
Abstract
Background:
The newborn transphyseal fracture of the distal humerus is frequently misdiagnosed with an elbow dislocation due to the absence of the lateral condyle ossification node. No consensus has been reported either for the diagnosis or the management of these rare fractures. This study aimed to analyze a series of newborns with transphyseal distal humerus fractures.
Methods:
All consecutive infants treated between 2005 and 2020 for a transphyseal fracture of the distal humerus before the age of 6 months were retrospectively included. All radiological examinations were analyzed (X-ray, ultrasound, and magnetic resonance imaging (MRI)) as well as the therapeutic management (orthopedic or surgical treatment). The patients were seen at outpatient clinic visits with a minimum of 2-year follow-up.
Results:
Nine newborns were treated. The main cause was an obstetrical traumatism (n = 8). The diagnosis was made on physical examination and addressed by obstetric departments with standard biplanar radiographs in four cases. The fracture was suspected on physical examination in the remaining five cases and confirmed by complementary imaging (ultrasound (2), MRI (1), and both (3)). A total of six patients were treated conservatively and three surgically with an open reduction. At a mean follow-up of 79 months, two complications occurred: one axillary abscess due to the cast and one cubitus varus deformity. All children had a full functional recovery.
Conclusions:
The transphyseal fracture of the distal humerus in newborns is a rare entity that should be managed conservatively. Additional imaging examinations are recommended to clarify the diagnosis.
Level of evidence:
Level IV, cohort study.
Introduction
Newborn transphyseal fracture of the distal humerus, corresponding to Salter and Harris type I fractures, is a very rare entity that occurs in less than 0.00001% of births. 1 This fracture seems to occur during difficult deliveries and in both cesareans and vaginal extractions. However, the exact mechanism leading to this injury is still unknown. The literature is rather poor and mainly composed of case reports, the largest study including six patients. 2 One recent review by Ratti et al. confirmed the heterogeneous management, in either the diagnosis or treatment, with short-term follow-up (mean of 22 months) studies. 3
The distal humerus of the newborn is not ossified at this age, and the injury is frequently misdiagnosed. Standard radiographs can show indirect signs, such as joint effusion and displacement of the proximal forearm, frequently confounded with an elbow dislocation. Other imaging techniques have been used to confirm the diagnosis: ultrasound, magnetic resonance imaging (MRI), and arthrography.3 –10,11 Each of these requires specific training to be performed and interpreted correctly in the newborn. The second difficulty is that there is no consensus regarding the therapeutic management of these fractures. Both conservative orthopedic treatment (immobilization with safety pins attached to the bodysuit), with or without prior reduction, and surgical treatment (closed or open surgeries) have been reported in the literature.2,3,12–16,11 If not treated, complications are limited range of motion either in flexion and extension or in prono-supination, elbow malunion in cubitus varus, and persisting pain, requiring further surgeries in the long term.
Therefore, this study aimed to report results from a newborn cohort of transphyseal fractures to guide physicians in the management of these injuries.
Materials and methods
Study population
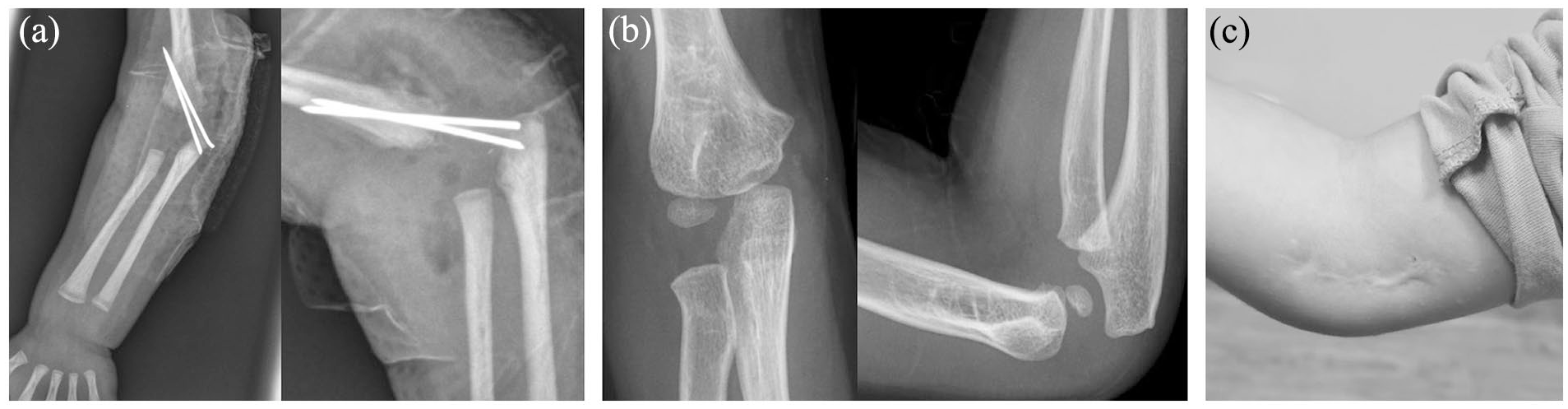
After IRB approval (CEER2023-724), a retrospective, monocentric case series study, including all consecutive transphyseal Salter and Harris type I distal humerus fractures, was conducted between 2005 and 2020. Search terms in the institutional coding system for diagnosis were “elbow dislocation” and “distal humerus fracture.” Inclusion criteria were as follows: (1) patients aged 0–6 months, (2) without ossification of the distal humerus metaphysis, and (3) with a minimum of 2-year follow-up. The aspect of “elbow dislocation” on the initial X-ray reflects the displacement of the proximal forearm (Figure 1). Ultrasound and/or MRI were used to confirm the diagnosis (Figures 2 and 3).
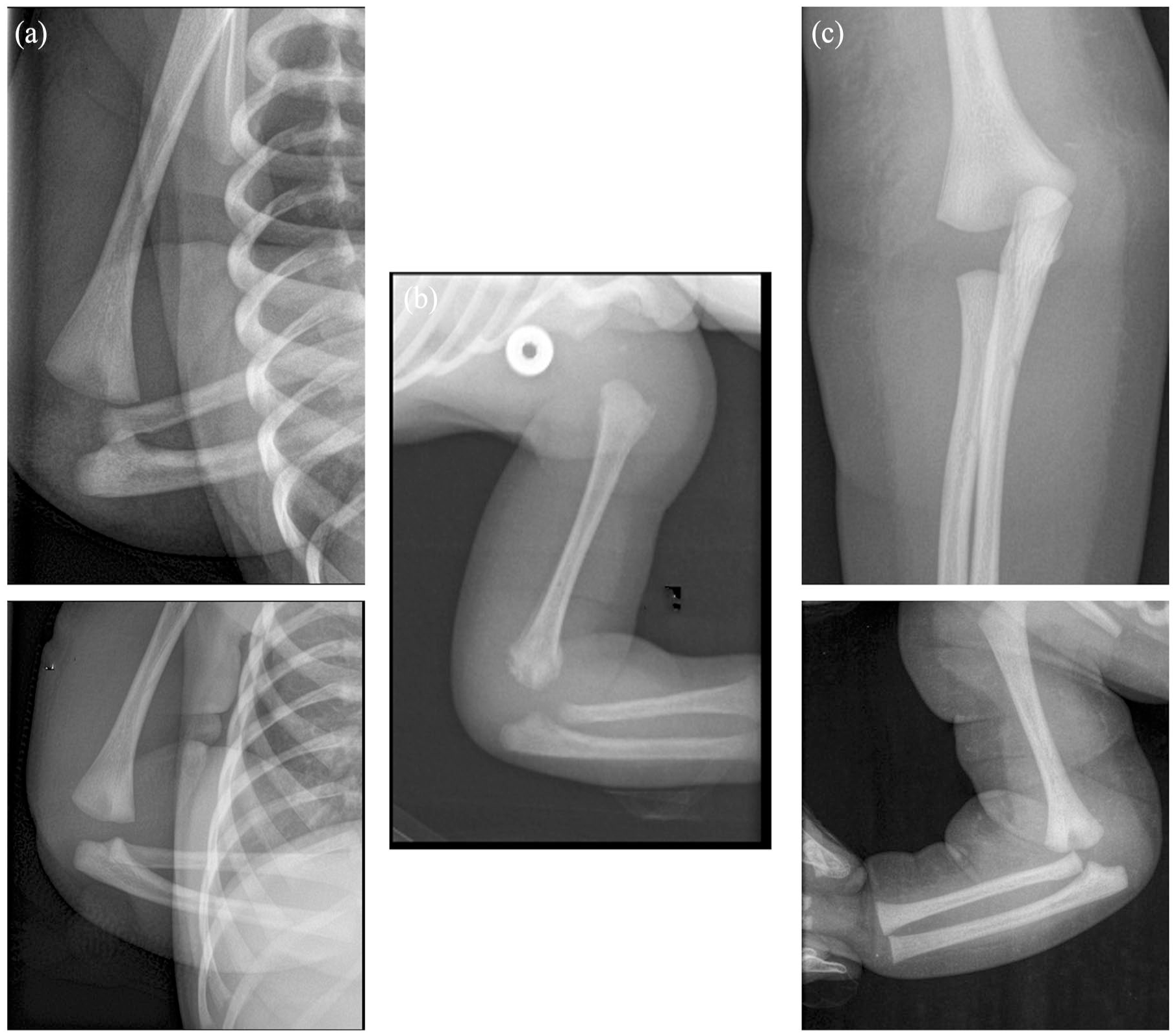
Anteroposterior and lateral sides X-rays show the forearm displacement and the so-called “elbow dislocation”: (a) patient 1 with a Gartland III fracture for whom the displacement was diagnosed on the ultrasound; and (b) patient 3 with a Gartland IV fracture identified on the MRI: (c) patient 9 with a Gartland IV fracture reduced under general anesthesia.
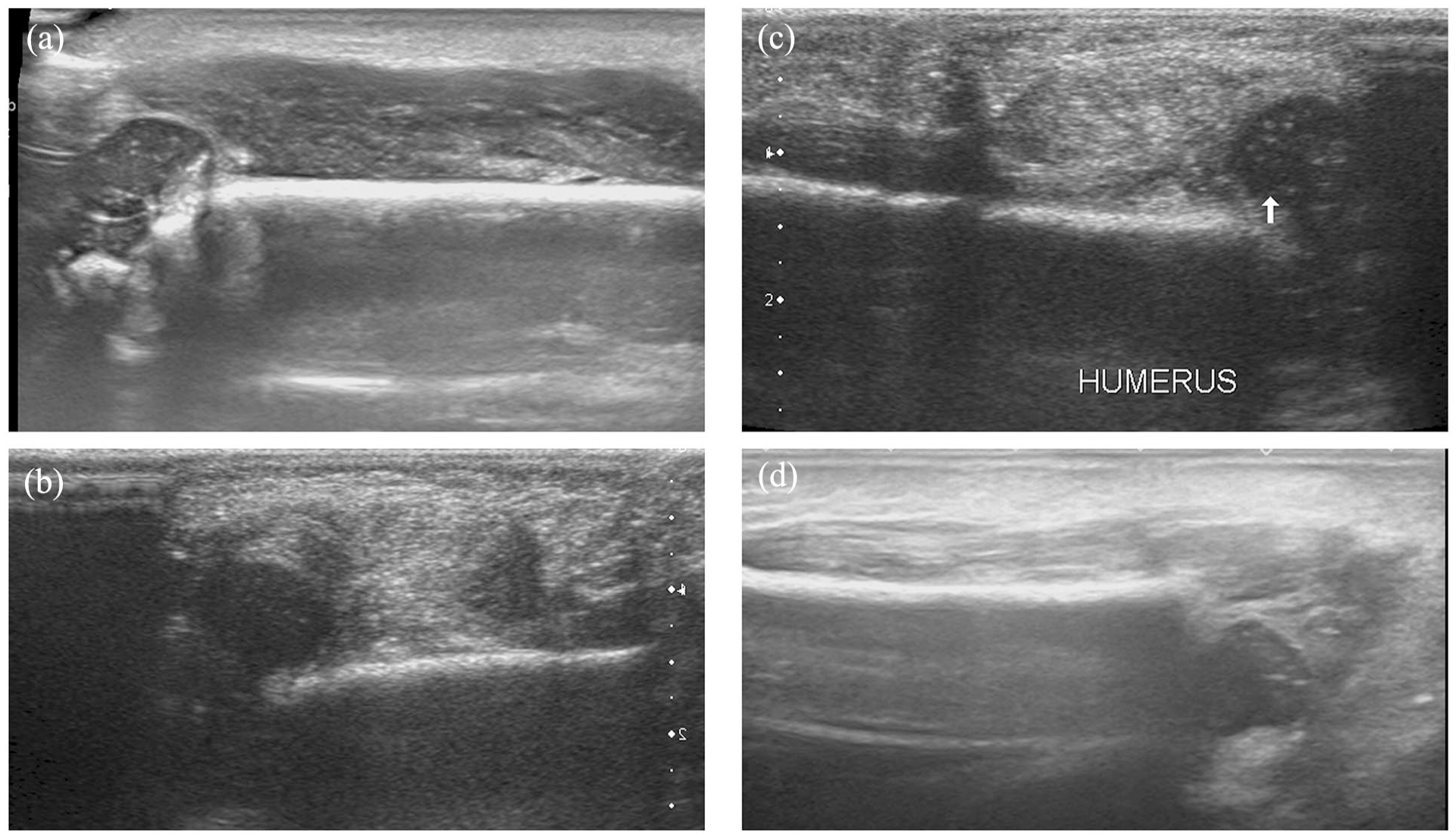
Illustration of the different initial ultrasounds shows a persistent contact between both sides of the fracture in patient 2 with a Gartland II fracture (a). (b), (c), and (d) illustrate patients 4, 5, and 9 who had severe displacement of the fracture. Patients 4 and 5 had an open reduction and patient 9 was reduced under general anesthesia.
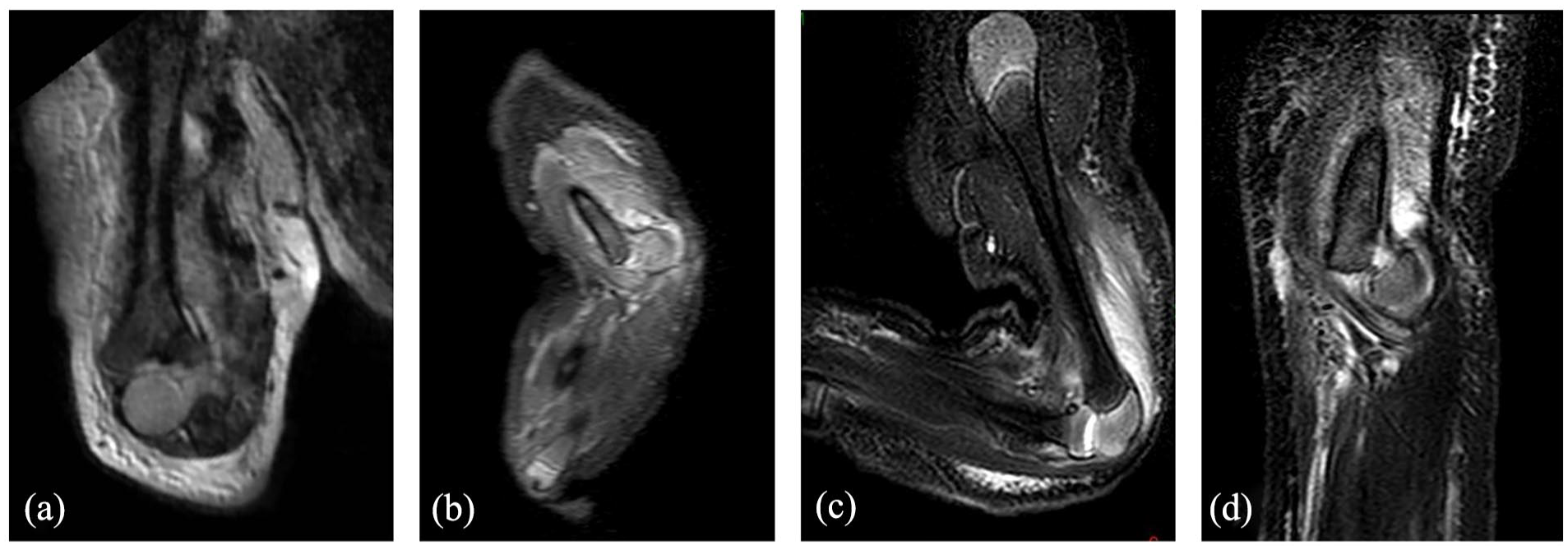
Illustrations of initial MRIs. (a) Coronal view of patient 3 showing a 90° rotation of the distal humerus; (b) a sagittal view of the severe displacement for patient 5 treated by an open reduction; and (c) and (d) view of patients 7 and 8 who were treated orthopedically.
Diagnostic strategy
All the patients were referred to our pediatric orthopedic department for a swollen and painful elbow with functional impairment. X-rays were performed in the obstetrics department in some cases. Upon their arrival, a physical examination was achieved before any further investigations by an orthopedic surgeon to eliminate septic arthritis. Complementary investigations were performed: ultrasound and/or MRI to classify the degree of displacement according to the Gartland classification. No general anesthesia or sedation was necessary for the MRI since it was performed just after feeding the newborn or after the administration of oral 5% glucose, so the newborn was calm and cooperative (Figure 3). X-rays, ultrasound, and MRI were all interpreted by a trained and senior pediatric radiologist and an orthopedic surgeon.
Treatment
Both orthopedic and surgical treatments were performed in the current cohort based on the severity of the displacement. The orthopedic treatment consisted of the immobilization of the elbow with the long arm of the bodysuit fixed with two safety pins to the bodysuit (Figure 4). If the initial displacement was considered unacceptable (Gartland IV), reduction under general anesthesia was attempted and open reduction with internal fixation (ORIF) by two Kirschner wires was performed if the radiological result after closed reduction maneuvers was not satisfactory (Figure 5). No arthrography was performed. The removal of the wires and the immobilization was done 4 weeks later.
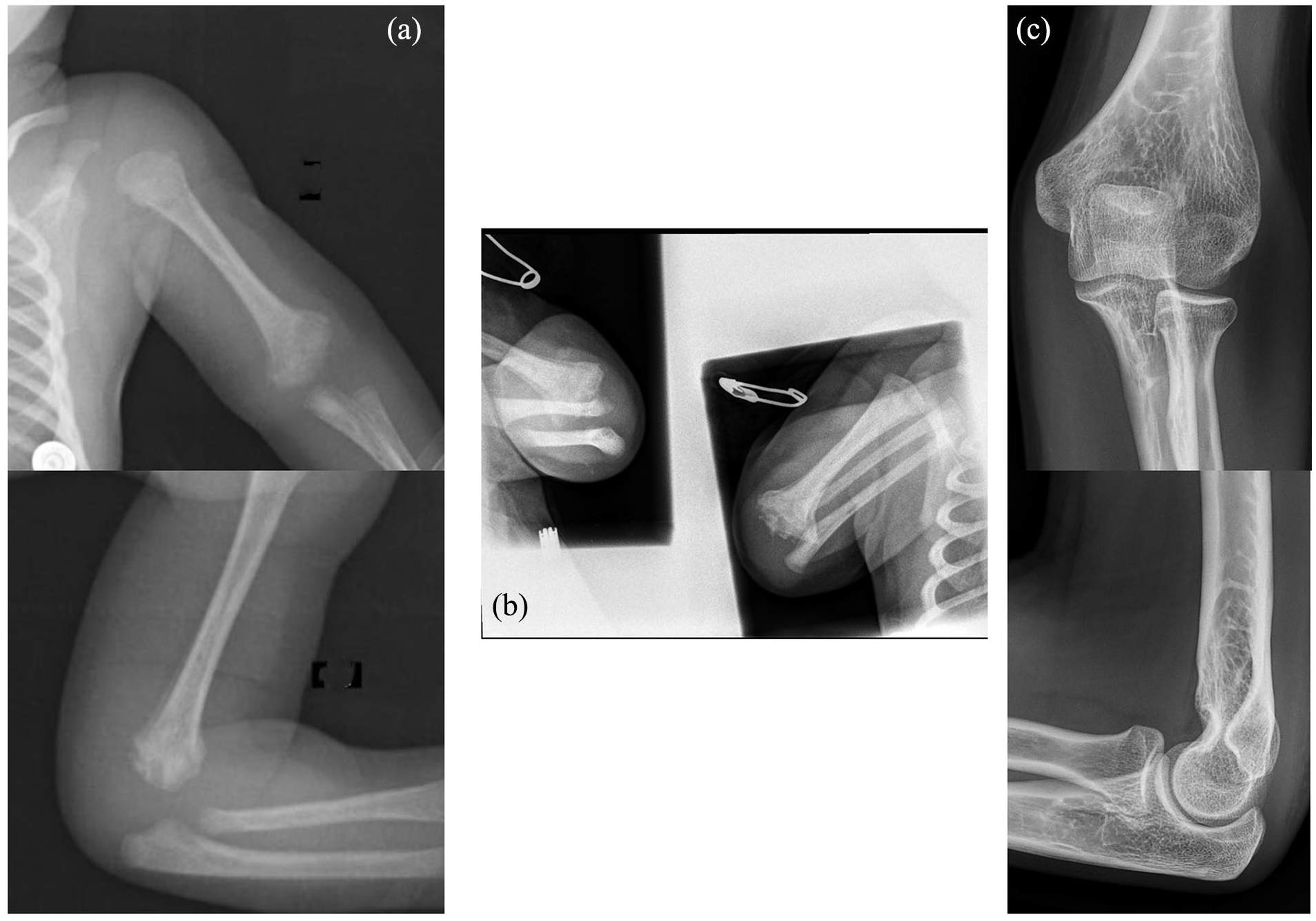
Twelve-day-old X-rays (a). The patient was treated conservatively with the arm attached with two safety pins to the bodysuit for 4 weeks as illustrated on the biplanar X-rays performed after reduction (b). After 13 years, the fracture was consolidated without complication (c).
Postoperative X-rays of a 9-day-old patient treated surgically by an ORIF (a). At the age of 4.5 years, the fracture was consolidated without complication (b). The scar was a Vancouver type 3 (c).
Follow-up period
The children were seen in outpatient clinic visits at regular intervals (4 weeks, 6 weeks, 3 months, 6 months, and 1 year) and then every 2 years. At each outpatient visit, the examination consisted of the evaluation of the elbow motion and the presence of a malunion. Biplanar X-rays were also performed. An aspect of the scar was assessed by the Vancouver Scar Scale. 17 This is a 13-point scale that considers vascularity, pigmentation, elasticity, and scar height. The lower the score is, the more satisfactory the appearance of the scar is.
Results
Population
Between 2005 and 2020, nine newborns have been managed for a transphyseal fracture of the distal humerus (Table 1). No ischemia or palsy was reported prior to treatment. In eight cases, the cause of the fracture was caused by the delivery, and the fracture was diagnosed in the first 10 days after birth. The average birth weight was 3300 g, ranging from 2020 to 4020 g. Only one newborn was considered a macrosomic child. Three of them were delivered with a cesarean section (C-section). Difficulties during birth were reported by the obstetricians in two out of the eight obstetrical cases (patients 3 and 4). Patient 3 was delivered by C-section and the obstetricians reported manipulating the right upper limb during the extraction. Patient 4 was delivered vaginally (twin pregnancy) in a breech presentation during which a Lovset and Mauriceau maneuver was necessary for the extraction.
Population characteristics.
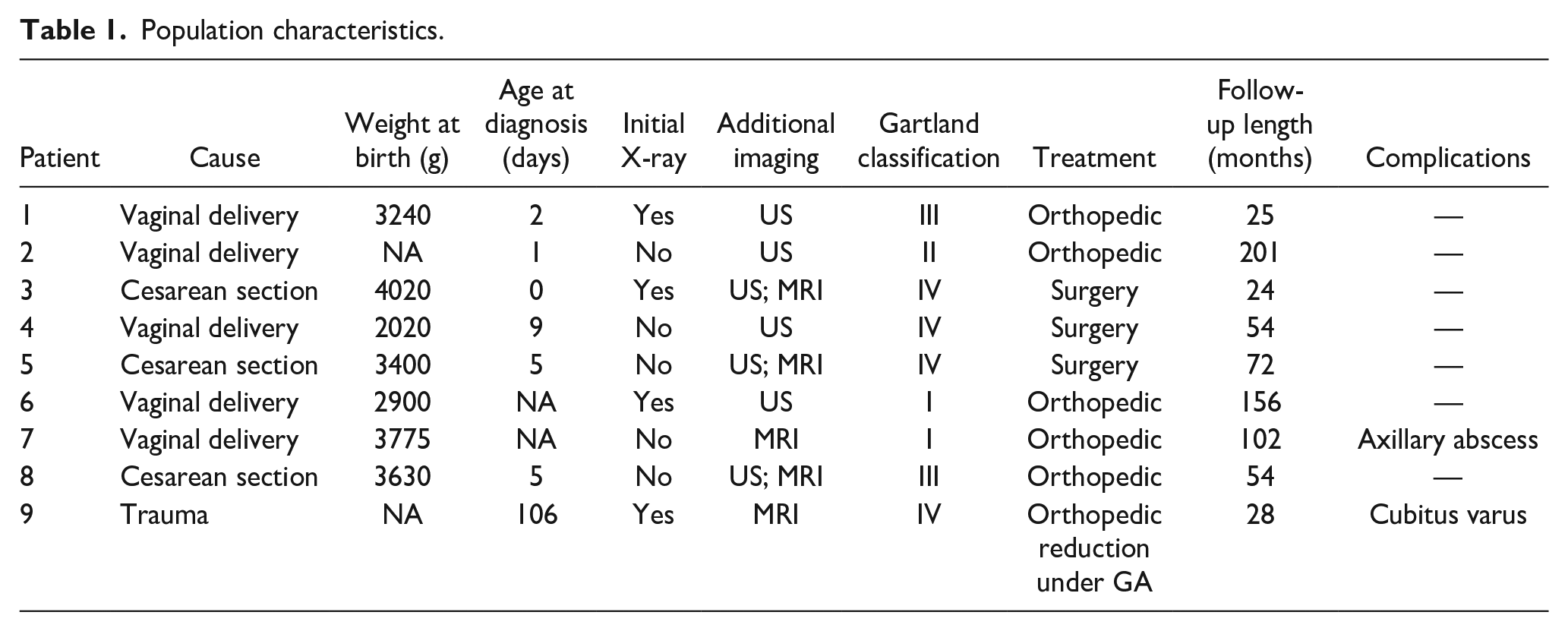
The last infant was diagnosed with a transphyseal fracture of the distal humerus at the age of 3 months secondary to a fall from the sofa.
Diagnosis management
The mean time to diagnosis after birth was 4 days for the eight obstetrical cases, ranging from 0 to 9 days. The clinical signs that led to suspect an upper limb fracture were a “pseudo paralytic” arm associated with hematoma and major swelling, or an obvious discomfort and functional impairment at mobilization. No blood test was running to diagnose a potential elbow septic arthritis.
Initial radiographs showed a displacement of the proximal forearm in four patients (Figure 1) and the ultrasound and MRI performed confirmed the diagnosis in all the cases.
Treatment management
Six out of nine newborns were treated orthopedically, one being reduced under general anesthesia (Figure 4). Three children were managed surgically by open reduction and internal fixation (Figure 5). One complication occurred in patient 7, treated orthopedically. The patient developed an axillary abscess due to the immobilization and required surgical drainage at the age of 1 month. The outcome was favorable.
Follow-up and complications
The average age at the last follow-up date was 6.5 years (mean follow-up of 79 months). At the last outpatient visit, no child had residual pain and all the patients had a complete joint range of motion without any limitations. The average Vancouver score was 2 for treated children, which is a good cosmetic result (Figure 5). There was no case of non-union. One case of malunion was found in patient 9, who developed a cubitus varus (22°) at the age of 18 months.
Discussion
This study is the largest cohort of patients with a transphyseal fractures of the distal humerus in neonates reported in the literature and with the largest follow-up. Even though this fracture is extremely common in older children, accounting for 15% of all pediatric fractures, this is not the case in neonates. Indeed, among the 1893 transphyseal fractures of the distal humerus treated surgically in our institution during the same period, the one occurring in newborns was very rare (0.5%).
Diagnosis management
In front of a painful and swollen elbow after birth, patients should be immediately addressed to a pediatric orthopedic surgery department. The diagnosis is based above all on the physical examination. Pediatricians should be alerted if a newborn seems to barely mobilize the upper limb or seems to be uncomfortable. Each joint, including the elbow, should be carefully examined for obvious deformity, edema, or ecchymosis. Passive mobilization is always painful. In this case, the current authors recommend a biplanar X-ray. The most obvious indirect sign is a pseudo-dislocation of the elbow with the displacement of the proximal forearm. The main differential diagnosis is obstetrical brachial plexus palsy, but the latter is not painful. 18 The second differential diagnosis is septic arthritis, but the complementary imaging performed in all cases confirmed the diagnosis. After birth, in children under 6 months of age, there are no more specific signs, but a context of maltreatment should always be sought.
Complementary radiological exams
Due to the absence of ossification of the distal humerus at this age, X-rays provide very little information about the fracture. Moreover, it is impossible to assess the extent of displacement and the persistence of bone contact. The only indirect sign is the “elbow dislocation” which indeed reflects the severity of the displacement. These elements are nevertheless important and must be considered to classify these patients, based on the older patient’s classification. 19 Nonetheless, some authors have reported the risk of misdiagnosis with elbow dislocation but there is no evidence in the literature to support the existence of this entity in neonates.3,16
Complementary radiological examinations are, therefore, mandatory (ultrasound, MRI, or arthrography).2,5,9,10,14,15 In the current study, ultrasound and MRI were performed solely in five out of nine newborns. Ultrasound and/or MRI are now systematically performed in those cases in the current institution. Ultrasound is an examination that is easily accessible, is not expensive, and does not require sedation and/or anesthesia. However, it must be performed by a senior radiologist used to young children since there is pain in this condition with frequent difficulties during the examination. MRI has the advantage of being a cross-sectional imaging technique, less dependent on the operator, and not painful for the child. However, it might require sedation or anesthesia, as reported in the literature.2,6 However, in a pediatric institution, it is possible to perform this examination without any sedation, which was the case in the current study.8,13 The patient should only be fed just before the examination. No arthrography was performed in the current study and might be at risk of infectious arthritis. However, it might be useful when a closed reduction is performed under general anesthesia to verify if the reduction is correct (Figure 6).
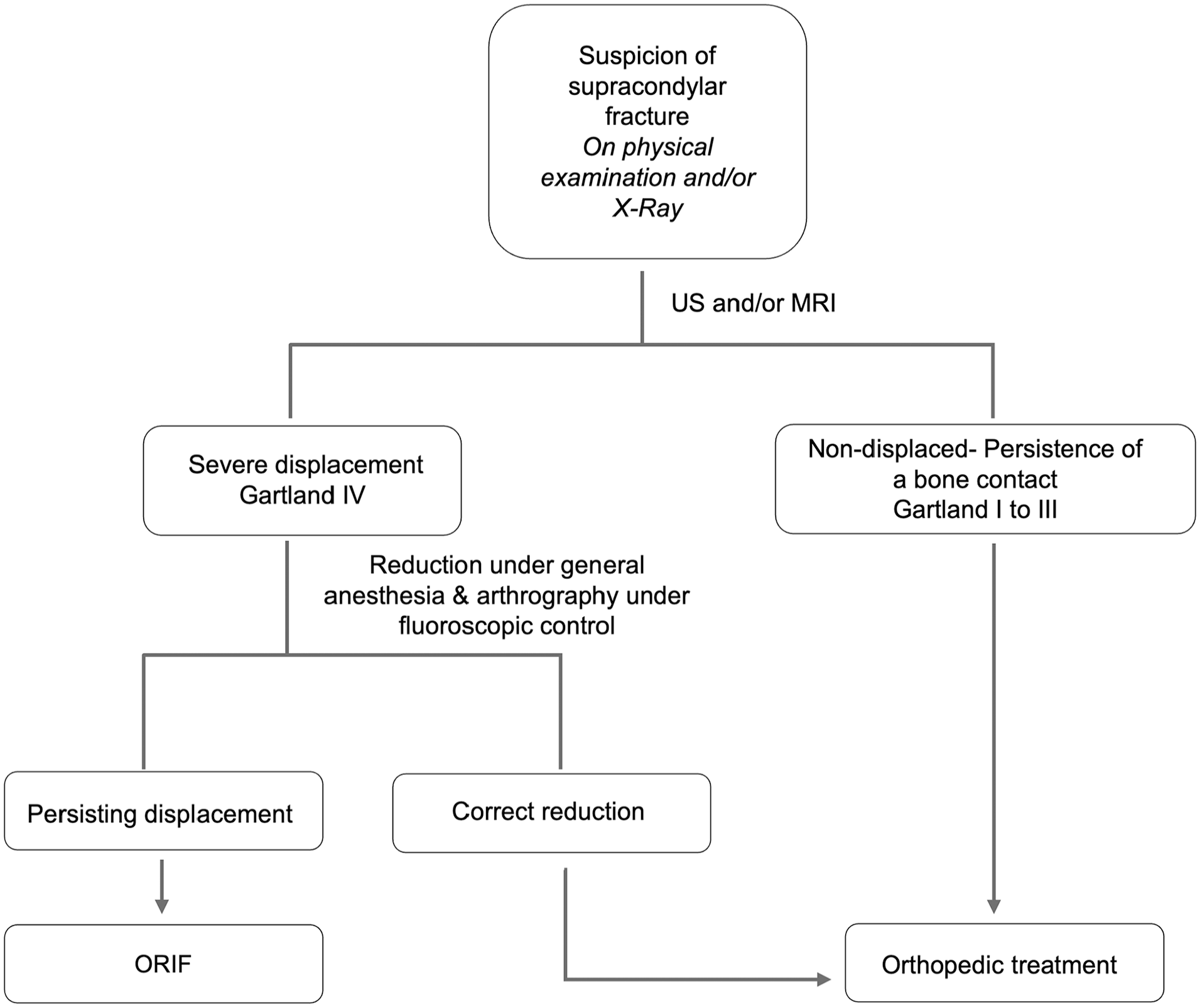
The flowchart illustrates the recommendations for the management of those fractures.
Therapeutic management
The rate of surgery was higher (33%) in the current study compared to the literature (12%). 3 This disparity can be explained by the lack of consensus regarding the management of these injuries. The orthopedic treatment gives good results and is well tolerated at this age regarding the length of potential bone remodeling in such young children, even though it concerns 20% of the humerus. However, this treatment cannot control the transversal displacement, which is not monitored on the X-rays due to the absence of ossification (Figure 3(a)). In the current study, complications occurred in children treated orthopedically (patients 7 and 9). Surgical treatment should therefore be considered and based on the degree of displacement assessed by the complementary radiological exams.
However, even though no complications were reported in the current cohort, surgery is not without risk. First, it requires general anesthesia with the risk of laryngeal spasm. 20 The medial approach of the elbow, used presently, might have exposed them to an ulnar nerve palsy. There is also a risk of surgical site infection. Finally, depending on the quality of wound healing, there might be a cosmetic impairment even though there were good results in the current study (Figure 5).
Recommendations for management and treatment
Based on the current results, the authors’ recommendations are summarized in a flowchart (Figure 6). Even though no arthrography was performed in the current study, it can be proposed in the cases of patients for whom a reduction under general anesthesia is performed and with a persisting doubt regarding the quality of the reduction.
Limitations
This study has several limitations. It is a retrospective, descriptive, and non-comparative study. Although it is one of the largest series, the number of children was small. In addition, not all children underwent complementary imaging such as ultrasound or MRI. Management in the current pediatric orthopedic department has evolved, and one of these radiological examinations is being systematically performed. Finally, the only child with a chronic complication in the current study (cubitus varus) was a child treated orthopedically. However, it was one of the children with the lowest follow-up and the next evaluation might show better results.
In conclusion, transphyseal fracture of the distal humerus of the newborn is a rare entity that should be investigated in case of clinical anomalies at birth. Standard radiographs should be completed by an ultrasound and/or an MRI to confirm the diagnosis and to evaluate the degree of displacement. Although this study was not comparative, orthopedic treatment should be priorly considered and gives satisfactory consolidation for the child at skeletal maturity
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241278166 – Supplemental material for Management of the supposed elbow dislocation in newborns
Supplemental material, sj-pdf-1-cho-10.1177_18632521241278166 for Management of the supposed elbow dislocation in newborns by Florian Kruse, Frederique Dizin, Brice Ilharreborde, Pascal Jehanno, Anne-Laure Simon and Virginie Mas in Journal of Children’s Orthopaedics
Footnotes
Author contributions
V.M. and A.L.S. Conception and design; A.L.S. Administrative support; P.J. and B.I. Provision of study material and patients; F.K. and F.D. Collection and assembly of data; F.K., F.D., and V.M. Data analysis and interpretation; F.K., F.D., B.I., P.J., A.L.S., and V.M. manuscript writing; F.K., F.D., B.I., P.J., A.L.S., and V.M. final approval of the manuscript.
Availability of data and material
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE uniform disclosure form. BI declares to be a consultant for Zimmer Biomet, Medtronic and Implanet. The other co-authors have no conflict of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Robert Debré (Comité d’évaluation de l’éthique des projets de recherche de Robert Debré, CEER-RD) (CEER2023-724) on July 18th, 2023. No specific consent is needed for statistical analyses of aggregated de-identified data. For this study, the raw data were first extracted from HIS, and patients’ identities, including names, screening IDs, patient IDs, and mobile phone numbers, were de-identified.
Ethical approval
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.