
Abstract
Abstract
Purpose
Previous classifications of tibial malformations are no longer sufficient and practical for clinics and treatment. They are not precisely defined, include incorrect pathological–anatomical definitions, are related to X-ray diagnosis only, miss complete formal types of malformation, or describe too complex concepts not useful for clinical applications (Jones et al., J Bone Joint Surg B 60:31–39, 1978; Kalamchi and Dawe, J Bone Joint Surg B 67:581–584, 1985; Henkel et al., Arch Orthop Trauma Surg 93:1–19, 1978). More precise preoperative diagnosis, including by sonography and MRI and experienced intraoperative analysis of anatomical structures ensure exact description of the pathological–anatomical situation which can be used because of new potential in therapy. Until now, no score was available for detection of additional limb malformations and, therefore, clinical and scientific comparison of the different tibial reduction deficiencies, especially in respect to the success of therapy, was not sufficiently realisable. A new classification and score is presented reflecting the improved therapy currently available.
Methods
In this classification and score the main pathological findings of the complete leg are included (coxa–femur–patella–tibia–fibula–pes), with specific importance of the tibia. Tibial malformations are divided into seven main groups and five of them into two subgroups. The cartilaginous anlage of the tibia which has not yet received much attention in the literature plays an important role in this classification. Only seven main types of tibial defect have to be recognized and, if necessary, additional defects of the whole leg, including the function of the affected parts, can be summarized in a-five-class-system.
Results
With this classification and this score system which was evaluated on 95 affected limbs, with a sex ratio of 51%:49% (male:female), right:left affection, and unilateral:bilateral affection also, we found the sequence of the distribution of types as follows: 61% of cases with type-VII, 15% with type-III, 6% with type-I, 6% with type-V, 5% with type-II, 3% with type-IV, and 3% with type-VI. In comparison with the Jones et al. (J Bone Joint Surg B 60:31–39, 1978), Kalamchi and Dawe (J Bone Joint Surg B 67:581–584, 1985) and Henkel et al. (Arch Orthop Trauma Surg 93:1–19, 1978) classifications the tibial defects in the presented classification are detected more precisely, the pathological anatomical terms are correctly used, the whole leg and all main functions are included and, thus, reference to therapeutical possibilities is given.
Conclusions
The new classification and the score system allow simple, therapeutically relevant, and comprehensive classification and, additionally, scientific comparison of the different pattern of defects described by diverse authors. For daily clinical use the tibial classification only is preferred.
Introduction
The first correct description of so-called tibial hemimelia was given by Billroth [1] according to Dankmeijer [2]. The longitudinal tibial reduction defect is a very rare disease with an incidence of 1 in 1,000,000 live births [3, 4]. The major classifications of the literature are antiquated and based only on X-ray findings. Furthermore, they are not exactly defined, include incorrect pathological–anatomical definitions, include incomplete formal types of malformation [5, 6], or describe concepts—without functional data—which are too complex and, thus, not useful for clinical application [7]. None of these classifications reflects the importance of the cartilaginous anlage. Therefore, they are not useful therapeutically. A more precise preoperative diagnosis, including sonography and MRI, and experienced intraoperative analysis of anatomical structures ensure exact analysis of the pathological–anatomical situation, which can be used because of new potential in therapy [8, 9]. The previous classifications of tibial malformations are no longer useful for present-day requirements. A new classification for tibial malformations with therapeutic relevance is presented. It reflects the severity of pathological–anatomical conditions and, especially, the important role of the cartilaginous anlage (Fig. 1). For adequate therapy precise classification is required. For comparison of the results in different therapeutic procedures a score is needed to detect additional malformations on the affected limb according to joints, femur, foot, and muscle function. For this purpose a new score is presented in detail.
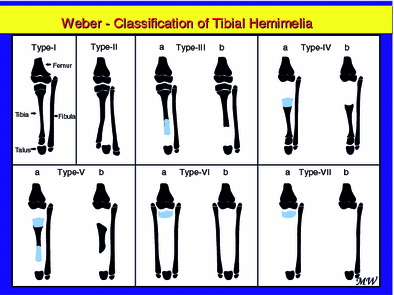
Classification of tibial reduction defects in seven types and five subgroups (a = with cartilaginous anlage, b = without cartilaginous anlage) according to the severity of the malformation. Black = bone, blue = cartilage. The figure represents a higher maturation level of the lower leg instead of the situation immediately after birth because of the possibility of giving more detailed illustrations. Type-I = hypoplasia, type-II = diastasis, type-III = distal aplasia, type-IV = proximal aplasia, type-V = bifocal aplasia, type-VI = agenesia with double fibula, type-VII = agenesia with a single fibula
Patients and methods
A total of 63 patients with 95 affected limbs were analysed retrospectively in respect of the presented classification and score, with regard to their statistical data.
In this new classification and score the main anatomical findings of the complete leg are included (coxa–femur–patella–tibia–fibula–pes) obviously with specific importance of the tibia. The tibial malformations are divided into seven main groups and five of them into two subgroups. The cartilaginous anlage is marked in the subgroups with a, when present, and with b, when absent (Table 1, Fig. 1). The pathological–anatomical terms are used with regard to their original definitions. As these terms do not differentiate between cartilaginous and osseous anlagen a correlation with one or both must be made. For easy use all the following definitions are related to the osseous anlage. Thus, hypoplasia is defined as complete but underdeveloped osseous part of the skeleton. Aplasia is defined as partial loss of an osseous part of the skeleton (e.g. proximally or distally). A cartilaginous anlage can be present or absent in the proximal or distal location. In contrast, agenesia describes total lack of the tibial bone. A cartilaginous anlage can be present and is normally located proximally and is small in size.
Classification and score system for the tibial reduction defect of the leg
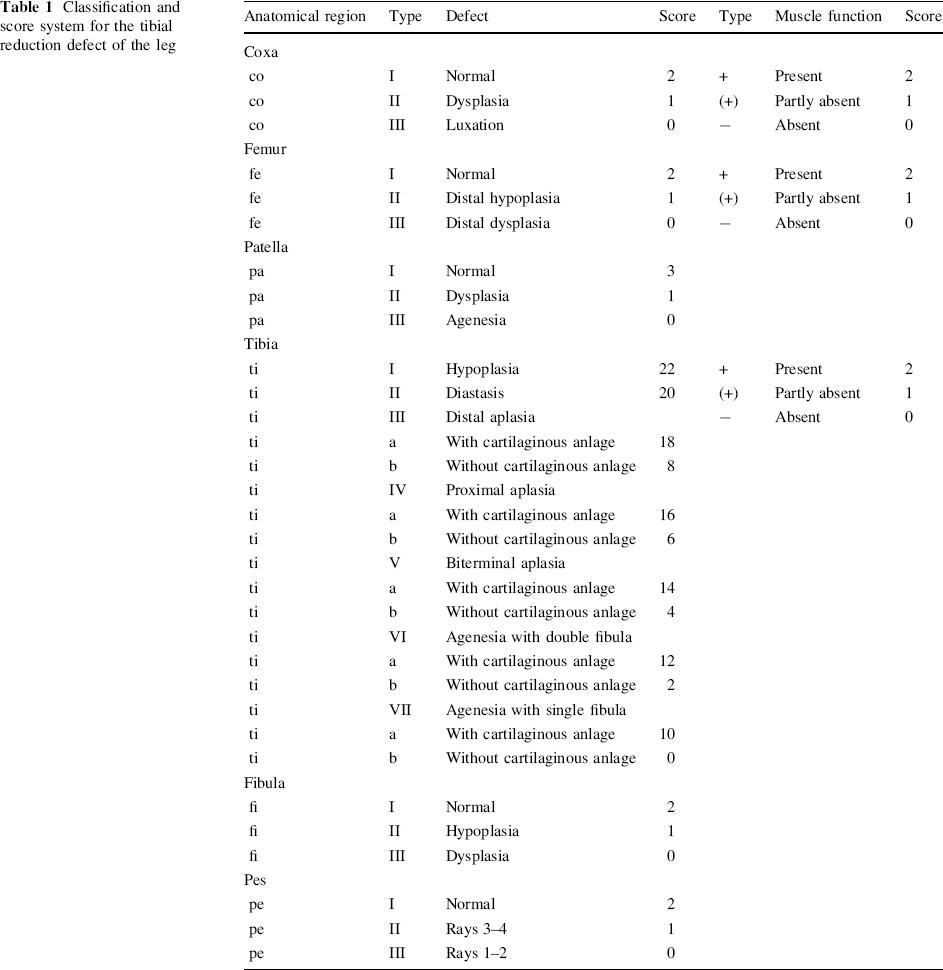
The definitions of the new score are:
For hip, femur, patella, fibula, foot, and muscle function three types of each are defined in relation to the extent of their defects. According to the importance of the patella for constructive operations the maximum score is three points (Fig. 4). For hip, femur, fibula, and muscle function two points are intended. The importance of the cartilaginous anlage, especially for constructive operations, finds its expression in a ten-point higher rate between a and b of the same type and eight point higher rate between annexed different tibial types with a cartilaginous anlage (e.g. type-IVa = 16) versus without anlage (e.g. type-IIIb = 8). A difference of two points distinguishes the annexed different tibial types inside the a-group or b-group (e.g. IIIb = 8; IVb = 6). The higher the number the less is the grade of impairment. The minimum is 0 and the maximum is 39 points. To characterize the extent of defects of the extremity, corresponding abbreviations are introduced: coxa (co); femur (fe); patella (pa); tibia (ti); fibula (fi); pes (pe). The three types of muscle function are described as +; (+) and −. The abbreviations are related to the corresponding anatomical region. Certainly, the complete status of muscle function cannot be integrated in a practicable score system. The lack of quadriceps muscle function is defined as (+) and related to the femur. The muscle function (+, (+), −) which is responsible for the movement of the hip joint is ascribed to the coxa, that which moves the knee joint is connected to the femur and that which moves the foot is connected to the tibia (Figs. 2–4).
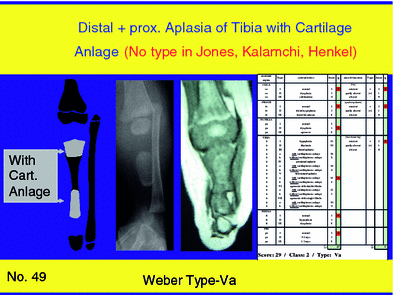
Case 49. Schematic drawing, X-ray, MRI, and score of Weber type-Va tibial hemimelia. No classification is available in the Jones, Henkel, and Kalamchi and Dawe systems
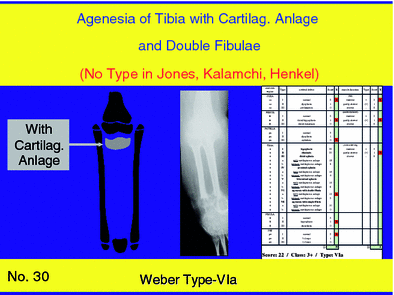
Case 30. Schematic drawing, X-ray, MRI, and score of Weber type-VIa tibial hemimelia. No classification is available in the Jones, Henkel, and Kalamchi and Dawe systems
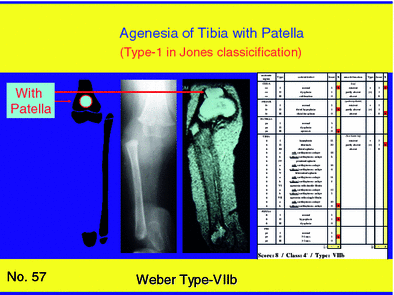
Case 57. Schematic drawing, X-ray, MRI, and score of Weber type-VIIb tibial hemimelia. MRI ap view with flexed knee shows the patella in coronal view
Example 1 Distal diastasis of the tibia with four-ray foot and normal hip joint, normal femur, normal patella, normal fibula, and normal muscle function is abbreviated coI+/feI+/paI/tiII+/fiII/peII with a score of 37 points (2 + 2/2 + 2/3/20 + 2/2/2).
Example 2 Tibial agenesia without cartilaginous anlage, reduced muscle function, and singular hypoplastic fibula, normal hip, missing function of the quadriceps muscle, femoral hypoplasia, agenesia of patella, and three-ray foot is abbreviated coI+/feII−/paIII/tiVIIb(+)/fiII/peII with a score of eight points (2 + 2/1 + 0/0/0 + 1/1/1).
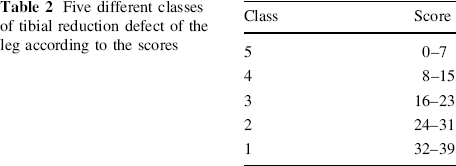
According to the score system five classes of defect are defined (Table 2): Example 1 can thus be referred to as tibial defect type II/class1 and Example 2 as tibial defect type VIIB/class 4−. According to the class, a tendency to the next lower class is described (−) and a tendency to the next higher class is described (+).
Five different classes of tibial reduction defect of the leg according to the scores
Results
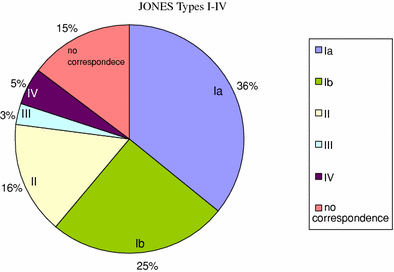
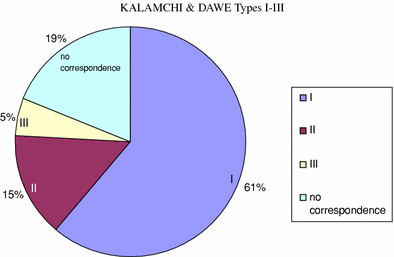
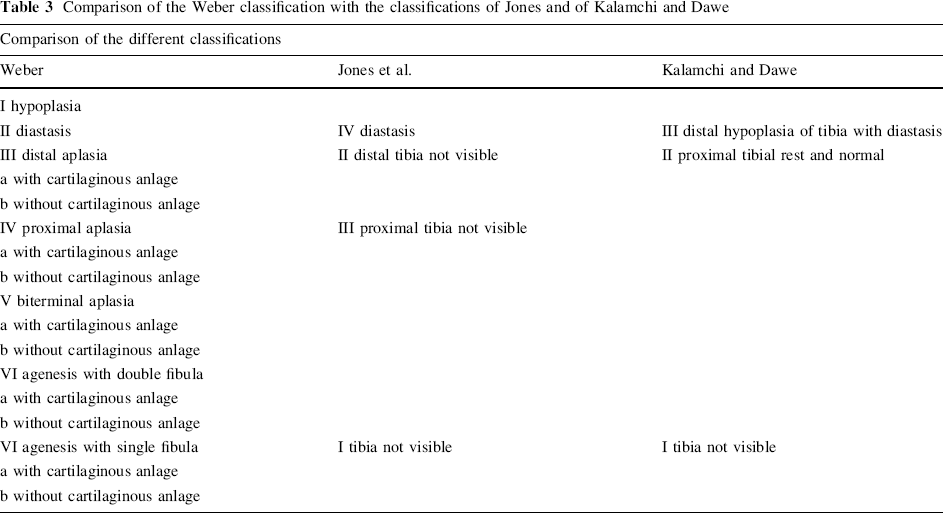
Our sample shows a sex ratio of 51%:49% (male:female), right:left affection, and unilateral:bilateral affection also. According to the Weber-classification the sequence of the distribution of types is as follows: 62% of cases with type-VII, 15% with type-III, 6% with type-I, 6% with type-V, 5% with type-II, 3% with type-IV, and 3% with type-VI (Diagram 1). According to the Jones classification our sample comprises: in 36% of cases type-Ia, in 25% type-Ib, in 16% type-II, in 5% type-IV, in 3% type-III, and in 15% no correspondence to our cases (Diagram 2). In the Kalamchi and Dawe classification our patients display: in 61% type-I, in 15% type-II, in 5% type-III and in 19% no correspondence to our cases (Diagram 3). Direct comparison of the Weber classification with the Jones classification shows that hypoplasia, biterminal aplasia (Fig. 2), and agenesia with double fibula (Fig. 3) are not included in the Jones classification. Furthermore, the Kalamchi and Dawe classification does not include hypoplasia, proximal aplasia, biterminal aplasia (Fig. 2), and agenesia with double fibula (Fig. 3), in contrast with the Weber classification (Table 3, Fig. 1). It is important to note that all three old classifications do not take into account the cartilaginous anlage.
Distribution of the different types of tibial hemimelia in our sample, in the Weber classification Distribution of the different types of tibial hemimelia in our sample, according to the Jones classification Distribution of the different types of tibial hemimelia in our sample, according to the Kalamchi and Dawe classification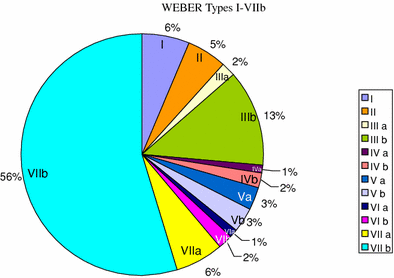
Comparison of the Weber classification with the classifications of Jones and of Kalamchi and Dawe
Discussion
The decision to define the bone of the tibia as fundamental to the classification is based on the following reasoning:
the bone can be detected by simple X-rays; in the past MRI or ultrasonography were not available; and categorisation of the main types of tibial reduction deficiency is realisable, even if the cartilage anlage cannot be diagnosed for some reason.
If a definition is based on the complete anatomic structure (bony and cartilaginous anlage), aplasias with, e.g., a cartilaginous anlage must be defined theoretically as distally or proximally accentuated hypoplasias with missing osseous maturation. However, those cartilaginous anlagen are frequently not completely matured. Thus, more descriptions are necessary to improve the fine structure of the classification. The use of the bony anlage as guidance for the classification facilitates this process.
Detection of a cartilaginous anlage (by ultrasonography, MRI, intraoperative view) which until now has been paid no attention in the literature is of considerable clinical significance (Fig. 2). If the cartilaginous anlage comes in contact with the corresponding joint it matures completely to an osseous structure, including growth plates, because of the processes of callus distraction, weight loading, and functional loading. Thus, the cartilaginous anlage plays a key role in this new classification. The terms partial or complete aplasia, frequently found in the literature, are confusing descriptions because aplasia is, by definition, a partial defect of a skeletal bone without restriction of any kind [5, 6]. The correct definition of agenesia is the complete absence of a skeleton bone. Normally, the cartilaginous anlage of an osseous tibial agenesia is proximally located. Theoretically, distal location or complete cartilaginous anlage of the tibia could be possible. However, I am not aware of such a case either in my own patients or in the literature. For this reason, a subclassification does not seem reasonable at the moment. Thus, an additional description with proximal, distal location, bifocal location, or complete cartilaginous anlage seems sufficient in this context.
Certainly, the classification of Henkel et al. [7] reflects the variety of possible tibial reduction defects, however, it misrepresents a classification as it is only a formula usable for description of the countless defects of this disease. Their detailed description is not useful clinically because a reduction to the main pattern of malformations is not given. However, it is a requirement for therapy to differentiate important facts from those of no importance. On the one hand, a classification appropriate for clinical use should focus on the main different types leading to diverse therapeutic procedures. On the other hand, it is not reasonable to renounce malformation types of important therapeutic relevance only to receive a simple classification. The more details characterizing a classification, the more inapplicable is their clinical practicability. The more a classification reduces the details the more is the risk that important malformations are disregarded. The classifications of Jones et al. [5] and Kalamchi and Dawe [6] applied to our sample showed that in 15 and 19% of the cases, respectively, the affected legs would not be categorized. It is important to note that this lack includes important types for which therapy is successful. Thus, a classification should be as detailed as necessary and as reduced as possible.
My classification designed for the therapist fulfils this requirement clearly. The severity of the disease intensifies with the number of malformation types. The absence of the cartilaginous anlage increases the difficulty of the operative procedure, and finds its expression in the score with a difference of ten points within a type, whereas the difference of adjoining types amounts only to two points (Table 1). The seven different types are clearly distinguished therapeutically. Depending on the presence or the lack of the cartilaginous anlage twelve different operative procedures are necessary to include a specific malformation. For this reason, rare types (1% type-IVa and 1% type-VIa) in our sample are respected in the classification. It should be pointed out that in comparison with the other types these infrequent types require different characteristic operative procedures because of their specific impairment [8, 9].
The character of other affected structures of the complete leg is of tremendous significance in respect of the treatment of tibial reduction deficiency. This means that, e.g., damage to the hip, a missing function of the quadriceps, or a lack of the patella is of importance for a successful operation with consequent improvement of function. Thus, the system of the score includes the complete extremity to define the extent of the malformation in combination with the classification of the tibial reduction deficiency. This is reflected in the new score which allows, for the first time, a comparison of different forms of treatment and a definition of basic principles of treatment in relation to the extent of the malformation (Tables 1, 2). Both the classification and the score system are based on the main pathological alterations for practical use and are designed for surgeons.
Only seven main types of tibia defect have to be recognized and, if necessary, other defects of the whole leg can be summarized in the five-class-system (Table 2). With this classification and score system the tibial defects are detected more precisely, the pathological anatomical terms are used correctly, the whole leg and its function are included, scientific comparison of the treatment outcome of different types and results from different authors is possible and, consequently, a recommendation for therapeutic possibilities is given.