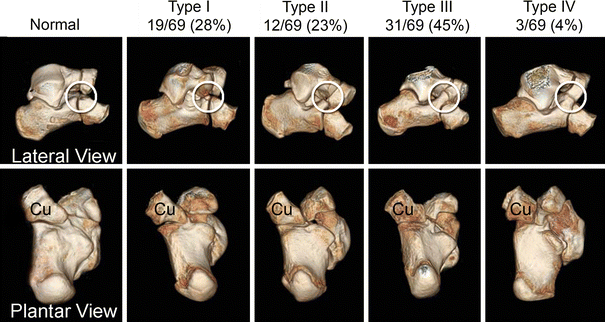
Classification system demonstrating the histopathologic continuum of a calcaneonavicular coalition (white circles) and the change in the shape of the cuboid (Cu). In the plantar view, the cuboid tongue or protrusion toward the calcaneus first becomes hypoplastic and then “squared off” as the coalition increases from a Type I to a Type IV (complete bony coalition)
The cortical borders of the calcaneus and navicular bones in the normal feet from the control cohort were noted to be smooth and clearly demarcated. Also, in the control cohort, the cuboid was noted to extend medially plantar to the calcaneus and navicular bones.
Nineteen coalitions (28%) were categorized as Type I or forme fruste variants. These coalitions were noted to have cortical irregularities at the tip of the calcaneus or had an ossicle present between the calcaneus and navicular bones. There was also noted to be slight blunting of the cuboid, as seen from the plantar view in Type I coalitions, compared to normal feet.
Sixteen coalitions (23%) were categorized as Type II or fibrous. Characteristic features of Type II coalitions included further blunting of the cuboid extension and narrowing of the non-ossified gap between the calcaneus and navicular bones.
Type III coalitions were present in a large proportion of the feet studied (45%). Near-complete or cartilaginous fusion between the calcaneus and navicular was present in this group, with a distinct “squaring-off” of the cuboid bone visible from the plantar view.
Finally, Type IV coalitions represent a complete osseous fusion between the navicular and calcaneal bones and were present in only 4% of the feet in our study. A dramatic change in the shape of the cuboid bone was observed in relation to the complete osseous coalitions, as the medially extending prominence present in the normal feet was no longer visible.
Clinical data
Physical examination and plain radiographs alone identified 24 patients with bilateral coalitions (65%). However, after all patients underwent CT of bilateral feet, an additional eight patients were found to have bilateral involvement (32/37 = 86%). Of the eight additional coalitions identified, magnetic resonance imaging (MRI) was performed on five patients to verify the presence of a coalition (Fig. 6). Three patients were found to have a cartilaginous ossification center present within a fibrous connection between the calcaneus and navicular bones (Type I coalition), while two patients had a small osseous extension of the calcaneus toward the navicular with a predominantly fibrous connection between the two bones (Type II coalition).

MR image of a Type II (fibrous) calcaneonavicular coalition (black circle)
Thirty-eight percent of the coalitions (26/69) were found to be asymptomatic and were incidentally found on physical exam, radiographs or CT. Out of these, most of them were classified as Type I (11) or Type II (9), and the remaining were classified as Type III (6). However, out of the 62% symptomatic coalitions (43/69), eight were found to be Type I, and seven were found to be Type II. Ten of these 15 non-ossified coalitions (4 Type I and 6 Type II) were resected surgically. Although post-operative follow-up of these patients was limited (4–6 months), all patients reported clinical improvement, with decreased pain and improved range of motion.
Discussion
Patients with calcaneonavicular coalitions commonly present to the hospital in adolescence, during the period of increasing ossification of the coalition, with vague ankle or foot pain after a minor traumatic injury [4]. Accordingly, in the current cohort of patients studied, the average age at presentation was found to be 13 ± 2 years. Several diagnostic modalities can be utilized to identify a calcaneonavicular coalition. On physical examination, pain localized to the sinus tarsi, diminished inversion and eversion of the subtalar joint, and rigid hindfoot valgus alignment can be indicative of a coalition. Peroneal spastic flatfoot can also be suggestive of a coalition [14–17], although various other etiologies must first be excluded. Numerous plain radiographic findings suggestive of a tarsal coalition have been described, including talar beaking on the lateral radiograph [18] and the “anteater nose” on a 45° medial oblique view [19]. Computed tomography, however, has recently become the imaging modality of choice for diagnosing a calcaneonavicular coalition [6, 9, 11].
The evaluation of 3D reconstructions of calcaneonavicular coalitions in this study enabled the identification of forme fruste variants, resulting in a greater number of patients that were found to have bilateral involvement (86%) than reported previously. With physical examination and radiographic evaluation alone, the authors have previously reported a bilateral calcaneonavicular coalition incidence of between 40 and 68% [4, 20]. CT evaluation, however, has been shown to result in the identification of more coalitions in the asymptomatic, contralateral foot. For example, Hochman and Reed reported a bilateral incidence of 75% for calcaneonavicular coalitions evaluated using CT [10]. However, the clinical importance of forme fruste variants should be considered. Our clinical data suggest that forme fruste variants should be recognized and that they should be treated in a similar fashion to the more osseous coalitions. Although many of the Type I and II coalitions may be asymptomatic on presentation, 3D CT data may provide the rationale for further evaluation of symptomatic forme fruste variants with MRI or surgical exploration.
The 3D CT analysis enabled the classification of the spectrum of calcaneonavicular coalitions. Historically, a coalition has been described as being either cartilaginous, fibrous, or osseous. However, the classification system presented in this study considers these categories as points within a histopathologic continuum [5]. Gradual changes from the “normal” variant to the Type IV (complete osseous) coalition were observed by CT; not only within the coalition itself, but also in the shape of the cuboid bone. As the coalition progresses from the forme fruste variant (Type I) to the fibrous coalition (Type II) to the near-complete coalition with a cartilaginous synchondrosis (Type III) to the osseous coalition (Type IV), the medially extending prominence or tongue of the cuboid appeared to become hypoplastic and eventually “squared off.” From the plantar view of the Type IV coalition, it appears as though the extension of the cuboid is “blocked” by the osseous bridge of the coalition. These anatomic relationships are important to consider when evaluating patients with persistent foot pain and a fibrous coalition that may be difficult to appreciate on plain X-rays.
The 3D CT analysis also allowed for the characterization of the curved wedge-shaped resection required in the surgical treatment of these patients. The widths of the calcaneal and navicular contributions to the coalition averaged about 16 mm on the dorsal surface, while the widths on the plantar surface were more than half that, or about 7 mm. Considering these dimensions, we recommend using a 5 mm straight Lambotte osteotome within the coalition to achieve a complete resection. A 10-mm-wide osteotome may be adequate on the dorsal surface of the coalition; however, near the plantar surface, where the average coalition width is only 7 mm, a 1-cm osteotome may damage the head of the talus or the cuboid (Fig. 7). Especially in forme fruste variants, care must be taken not to damage the medial extension or tongue of the cuboid plantar to the coalition. We also recommend using a Kerrison rongeur to ensure complete resection of the curved portion of the coalition that may be under the head of the talus and is not obviously visible from the dorsal incision.
Resection plane demonstrating the curved wedge shape of the coalition and relationship to the head of the talus and cuboid
The depth of the resection is also an important variable for preventing reossification of the coalition. As shown in this study, complete resection requires the removal of almost 25 mm (about 1 inch) of bone (Fig. 8). As demonstrated previously with cadaveric foot dissections [21], interposition of the extensor digitorum brevis (EDB) in a resected calcaneonavicular coalition is not recommended. Due to anatomic restrictions, the EDB muscle is not long enough and leaves a nearly 10-mm unfilled void at the base of the resection. Additionally, the use of the EDB commonly results in a large, cosmetically unappealing indentation in the sinus tarsi. Fat graft is abundantly available from the gluteal crease, or occasionally the abdomen, even in the most slender children. We recommend the use of fat to generously pack the 2.5 cm defect created by the coalition resection.
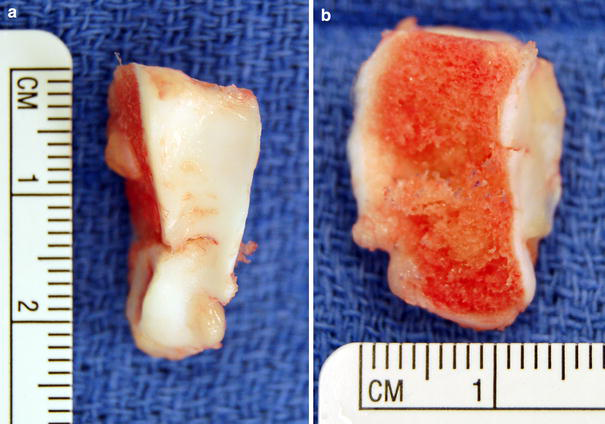
Intra-operative photographs of an en-bloc-resected calcaneonavicular coalition demonstrating a curved wedge shape with (
This study was limited due to its retrospective nature. For example, it is possible that a selection bias may have artificially increased the incidence of bilateral coalitions we observed. Additionally, in evaluating symptomatic forme fruste variants, not all Type I and II coalitions were evaluated with MRI, and the surgical follow-up for those treated with a resection was limited. This was, however, not the primary purpose of this study and will need to be evaluated in a future analysis. Finally, we presumed a normal calcaneonavicular relationship in the control cohort. As these patients presented to our institution with foot or ankle pain, it is possible that anatomic abnormalities of the foot were present and caused their symptoms; however, it would not have been ethically or financially responsible to obtain CT of bilateral feet on asymptomatic children.
In conclusion, 3D CT enabled the classification of the spectrum of calcaneonavicular coalitions. In Type I or II coalitions, the cuboid extended medially plantar to the fibrous connection, while in more complete Type III or IV coalitions, the cuboid was “squared off” and remained lateral to the osseous bridge. An understanding of the 3D anatomy is important when diagnosing milder forms of coalitions, and during surgical resection in order to avoid iatrogenic injury to the calcaneus, head of the talus, or cuboid. Furthermore, we confirmed the depth of the resection defect to be on average 25 mm, thus advocating fat rather than EDB muscle interposition.
Footnotes
Acknowledgment
This study was supported by the Children's Specialists Pediatric Orthopedic Fellowship and Education Fund.