
Abstract
Abstract
Purpose
Modern principles for treatment of patients with myelomeningocele include early closure of the neural tube defect, neurosurgical treatment of hydrocephalus and treatment aimed at minimizing contractures and joint dislocations. The aim is to achieve a better survival rate and a better quality of life (QOL). Better ambulatory function is thought to improve the management of activities of daily living. This study focused on evaluating which factors might affect ambulation, function and health-related QOL in children with myelomeningocele.
Methods
Thirty-eight patients with neurological deficit from myelomeningocele were examined in an unbiased follow-up. This included a physical examination using validated methods for ambulatory function and neuromuscular status, chart reviews and evaluation of radiographs in terms of hip dislocation and spine deformity. The Pediatric Evaluation of Disability Inventory (PEDI) was used to measure mobility, self-care and social function, and the Child Health Questionnaire (CHQ-PF50) was used to measure QOL.
Results
Muscle function class, quadriceps strength, spasticity in hip and/or knee joint muscles and hip flexion contracture as well as the ambulatory level all affected functional mobility as well as self-care/PEDI. Patients with hip dislocation, spinal deformity or those who were mentally retarded also had significantly worse functional mobility. Besides being affected by the severity of the neurological lesion, self-care/PEDI was significantly impaired by hip flexion contracture and absence of functional ambulation. General health-related QOL was significantly lower in this patient group than for US norms. Nonambulatory and mentally retarded patients had a significantly lower physical function of their QOL (CHQ).
Conclusions
The severity of the disease, i.e. reduced muscle strength and occurrence of spasticity around hip/knee, affected ambulation, functional mobility and self-care. Acquired deformities (hip dislocation and spine deformity) affected functional ambulation only. Patients with reduced functional mobility and self-care experienced lower physical QOL. Children with myelomeningocele had significantly reduced QOL compared to healthy individuals.
Introduction
With modern principles for treatment of patients with myelomeningocele; i.e. early closure of the neural tube defect and neurosurgical treatment of hydrocephalus, which have been used since the beginning of the 1970s, the early mortality rate has dropped. Also, morbidity due to kidney disease has been substantially reduced with the introduction of clean intermittent catheterization for management of neurogenic bladder. Individuals with myelomeningocele should now be expected to survive into adulthood. The emphasis of medical care is shifting to enhancing quality of life (QOL) and promoting independence [1].
The ability of an individual to care for oneself is highly dependent on the functional mobility of that individual. Achieving independent ambulation has traditionally been the goal of orthopaedic treatment and is the aspect of mobility that receives the most attention. It is assumed that maximizing ambulatory function will promote future independent living and higher QOL; however, the relationship of ambulation to other functional skills and QOL has not been fully explored.
The purpose of this study was to investigate which factors might negatively influence ambulatory function and explore the connection between ambulation, function and health-related QOL. Increased knowledge might help to predict future ambulation, thereby improving treatment planning. It might also answer the question of whether better ambulatory function renders a better QOL in children with myelomeningocele.
Materials and methods
Patients
Patients were recruited from two centres with well-established treatment for children with myelomeningocele: the Walter Reed Army Medical Center, Washington DC, and the Kennedy Krieger Institute, Baltimore, MD, USA. All patients fulfilled the inclusion criteria: (1) there was a myelomeningocele that had been surgically treated in the neonatal period; (2) there was the presence of some motor deficit regardless of level of spina bifida; (3) age was between 3 and 16 years at the time of inclusion in the study; (4) treatment occurred at one of the two centres at the time of the study; (5) acceptance and ability to participate in the study. Eleven children at the Walter Reed Army Medical Center and 27 patients at Kennedy Krieger Institute completed the study, so the total number of patients included was 38.
Physical examination
Two physiotherapists who had not taken part in the treatment of the patients, either one of the authors (Å.B) or a physiotherapist especially trained by her for this study, performed the physical examinations. All methods used for physical examination, Table 1, have been validated, shown to be reliable and previously used in published studies.
Definitions and descriptions of used gradings of muscle function classes, functional ambulation, PEDI and CHQ-PF50
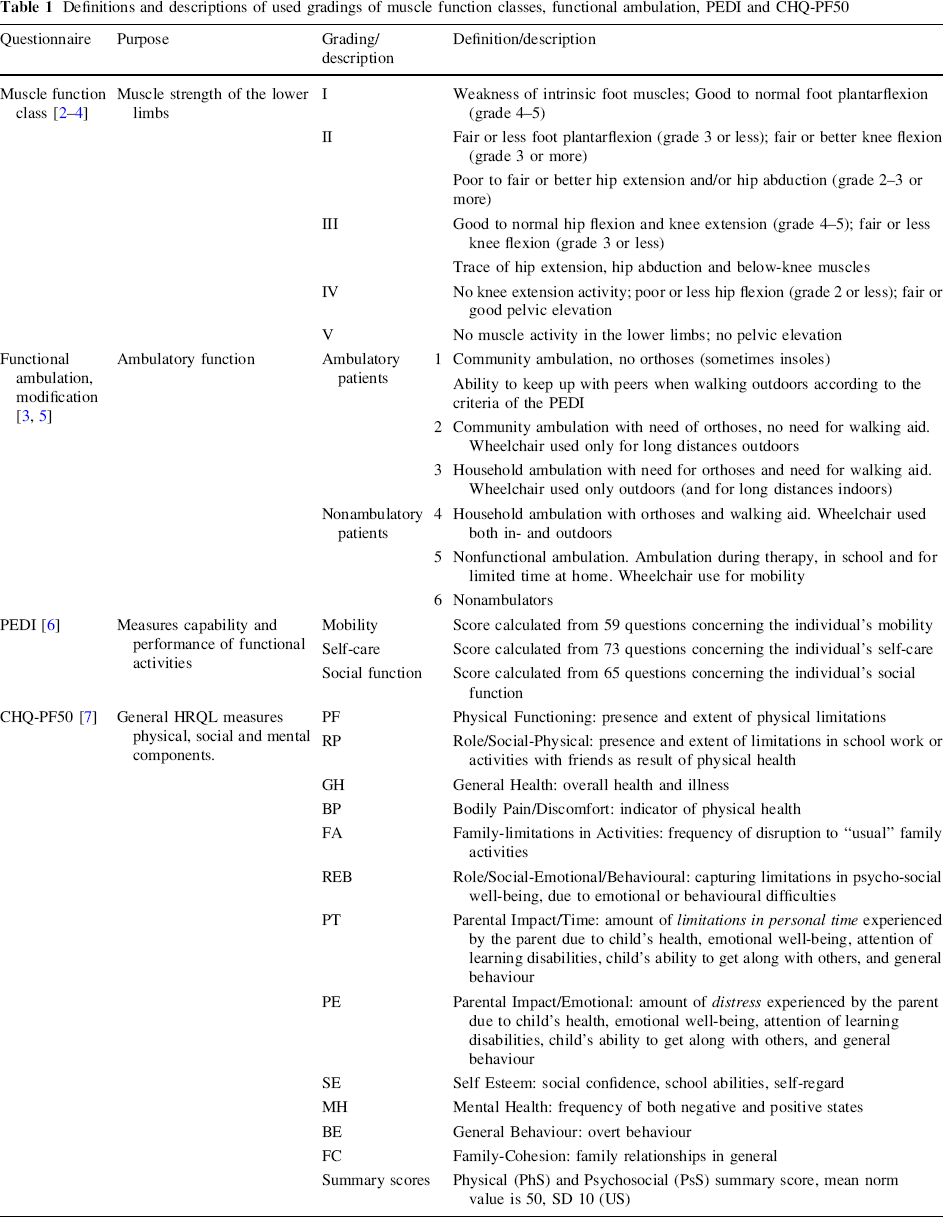
The children were divided into five classes of muscle function according to their lower limb muscle strength [2, 3]. The development of muscle function classes was based on a comparison of six different classification systems with the aim to facilitate comparison of treatment results with special consideration of ambulation [4]. This classification was found to be reliable and work well both for clinical judgments and for outcome documentation in the Swedish studies of these authors.
Presence of spasticity in the lower limb muscles was documented. Spasticity was considered present if the patient showed one or more of the following signs: static abnormal posturing with increased muscle tension despite full passive motion of a joint, velocity-dependent catch response, resistance throughout passive range of motion or clonus. For the purpose of statistical analyses, patients were grouped into two groups; no spasticity of lower limbs or around ankle joint, or occurrence of spasticity around the knee and/or hip joints.
The range of motion of the lower limb joints was assessed according to the recommendations of the American Academy of Orthopaedic Surgeons [8]. Joint contractures of the lower limb were defined for the ankle if ≥15 degrees of fixed equinus foot, for knee if ≥20 degrees of extension contracture or for hip if ≥20 degrees of extension contracture were observed. Hip flexion contracture was measured using Thomas’ test [9]. All contractures were measured in the supine position.
The ambulatory function was assessed using the criteria of Hoffer et al. [5], with some modifications [3]. For the purpose of statistical analyses, patients were grouped together as either “ambulatory”, i.e. ambulating but using wheelchair only for long distances outdoors (Grade 1–3) or “nonambulatory”, i.e. using wheelchair both in- and outdoors (Grade 4–6).
Key functional capabilities and performance were measured by the Pediatric Evaluation of Disability Inventory (PEDI, Table 1) [6]. In a parent-report questionnaire, administered in an interview session, the parents were asked questions that reflect the three content domains: self-care (73 questions), mobility (59 questions) and social function (65 questions). All children had scaled scores that provide an estimate of the level of capability regardless of age and can be used for the evaluation of children over the age of 7.6 years if their functional abilities fall below those expected of 7.5-year-old children with no disabilities. The scaled scores range from 0 to 100, where 100 reflects the best function. The PEDI can be used for the comparison of children of all age groups; however, no norm scales exist for children above the age of 7.5 years. The questionnaire has previously been used in populations with myelomeningocele.
Review of charts and radiographs
Chart reviews for all examined patients were performed to collect information on previous medical and surgical treatments as well as complication(s) of the disease and other concomitant diseases.
Radiographs of the hips and spine were located, and if older than one year a new examination was undertaken. The prevalence of hip dislocation was noted. Four patients did not have new radiography performed; however, a judgment of the occurrence of hip dislocation was possible through clinical evaluation in combination with older radiographs.
For the spine, the existence of scoliosis or kyphosis, including Cobb angle [10] and apex of the curve, was noted. Radiographs of the spine older than one year were used in five patients, who did not show any clinical signs of scoliosis at physical examination.
Questionnaires
Parents underwent a nurse interview session. Information on mental retardation was collected from the Individual Education Program (IEP) of the specific patient. The IEP is a written document that is developed for each public school child who is eligible for special education and is a mandated requirement of the “Individuals with Disabilities Education Act” of the United States.
A validated questionnaire on general health-related QOL, the Child Health Questionnaire-50 Parent Form (CHQ-PF50) [7], was answered by the parent (Table 1). It measures the physical, social and mental components of health-related QOL. The questionnaire has 12 subscales and each is scored from 0 to 100, where 100 reflects the best function. It also offers an opportunity to calculate physical and psychosocial summary scores (PhS and PsS respectively), each with a mean norm value of 50. The CHQ has been validated in many countries and used for a variety of different diseases, including myelomeningocele [11]. The national norms for a population sample of US children have been used for comparison with the results from our study group.
Ethics
The Institutional Review Boards at the Johns Hopkins Hospital, Baltimore, MD and the Walter Reed Army Medical Center, Washington, DC, United States, approved the study.
Statistical methods
Distributions of variables are given as means, standard deviations (SD) and ranges.
When comparing two groups, Fisher's exact test for dichotomous variables, chi-square test for nonordered categorical variables and Mantel–Haenszel chi-square test for ordered categorical variables were used. Mann–Whitney's U-test was used for continuous variables.
The Student's t-test was used for comparison with the US norm values.
The Spearman rank correlation coefficient (r s) was used for correlation analyses.
All tests were two-tailed and conducted at the 5% significance level.
Results
Age distribution, gender, racial origin and neurological findings of the patients are found in Table 2. Thirty-five (92%) patients had a shunt, of which 69% had been revised twice or more. Nine patients had mild or moderate mental retardation (none had severe or profound mental retardation).
Age, gender, racial origin and neurological findings in 38 patients with myelomeningocele [Mean (SD)/Median (Min−Max) orn(%)]
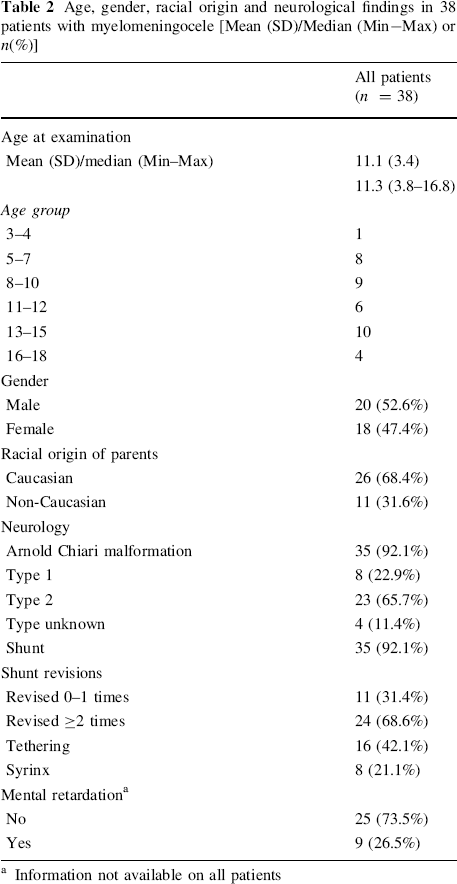
Information not available on all patients
Neuromuscular status and orthopaedic manifestations
Information on the musculoskeletal status of the patients is shown in Table 3, divided up by functional ambulation. Nineteen children were ambulatory and nineteen non-ambulatory.
Characteristics of 38 patients with myelomeningocele divided up by ambulatory function [n(%)]
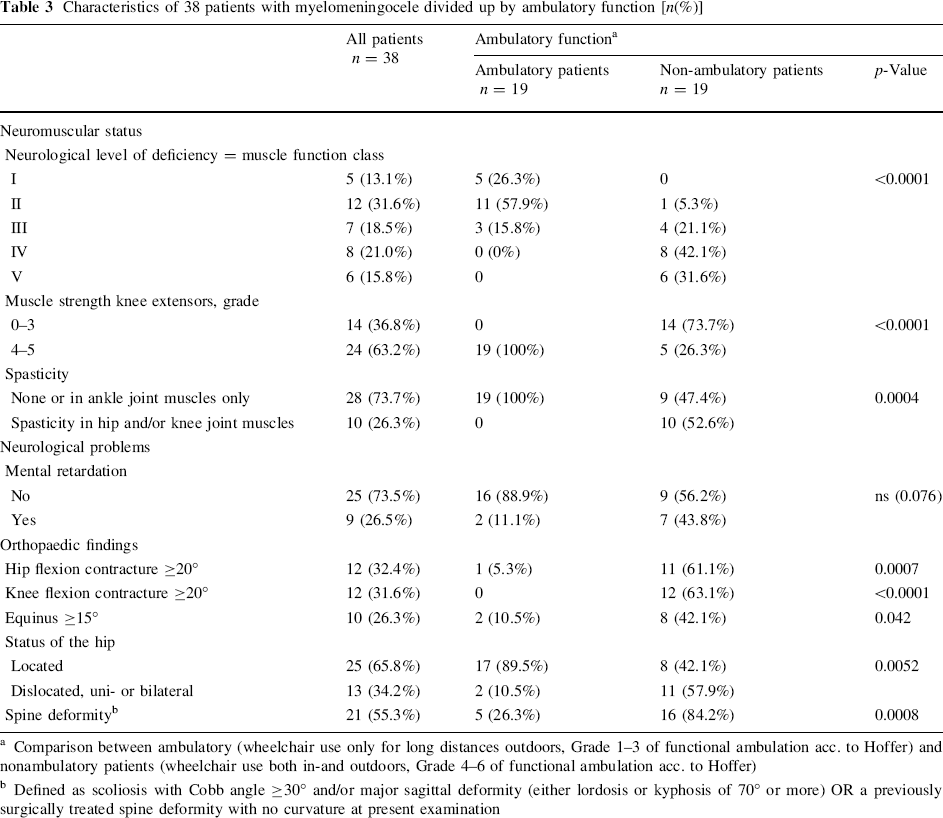
Comparison between ambulatory (wheelchair use only for long distances outdoors, Grade 1–3 of functional ambulation acc. to Hoffer) and nonambulatory patients (wheelchair use both in-and outdoors, Grade 4–6 of functional ambulation acc. to Hoffer)
Defined as scoliosis with Cobb angle ≥30° and/or major sagittal deformity (either lordosis or kyphosis of 70° or more) OR a previously surgically treated spine deformity with no curvature at present examination
The only child in age group 3–4 years was ambulatory (Grade 2 acc. to Hoffer). Among the eight children aged between five and eight years at examination, six were ambulatory and two were nonambulatory. One of these two nonambulatory children was 5.4 years at examination, had muscle function class III, hip contractures of more then 20°, bilateral hip dislocations and a scoliotic curve of 35°. The other nonambulatory child, 7.6 years of age, had muscle function class V, spasticity around hip and knee joints with hip and knee contractures of more then 20° as well as equinus, unilateral hip dislocation and a kyphoscoliotic spinal curvature (95° thoracic kyphosis and 26° scoliosis).
Patients with weak quadriceps muscles (strength of 1–3), less lower limb muscle strength or spasticity around the hip and/or knee joints were significantly more often nonambulators. All ambulatory patients had quadriceps muscle strength of 4–5.
Eleven percent of ambulatory patients were mentally retarded compared to 44% of nonambulators, ns (p = 0.076). Occurrence of shunt, shunt revisions twice or more, tethering or syrinx was not more frequently seen among the nonambulators.
Patients with hip or knee flexion contracture of 20° or more or equinus of at least 15°, approximately one-third of the patients, were significantly more often nonambulators. Thirteen patients (34%) had uni- or bilateral hip dislocations. 17/19 (89%) of the ambulatory patients had located hips, while 11/13 (84%) patients with hip dislocation(s) were nonambulatory, p = 0.0052.
Nine patients had a scoliotic spine with a curvature of at least 30° (Cobb) at the present examination, and another two patients were previously surgically treated for a scoliotic deformity, and now had a straight spine. Twelve patients had a major sagittal deformity (either lordosis or kyphosis of 70° or more), of which two also had a scoliotic deformity. Out of the total 21 patients with spine deformity, only five patients, all with muscle function class I–III and without spasticity or joint contracture, were ambulators. Out of the 16 nonambulators with spinal deformity, four patients had muscle function class I–III and 12 had class IV–V, but all 16 had either spasticity around hip/knee, joint contractures or hip dislocation.
PEDI/functional skills
Table 4 depicts functional skills as measured by PEDI. All three domains; mobility, self-care and social ability were tested against factors found to affect the ability to ambulate (Table 3). Testing was also performed for ambulatory versus nonambulatory patients and for normally intelligent versus mentally retarded children.
PEDI/functional skill domains in 38 patients with myelomeningocele, divided up according to subgroups of clinical status [Mean (SD)/(Min–Max)]
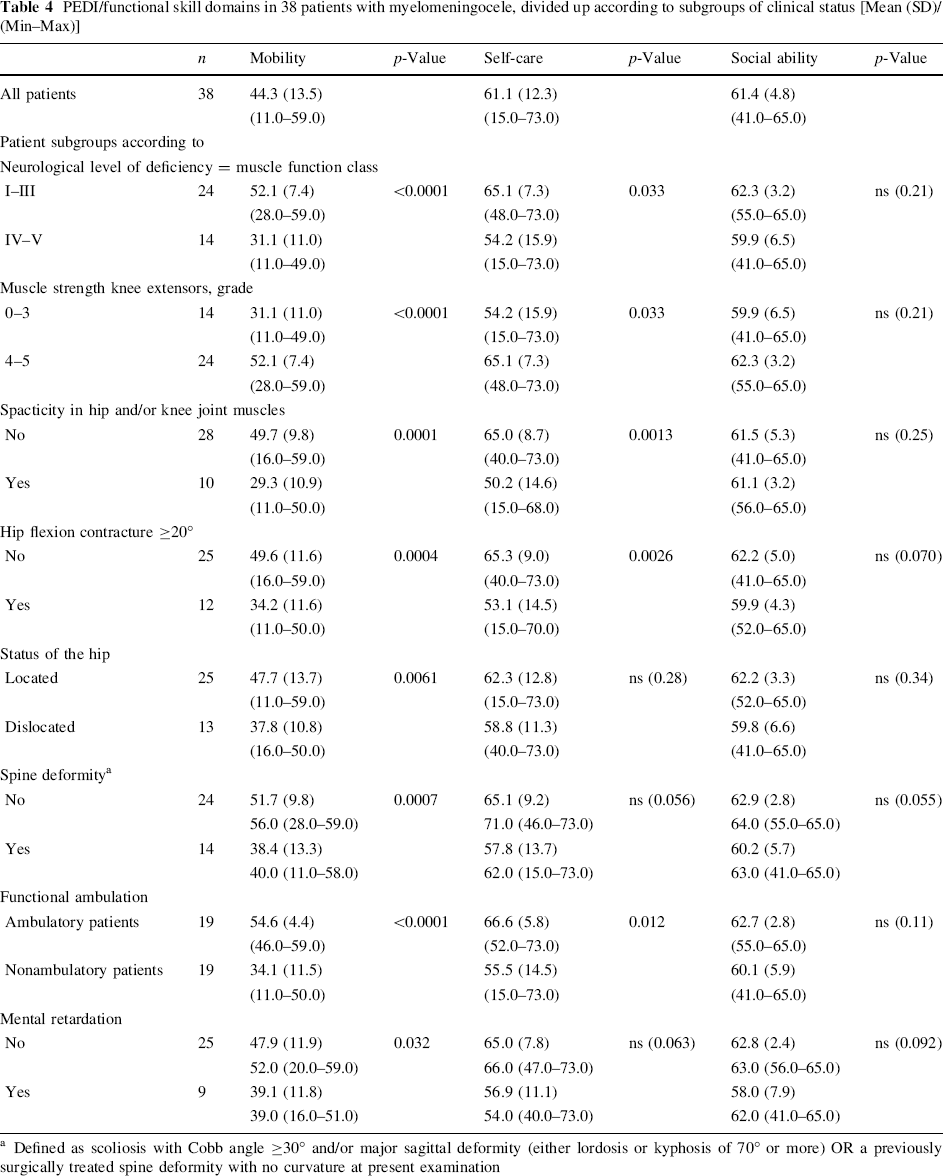
Defined as scoliosis with Cobb angle ≥30° and/or major sagittal deformity (either lordosis or kyphosis of 70° or more) OR a previously surgically treated spine deformity with no curvature at present examination
Functional mobility and functional self-care both were significantly better in patients with better lower limb muscle strength, quadriceps muscle strength of grade 4–5, no spasticity around the hip or knee joint, less than 20° hip flexion contracture or in ambulatory patients.
Function due to mobility also was significantly deteriorated by occurrence of hip dislocation, spine deformity and by being mentally retarded. None of the factors studied affected the social ability domain significantly.
Quality of life
Quality of life as measured with the CHQ was significantly reduced in children with myelomeningocele as compared to the US normative sample in all subscales but self esteem (SE), general behaviour (BE) and family cohesion (FC), Fig. 1. The summary scores were also significantly lower than the US norms, 31.5 vs. 53.0 (p < 0.0001) for the physical component summary score (PhS) and 47.9 vs. 51.2 (p = 0.036) for the psychosocial component summary score (PsS), Fig. 2.
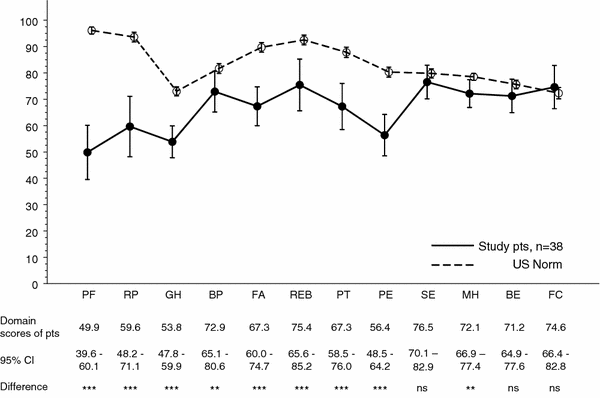
CHQ-PF50: results for subscales for patients with myelomeningocele versus national US norms. Mean with 95% CI. QOL as measured with the CHQ was significantly reduced in children with myelomeningocele as compared to the US normative sample in all subscales but self esteem (SE), general behaviour (BE) and family cohesion (FC). Subscales of CHQ: PF = Physical Functioning; RP = Role/Social-Physical; GH = General Health; BP = Bodily Pain; FA = Familiy-Activities; REB = Role/Social-Emotional/Behavioural; PT = Parental Impact-Time; PE = Parental Impact-Emotional; SE = Self Esteem; MH = Mental Health; BE = General Behavior; FC = Family-Cohesion
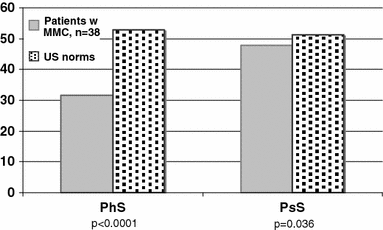
CHQ-PF50: summary scores for patients with myelomeningocele vs. national US norms. Both physical and psychosocial summary scores were significantly lower among patients with myelomeningocele than US norms. PhS = physical summary score, PsS = psychosocial summary score
Comparisons of QOL for subgroups of the study population in terms of ambulatory function or mental retardation are presented in Fig. 3. Physical functioning was significantly affected by ambulatory function (PF for ambulatory patients 59.1 vs. 40.6 for nonambulators, p = 0.020) as well as by mental retardation (PF for normally intelligent children 58.7 vs. 27.8 for mentally retarded children, p = 0.010).
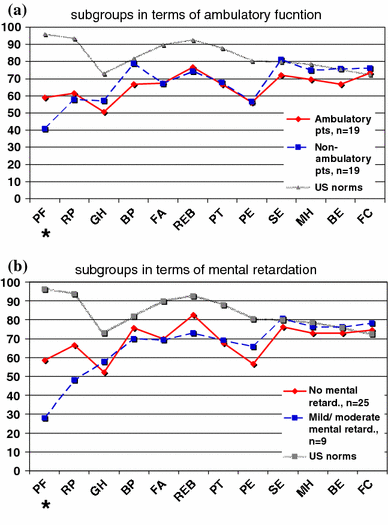
CHQ-PF50: Comparisons of QOL for subgroups of the study population. Subscales of CHQ: PF = Physical Functioning; RP = Role/Social-Physical; GH = General Health; BP = Bodily Pain; FA = Familiy-Activities; REB = Role/Social-Emotional/Behavioural; PT = Parental Impact-Time; PE = Parental Impact-Emotional; SE = Self Esteem; MH = Mental Health; BE = General Behaviour; FC = Family-Cohesion.
Correlations were found between the physical performance (PF) of the QOL and all three domains of PEDI, self-care (r = 0.51, p = 0.0012), mobility (r = 0.60, p < 0.0001) and social ability (r = 0.32, p = 0.049). These results were also reflected in the physical summary score (PhS score), which was correlated with self-care (r = 0.34, p = 0.035) and mobility (r = 0.38, p = 0.020).
Discussion
A considerable number of orthopaedic procedures as well as physiotherapeutic efforts and orthotic device production are performed with the aim to keep the lower extremities straight and hip joints located. Whether these efforts really have a positive impact from the patient's perspective and whether a higher level of ambulation really is correlated to a better QOL provide the focus for this paper. We also wanted to delineate between internal or external factors that might affect the ability of growing individuals with myelomeningocele to have independent mobility.
It might be questionable as to whether the younger children in the study had acquired their final ambulatory function. In the eight children less than eight years of age, six were already ambulators. The other two (nonambulatory) children had low muscle strength in combination with contractures and deformities to an extent that will make future ambulation doubtful. Therefore, we considered the grading of the ambulatory function reliable enough for analysis.
The neurological lesion itself did affect whether the patient was an ambulator or not. Patients with stronger lower limb muscles were significantly more often ambulating and all ambulatory patients had quadriceps muscle strengths of 4–5. The role of the knee extensor muscle strength in ambulation was in accordance with earlier studies by McDonald et al. [12], Mazur and Menelaus [13] and Huff and Ramsey [14], who all highlighted the importance of a quadriceps muscle strength grade of 4–5 for walking with ankle-foot orthoses.
Existence of spasticity around the hip and knee joints as well as spine deformity were deleterious for ambulation. The spasticity itself might also be a contributing factor to contractures of hips and knees, which were strongly associated with the loss of walking ability. These findings are in accordance with earlier publications [3, 5, 15–18]. Patients with hip dislocation were also significantly more often nonambulators than those with contained hips.
Even though only two out of nine (22%) mentally retarded patients were ambulators compared to 16 out of 25 (89%) normally intelligent children, this difference did not reach statistical difference. This might be due to the small number of patients in the study. However, in the measurements on physical function, patients with mental retardation showed significantly worse results both in terms of functional mobility domain/PEDI and physical function (PF) of the CHQ.
Functional mobility as well as self-care was significantly affected by the severity of the neurological symptoms; muscle function class, quadriceps strength and spasticity in hip and/or knee joint muscles. Furthermore, functional mobility was also significantly affected by secondary orthopaedic deformities/conditions. This discloses possible relationships between secondary orthopaedic deformities and mobility, which need further studies to verification. Larger patient groups with less heterogeneity in terms of age, physical function, neurological lesion and associated orthopaedic deformities as well as regression analysis will be needed to obtain scientific proof; these prerequisites could not be obtained for this study group.
Correlations between PEDI scores and walking ability, intelligence or independence in activities of daily living agree with earlier publications [19]. However, none of these abovementioned factors affected the social ability. As one may expect, social abilities can develop despite impaired functional mobility or a reduced level of self-care.
General (health-related) QOL in this patient group was significantly lower than for the US norms. QOL in terms of PF was associated with the ambulatory function and mental retardation, i.e. ambulatory and nonretarded patients had less limitation. PF was also correlated to all three PEDI domains, namely self-care, mobility and social ability. This fact strongly shows the importance of functional abilities in achieving a better (physical) QOL. This is in line with earlier publications: Rendeli et al. [11] found that disability was inversely correlated to the physical aspect of QOL, and Schoenmakers et al. [20] found that being independent with regard to mobility was the most important determinant of health-related QOL. They also found that mental status, having no contractures in lower extremities and normal strength in knee extensors were the most important factors in mobility independence. The present findings, as well as the earlier literature [1, 20, 21], support surgical correction of musculoskeletal deformities, treatment of tethered cord syndrome, and they point out the importance of maximizing functional independence, good muscle strength and mental ability to achieve a better QOL.
The goal for treatment of children with spina bifida has always been to give these children a life that is as good as it can be. However, the means of doing this has been under debate for many years. One area of debate is that of ambulatory function and is the question of whether to prevent hip dislocation. In this study, we found that physical QOL was significantly reduced and the mental well-being reduced in terms of effect on family and parents, but not for the child itself. These negative effects on QOL can thus already be seen during childhood. Therefore, it is important to prevent deterioration and to enhance improvement in physical abilities during childhood.
If improvement is achieved, the physical abilities and thereby the physical QOL may reach a higher level until maturity, which will also decrease the risk of “negative over-spill” into mental well-being. The patient will then be given the best opportunities to handle his or her own life when entering adulthood.
Conclusion
Ambulatory ability as well as functional mobility was significantly affected by the severity of the neurological symptoms; muscle function class, quadriceps strength and spasticity in hip and/or knee joint muscles. They were also significantly affected by musculoskeletal complications such as hip flexion contracture, hip dislocation and spine deformity, all of which are consequences that orthopaedic treatment aims to reduce.
The general (health-related) QOL for children with myelomeningocele was significantly lower than for the US norms. Functional physical abilities were shown to be of importance for achieving a better QOL. Having a higher level of functional mobility, self-care and social ability improved the physical QOL.
In order to clarify the existence of relationships between secondary orthopaedic deformities and mobility, further studies are needed. Until this has been done, a judgment cannot be made as to whether preventive treatments for musculoskeletal complications affect the QOL of the patient.
Footnotes
Acknowledgments
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. Funds were received in total or partial support of the research or clinical study. The founding sources were the Swedish-American Foundation, the Swedish Orthopaedic Society, the Swedish Pediatric Orthopaedic Society, the Folke Bernadotte Foundation, the Swedish Medical Society, the Gothenburg Medical Society and the Norrbacka–Eugenia Foundation.