
Abstract
Uterine artery pseudoaneurysm is a rare cause of secondary postpartum hemorrhage. Herein, we report a case of uterine artery pseudoaneurysm, with postpartum hemorrhage commencing 22 days after uncomplicated vaginal delivery. Intermittent bleeding occurred during conservative observation. Transvaginal ultrasound color Doppler imaging revealed swollen vascular structures that suggested arteriovenous malformations, and a saccular dilatation of blood vessels. However, it was insufficient to definitively diagnose the condition as pseudoaneurysm. Meanwhile, the three-dimensional computed tomography angiogram was effective in demonstrating a pseudoaneurysm in the uterus, and an absent early venous return sign, leading to the final diagnosis of a pseudoaneurysm. The patient was successfully treated with transarterial embolization using gelatin sponge pledgets. No bleeding or recurrence of the pseudoaneurysm was observed 2 months after embolization.
Keywords
Introduction
Pseudoaneurysms of the uterine artery are a rare cause of secondary postpartum hemorrhage. Etiologic factors of uterine artery pseudoaneurysms mostly involve patients’ history of uterine trauma, intrauterine manipulation, and both vaginal 1 and cesarean deliveries. 2 Some previous studies showed that some uterine artery pseudoaneurysm should be treated immediately and so early accurate diagnosis is mandatory. However, ordinary computed tomography (CT) or ultrasound sometimes did not provide an accurate diagnosis; this is partly due to their inability for illustrating the topological (three-dimensional (3D)) structure of the sac (pseudoaneurysm). Thus, we attempted to here illustrate the usefulness of 3D-CT for diagnosing this condition.
Case
A 24-year-old woman, gravida 1, para 1, with no past medical history had an uncomplicated vaginal delivery at 39 weeks of gestation in another clinic. During delivery, there were no complications, and the placenta came off smoothly with no need for manual removing. The amount of bleeding during delivery was 488 g, and the infant weighed 2426 g. The patient reported no medical or surgical history, including coagulation disorders. The patient visited the previous clinic with a complaint of vaginal bleeding at 22 days postpartum. On contrast-enhanced magnetic resonance imaging, placental polyps were suspected, for which she was referred to our hospital on the same day. On arrival to our department, her vital signs were as follows: blood pressure, 120/75 mm Hg; pulse, 73 bpm; respiratory rate, 15 breaths/min; and temperature, 36.4°C. On speculum examination, there was a small amount of bleeding. Laboratory tests showed normal serum hematocrit and hemoglobin levels. The white blood cell and platelet counts were also normal. Pelvic sonography revealed a blood-flow-rich mass extending from the endometrial cavity to the myometrium. Therefore, contrast-enhanced CT examination was performed to identify the source of bleeding. It showed a soft tissue mass with abundant vascular structures but with no obvious vascular leakage. A residual placenta was suspected, but the persistent bleeding ceased, and she was discharged. However, on the next day, she visited the hospital again due to rebleeding. Speculum examination showed vaginal blood retention, but no active bleeding. Transvaginal ultrasonography showed a mass of abnormal blood vessels with a mixture of arterial and venous flows in the uterine cavity (Figure 1(a) and (b)), suggesting uterine arteriovenous malformation (UAVM), and a saccular dilatation of blood vessels and “to and fro sign (yin-yang sign)” were observed on color Doppler (Figure 1(c) and (d)). Since it was difficult to differentiate UAVM from pseudoaneurysm based on the sonographic findings, we reconstructed the three-dimensional computed tomography angiography (3D-CTA) using thin-section CT images from the previous study to search for the cause of bleeding. This revealed dilated blood vessels in the uterus on the right side and an accompanying pseudoaneurysm with a diameter of 6.3 mm (Figure 2(a)). The early venous return sign, which is indicative of UAVMs, was not recognized. She was further observed conservatively but had repeated bleeding, and on the 27th day of puerperium, she underwent a new contrast CT examination and 3D-CTA. Since the pseudoaneurysm had grown to 12.7 mm (Figure 2(b)), interventional radiology hemostasis was performed to avert the rupture of the pseudoaneurysm. The dilated right uterine artery and pseudoaneurysm (Figure 3(a)) were embolized with gelatin sponge pledgets (Figure 3(b)). No bleeding or recurrence of pseudoaneurysm was observed at 2 months after embolization, and the reduction of the soft tissue mass was subsequently observed.

(a and b) Transvaginal ultrasonography showed a mass of abnormal blood vessels with a mixture of arterial and venous flow in the uterine cavity uterine cavity on color Doppler, suggesting uterine arteriovenous malformation. (c and d) Transvaginal ultrasonography showed a swollen blood vessel as well as “To and fro sign (yin-yang sign)” in color Doppler.
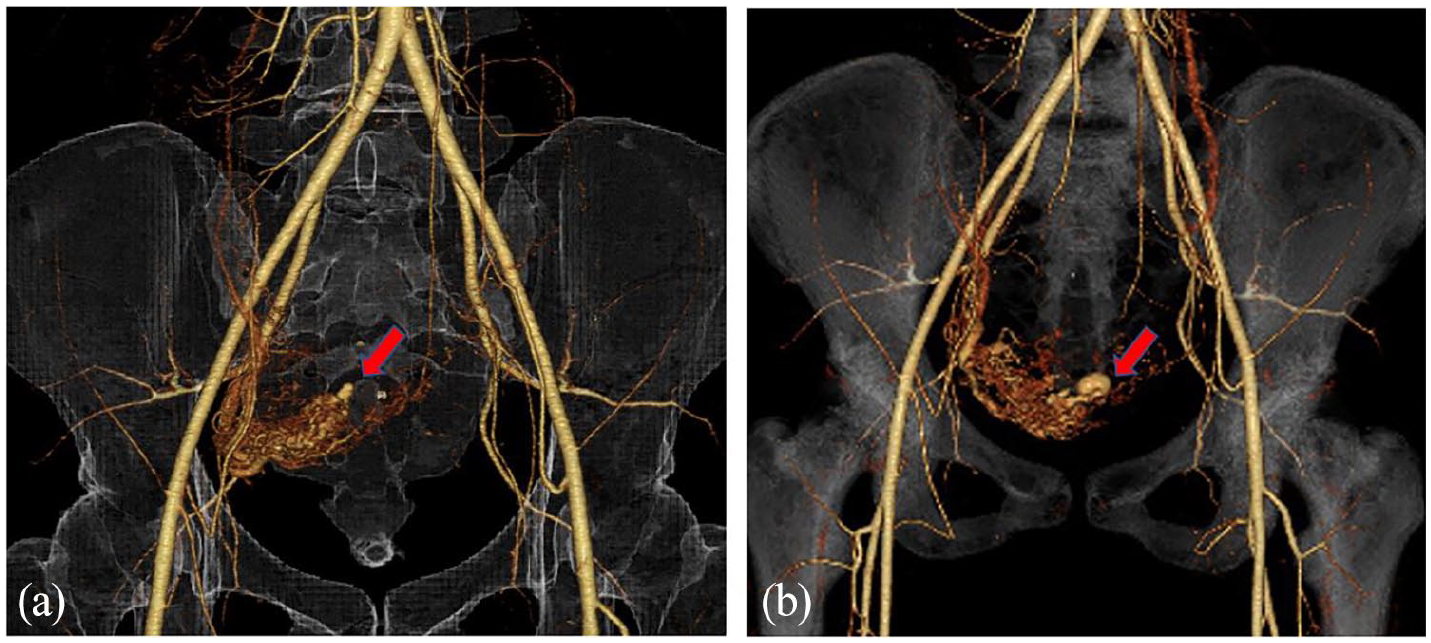
(a) 3D-CTA on the 22nd day of puerperium. A pseudoaneurysm 6.3 mm in diameter (red arrow) is recognized at the dilated right uterine arteries. (b) 3D-CTA on the 27th day of puerperium. The pseudoaneurysm grew to 12.7 mm in diameter (red arrow).
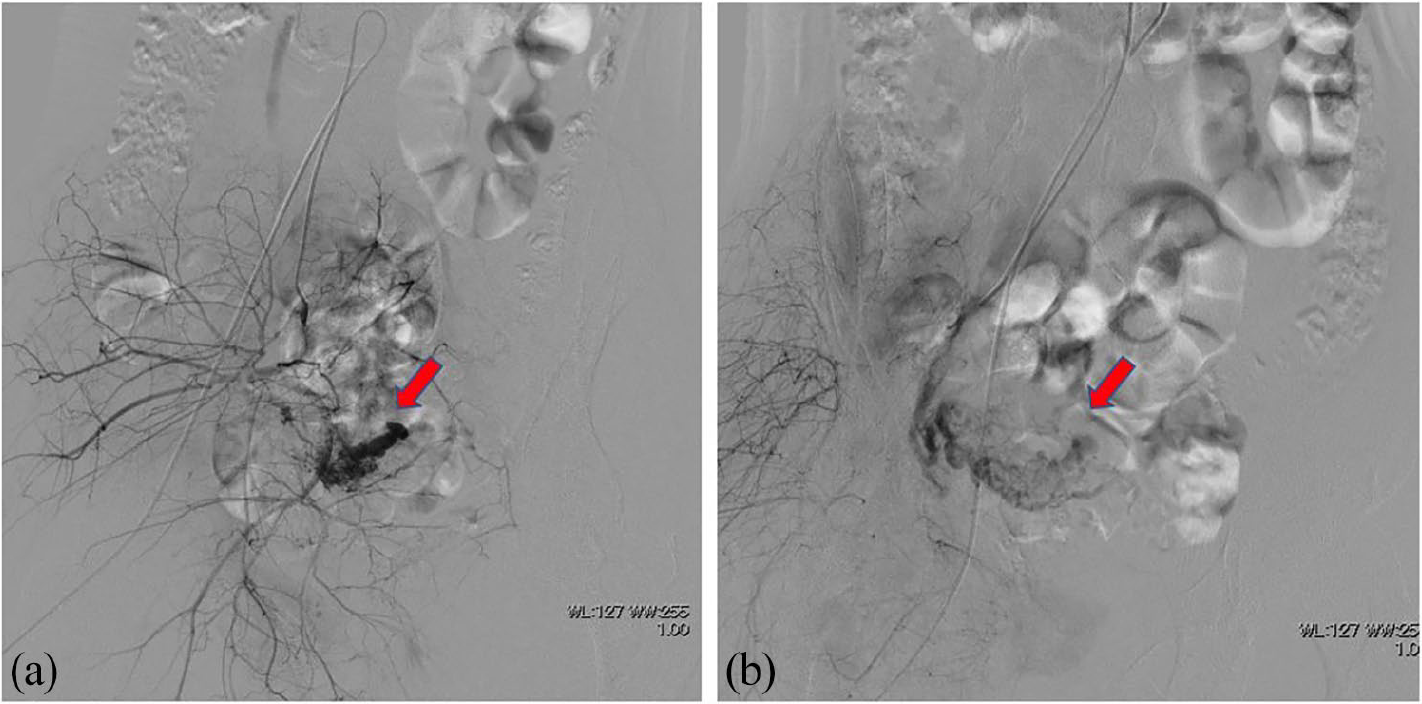
(a) Selective right uterine arteriography on 27th day of postpartum. The abnormally dilated right uterine arteries and pseudoaneurysm (red arrow) were embolized with gelatin sponge particles. (b) Right internal iliac arteriography after embolization. The right uterine arteries and pseudoaneurysm disappeared.
Discussion
Secondary postpartum hemorrhage, which occurs between 24 h and 6 weeks after delivery, usually results from retained products of conception, endometritis, or involution of the placental bed. 3 Uterine artery pseudoaneurysm is a rare cause of secondary postpartum hemorrhage. Pseudoaneurysms result from arterial wall laceration or puncture due to surgery or penetrating trauma, allowing blood to dissect into the periarterial tissues and create a perfused sac that communicates with the parent artery lumen. 4
It is crucial to accurately diagnose the cause of secondary postpartum hemorrhage because dilation and curettage for presumed retained products of conception could lead to fatal uterine bleeding. The diagnosis of pelvic pseudoaneurysm can be made using various imaging tests, but angiography remains the reference standard. Isono et al. 5 reported the definitive diagnosis of pseudoaneurysms using angiography (41.2%), computed tomography (CT) (29.4%), and color Doppler ultrasonography (29.4%).
In pelvic sonography, a pseudoaneurysm presents as a pulsating anechoic or hypoechoic structure connected to a parent artery by a small neck, with swirling blood flow on color Doppler images. 6 In our case, the pseudoaneurysm was not diagnosed confidently on color Doppler because the saccular hypoechoic area was continuous with the surrounding swollen blood vessels and the existence of a neck was ambiguous. Moreover, our findings were similar to UAVM, in which abnormal blood vessels are directly connected without intervening capillaries.
On ultrasonography, UAVM characteristically displays a subtle myometrial inhomogeneity with multiple distinct anechoic or hypoechoic spaces in the myometrium with no mass effect. On color Doppler, UAVM may present as an intense color in the myometrium with extensive color aliasing and apparent flow reversals. In our patient, color Doppler was insufficient to distinguish between the dilated arteries and veins, depict the direct connections between them, and exclude the possibility of UAVM.
Owing to the 3D reformatted images, CTA helped demonstrate the pseudoaneurysm and identify the feeding arteries. In addition, we were able to exclude UAVM using 3D-CTA because no early venous return sign was observed, which is probably an advantage of angiography over color Doppler imaging. We believe that blood vessel evaluation by 3D-CTA can be an effective and less invasive diagnostic imaging tool in future. However, its use should be restricted to highly selected patients, particularly for hemodynamically stable patients. We used high-quality CT equipment and optimized the radiation dose as low as possible.
Baba et al. 7 reported that some uterine artery pseudoaneurysm may not require transarterial embolization (TAE) at least immediately because it may resolve spontaneously. Thus, we waited for spontaneous resolution. However, surgical arterial ligation or hysterectomy may be required in patients with pseudoaneurysms if conservative treatment is not effective. Transcatheter embolization is safe and effective in treating postpartum bleeding. A recent study involving 588 patients with postpartum hemorrhage showed that pelvic artery embolization was effective in treating pseudoaneurysms, with a primary success rate of 94% and a secondary success rate of 100%. 8 Only one patient underwent repeated embolization, and no hysterectomy or arterial ligation was required in any case. 8 The existing literature shows that several agents can be used for pelvic arterial embolization in patients with postpartum hemorrhage, but gelatin sponge is the recommended embolic agent due to atony. 9
Conclusion
In conclusion, this case highlighted both the diagnostic advances in using 3D-CTA and the effectiveness of using gelatin sponge pledgets as a single embolic agent for uterine artery pseudoaneurysm.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.