
Abstract
Abstract
Purpose
The decision of whether or not to remove pediatric metallic implants remains a controversial issue. Many factors have been cited both in favor and against routine removal of metallic implants. The purpose of this study was to determine the fracture rate following the routine removal of hardware from patients with Legg–Calvé–Perthes (LCP) disease treated by proximal femoral varus osteotomy (PFVO) and to determine if there is an optimal time to remove hardware in this population.
Methods
We performed a retrospective chart review of children who had PFVO with subsequent hardware removal from March 1973 to May 2005 performed by a single surgeon. A total of 196 hips in 184 patients were included. Data was analyzed using logistic regression. Inverse prediction was also used to obtain estimates of the time needed to produce probabilities of no fracture.
Results
Ten out of the 196 hips included (5.1%) sustained a fracture after plate removal. The time from osteotomy to plate removal averaged 10.4 months in the nonfracture group and 4.8 months in the fracture group. This was statistically significant (P < 0.0001). Using the logistic regression model, the predicted time to plate removal corresponding to a 95% probability of no fracture was between 5.1 and 8.4 months.
Conclusions
Plate removal remains a reasonable choice but questions remain as to the timing of removal. These data suggest that patients may benefit from extending the time to hardware removal beyond radiographic union to at least six months or more after the osteotomy.
Introduction
Hardware removal is one of the most commonly performed pediatric orthopaedic procedures [1, 2]. Some series have described the indications for hardware removal to be related to the perceived risk of stress-risers above and below the plate [2, 3]. Despite the relative frequency of the procedure, objective evidence regarding whether or not to remove asymptomatic hardware is rare in the orthopedic literature [3–7]. Recent series have demonstrated that hardware removal results in uncomplicated healing in over 60% of cases [2]. While the Arbeitsgemeinschaft für Osteosynthesefragen (AO) recommends routine hardware removal, others have argued against it [1, 8, 9]. Complications of hardware removal include infection, blood loss, morbidity associated with second procedures, incomplete removal, and fracture [1–3, 6, 10, 11]. These complications, in some cases, may make the implant removal more morbid than the index surgery [3]. Kahle demonstrated that hardware removal about the proximal femur had the highest complication rate in their series [1]. In spite of these reports, it is customary at our institution to remove hardware after proximal femoral varus osteotomy (PFVO) with internal fixation. Postoperative fracture remains a difficult complication as it typically requires additional surgical procedures, casting, and/or hospitalization. In addition, there is a significant economic cost to routine removal of hardware [2, 3]. The amount of time to protect weightbearing after hardware removal in an active pediatric population has yet to be clearly defined. Furthermore, the timing of plate removal after radiographic union of the osteotomy is even less clear. In this study, we review the rate of fracture following PFVO performed by a single surgeon over a 32-year period.
Materials and methods
A retrospective chart review was conducted on cases treated by the senior surgeon (DSW). PFVO through a direct lateral approach was performed on a total of 196 hips in 184 patients (138 males and 46 females) with a diagnosis of Legg–Calvé–Perthes disease (LCP) from March 1973 to May 2005. The left hip was involved in 111 cases and the right hip in 85 cases. Osteotomy was performed at a mean age of 7.4 years with a range of 2.8–14.9 years. Plate removal was performed at a mean age of 8.2 years with a range of 3.3 to 16.0 years. Patients were kept nonweightbearing on the side of plate removal for two weeks with further weightbearing based on evidence of radiographic disappearance of screw holes. Data was analyzed using logistic regression with fracture status (no fracture, fracture) as the response and time (in months) from osteotomy to plate removal (time) as the predictor. For several probabilities of successful plate removal (no fracture), inverse prediction was used to obtain estimates of the time needed to produce those probabilities of no fracture. The analysis was performed with JMP statistical software (v.6.0.3; SAS Institute Inc., Cary, NC, USA, 2006).
Results
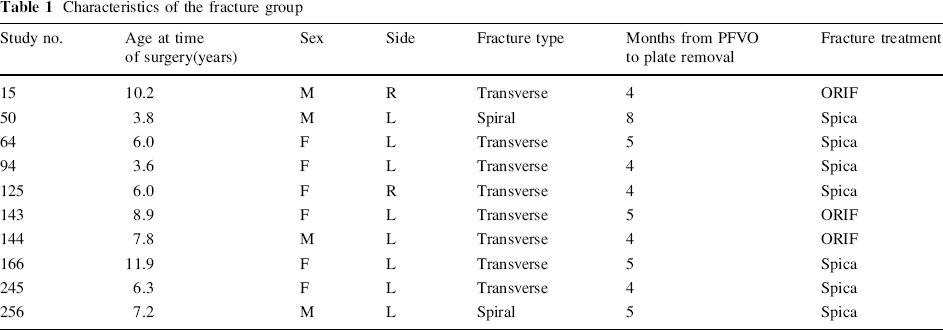
Out of 196 plate removal procedures performed, ten (5.1%) experienced a postoperative fracture (Table 1). Patient follow-up after plate removal averaged 6.2 years with a range of 0.5–26.9 years. Postoperative fractures occurred in six females and four males. The left hip was involved in eight of the fractures and the right in the remaining two. Of the ten fractures, eight were transverse through the osteotomy site, and two were spiral fractures through screw holes (Figs. 1, 2). A variety of fracture mechanisms was observed, ranging from falls to twisting injuries. Seven fractures were treated with reduction under general anesthesia and spica casting, and three were treated with open reduction and internal fixation.
Characteristics of the fracture group

Transverse fracture through osteotomy (4 years old)

Spiral fracture originating in a screw hole (6 years old)
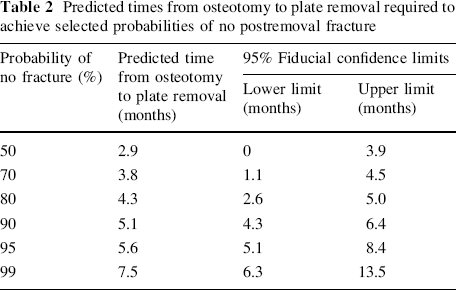
The time from osteotomy to plate removal averaged 4.8 months (95% confidence interval: 3.8, 5.6 months) for those patients that experienced a fracture and 10.4 months (95% confidence interval: 9.0, 11.7 months) in those that did not. This was statistically significant (P < 0.0001). The logistic regression analysis revealed that the probability of a successful plate removal (no fracture) increased with time (P = 0.004). For any given waiting time between surgery and plate removal, waiting an additional month increased the odds of no fracture by 170% (OR = 2.7). In other words, if an additional month is waited, the odds of no fracture are 2.7 times what they were if the additional month was not waited. To determine the time to wait between surgery and plate removal that is needed to have a reasonable probability of success (no fracture), an inverse prediction of the specified probabilities of success was conducted using the logistic regression model. Predicted times and their 95% fiducial confidence limits were computed for the following probabilities of successful plate removal: 50, 70, 80, 90, 95, 99% (Table 2).
Predicted times from osteotomy to plate removal required to achieve selected probabilities of no postremoval fracture
Discussion
The issue of whether routine hardware removal is the preferred choice remains unanswered by this or other papers. Our data does suggest that routine metal removal at the proximal femoral level in the pediatric population is reasonable. Our fracture rate of 5.1% compares favorably with the current literature regarding implant removal about the hip [2]. Some previous studies on hardware removal about the pediatric hip have been done in a cerebral palsy population [10]. The incidence of postoperative fracture would certainly be expected to be higher in our population of more active and ambulatory patients.
Bankes et al. demonstrated that a high percentage of LCP patients will go on to require total hip arthroplasty in future [12]. Retained metal may create distant technical difficulties at the time of reconstruction. Removal of this hardware at the time of arthroplasty may add significant morbidity and time to the operative procedure. A recent instructional course lecture regarding total hip arthroplasties for the dysplastic hip recommends removal of all hardware about the hip after it is has served its purpose for the aforementioned reasons [13].
Although healing times after PFVO performed at different levels were not compared, the subtrochanteric operative site has been utilized for over 20 years with routinely good radiographic results [14, 15]. Radiographic healing is generally complete by 3–4 months postoperatively. Fracture after plate removal after intertrochanteric osteotomy was not studied in this paper.
Our results also demonstrate that patients may benefit from increasing the time period from PFVO to plate removal. Patients who did not experience a fracture in our study had their plates removed on average 10.4 months after the osteotomy. Those that experienced a fracture had their plates removed on average 4.8 months after osteotomy. This was a significant difference (P < 0.0001). Our analysis suggests that each additional month allowed to elapse before plate removal nearly triples the chances of a successful outcome (OR = 2.7). Using our logistic regression model, we predicted the time to plate removal corresponding to a 95% probability of no fracture to be between 5.1 and 8.4 months (95% fiducial confidence limits) (Table 2). The upper limit of 8.4 months may be a reasonable recommended waiting time, since it is unlikely that it would be necessary to wait longer than this to achieve a 95% probability of no fracture. This amount of time would extend well beyond evidence of radiographic healing of the PFVO. It is highly likely that internal remodeling at the osteotomy site is occurring for a period of 1–2 years after the index surgery.
While the AO recommends 18–24 months between plating and subsequent removal in adults, plates in the pediatric population are typically removed much earlier [9]. Additionally, while the envelopment of a plate in bone is not a concern in the adult population, it occurs frequently in children [12] (Figs. 3, 4). While studies involving screw holes in dogs have shown remodeling as soon as four weeks, human studies have shown that it takes as long as 18 weeks to completely remodel screw holes [16]. Based on our data, it would appear that delaying hardware removal in our population allowed for sufficient internal remodeling to avoid subsequent fracture through the osteotomy or screw holes. It would stand to reason that patients would benefit from extending time to hardware removal beyond radiographic union of the osteotomy to at least six months or more after the index procedure. The only other paper in the literature that we are aware of that recommends at least six months to hardware removal in the pediatric population is from Becker and coworkers, on patients with cerebral palsy [10]. Additionally, we believe that this is the first paper in the literature to use a statistical model to validate the “six month rule.” The 5.1% fracture rate in this large series of patients is coincident with the literature and can likely be reduced in the future.

Bilateral plate envelopment at skeletal maturity

Attempted surgical removal aborted due to envelopment
Conclusion
The fracture rate after routine hardware removal in a large LCP patient population undergoing PFVO with plate and screw fixation of 5.1% is coincident with the literature, but a lower rate can be anticipated upon delaying removal until at least six months or more after the index procedure.
Footnotes
Acknowledgments
The authors wish to thank Mrs. Adeline Weiner for clerical assistance in the preparation of this paper.