
Abstract
Abstract
Purpose
Although non-idiopathic clubfeet were long thought to be resistant to non-surgical treatment methods, more studies documenting results on treatment of these feet with the Ponseti method are being published. The goal of this systematic review is to summarize current evidence on treatment of non-idiopathic clubfeet using the Ponseti method.
Methods
PubMed and Limo were searched, reference lists of eligible studies were screened and studies that met the inclusion criteria were included. Data on average number of casts, Achilles tendon tenotomy (ATT), initial correction, recurrence, successful treatment at final follow-up and complications were pooled. The Methodological Index for Non-Randomized Studies was used to assess the methodological quality of the selected studies.
Results
In all, 11 studies were included, yielding a total of 374 non-idiopathic and 801 idiopathic clubfeet. Non-idiopathic clubfeet required more casts (7.2 versus 5.4) and had a higher rate of ATT (89.4% versus 75.7%). Furthermore, these feet had a higher recurrence rate (43.3% versus 11.5%) and a lower rate of successful treatment at final follow-up (69.3% versus 95.0%). Complications were found in 20.3% of the non-idiopathic cohort. When comparing results between clubfeet associated with myelomeningocele and arthrogryposis, the first group presented with a lower number of casts (5.4 versus 7.2) and a higher rate of successful treatment at final follow-up (81.8% versus 58.2%).
Conclusion
The Ponseti method is a valuable and non-invasive option in the primary treatment of non-idiopathic clubfeet in young children. Studies with longer follow-up are necessary to evaluate its long-term effect.
Level of Evidence
Level III – systematic review of Level-III studies.
This work meets the requirements of the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses).
Introduction
Non-idiopathic congenital clubfoot or talipes equinovarus is one of the most common developmental anomalies of the lower limb, with prevalence rates ranging from 1.1/1000 to 1.6/1000 livebirths.1–5 Most clubfeet occur as an isolated birth defect and are considered to be idiopathic in nature. Non-idiopathic clubfeet, however, develop secondary to an underlying condition, including neuromuscular and syndromic disorders. The most common identified aetiologies associated with non-idiopathic clubfeet are spina bifida and arthrogryposis.6,7
Historically, both non-operative methods as well as surgical procedures have been used to treat clubfoot deformity. Following evidence reporting high success rates of the Ponseti casting method and its superiority to surgical interventions, it is now the preferred treatment for the management of idiopathic clubfeet.8–13 Children with non-idiopathic clubfeet typically present with feet that are more rigid than idiopathic clubfeet and often have additional abnormalities which may complicate treatment of the clubfoot and influence the outcome. 14 Non-idiopathic clubfeet are therefore generally expected to be more resistant to non-operative management. However, several studies have recently evaluated the results of the Ponseti casting technique in infants with non-idiopathic clubfoot. The goal of this systematic review is to summarize current evidence on treatment of non-idiopathic clubfeet using the Ponseti method.
Materials and methods
The electronic databases PubMed and Limo were searched for relevant articles with the last search being performed in December 2017. One person performed the search (TDM), while two reviewers supervised the search method (AVC and SP). The keywords were ‘non-idiopathic clubfoot’, ‘non-idiopathic talipes equinovarus’, ‘syndrome-associated clubfoot’, ‘syndromic clubfoot’, ‘arthrogryposis’, ‘spina bifida’ and ‘myelomeningocele’, in various combinations. Articles were screened for the following inclusion criteria: diagnosis of non-idiopathic clubfoot, treatment with the Ponseti method, primary treatment of clubfoot or treatment of relapsed clubfoot after non-surgical treatment, with exception of Achilles tendon tenotomy (ATT) and the English language. Non-idiopathic clubfeet include all clubfeet associated with an underlying condition, regardless of the aetiology of the underlying condition. Reviews, abstract-only publications, studies using treatment methods other than the Ponseti method and studies on relapsed clubfoot after previous surgery, except for ATT, were excluded. No limitation was implemented regarding publication year. Eventually, the reference lists of the selected articles were screened to identify further relevant studies.
Additional inclusion criteria were added to minimize heterogeneity in baseline characteristics between studies. This way, the risk on introducing bias when pooling data of different articles was reduced. The additional inclusion criteria were: average age at start of treatment or at presentation six months or less, average follow-up period of at least two years and results on separate feet. Initial correction, average number of casts necessary to achieve correction, need for ATT, recurrence rate, successful treatment and complication rate were identified as study endpoints. A foot was classified as initially corrected when no deformity persists after the last Ponseti cast or ATT. Successful treatment was defined as a plantigrade and braceable painless foot at final follow-up, achieved with the Ponseti method and ATT only and without the need for extensive surgery. Recurrences that were successfully corrected using repeat casting and/or ATT only were, therefore, also classified as successfully treated. Complications were classified as mild if they were transient without need for change in therapy; as intermediate if they required treatment but did not inflict long-term consequences; or severe if they inclined lasting damage.
Data on study endpoints was extracted with the use of a data extraction form, designed to meet the specific requirements of this systematic review. When a study matched their non-idiopathic group to an idiopathic cohort treated at the same time with the same method, data on these idiopathic clubfeet was extracted in the same way. All collected data was pooled and overall results were calculated. Overall average number of casts was determined by calculating the average of all data on this endpoint.
Data on clubfeet associated with arthrogryposis and spina bifida was evaluated separately. This includes all feet of patients diagnosed with arthrogryposis or spina bifida according to the study's protocol. No further classification was made based on subtype of arthrogryposis or spina bifida.
The Methodological Index for Non-Randomized Studies (MINORS) was used to assess the methodological quality of the selected studies. 15
Results
After searching PubMed and Limo for potentially relevant studies, 21 articles were selected based on title and abstract. Of these studies, 18 met the initial inclusion criteria. One additional study was identified by reviewing the reference lists of the selected articles. The articles were then screened for the above mentioned additional inclusion criteria. In all, 11 articles were eventually included in this systematic review (Fig. 1).7,16–25 The MINORS of each article was calculated which yielded scores ranging from 11/16 to 12/16 for non-comparative studies and from 18/24 to 21/24 for comparative studies. Because of the limited amount of studies reporting results on treatment of non-idiopathic clubfeet with the Ponseti method, all studies were included regardless of the MINORS.
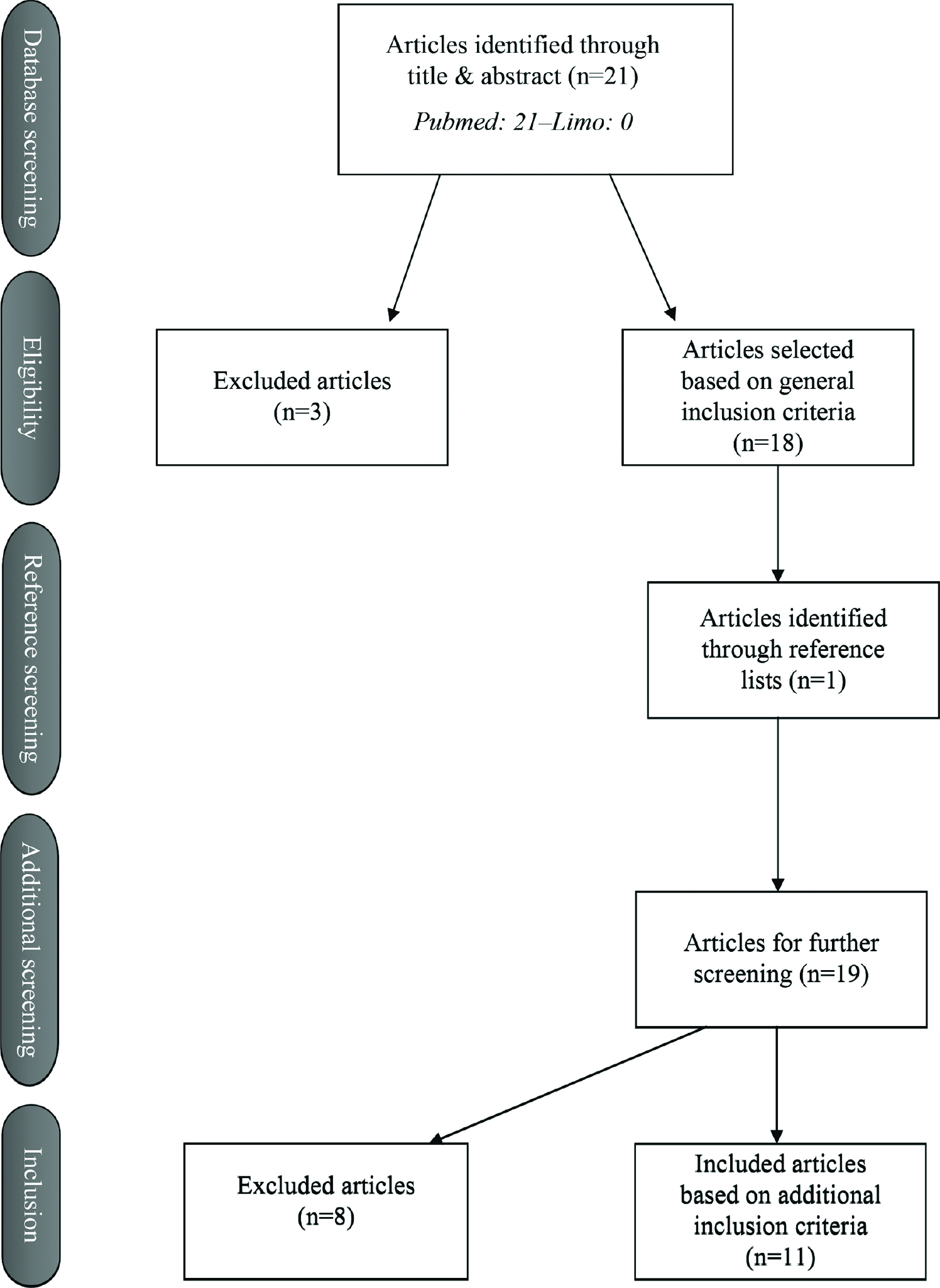
Flow Diagram.
Non-idiopathic
Baseline characteristics and results of the 11 included articles are presented in Table 1. Overall results are shown in Table 2. Kowalczyk et al20,26 published two articles on this topic, one in 2008 and one in 2015. The first study from 2008 was not included since its data are presumably included in their study from 2015. Pooling of data yielded a recurrence rate of 43.3%. Six studies reported causes for recurrence and these include noncompliance or intolerance with bracing protocol, reduced evertor muscle function, severity of deformity and concurrent deformities. Complications were found in 30 non-idiopathic clubfeet (20.3%) of which 19 feet were classified as having mild complications since they presented with blistering, skin hyperaemia or swelling. Intermediate complications were seen in 11 feet. These feet presented with iatrogenic fractures, cast slippage, sores or skin breakdown and required a change in treatment.
Baseline characteristics and results on non-idiopathic clubfeet
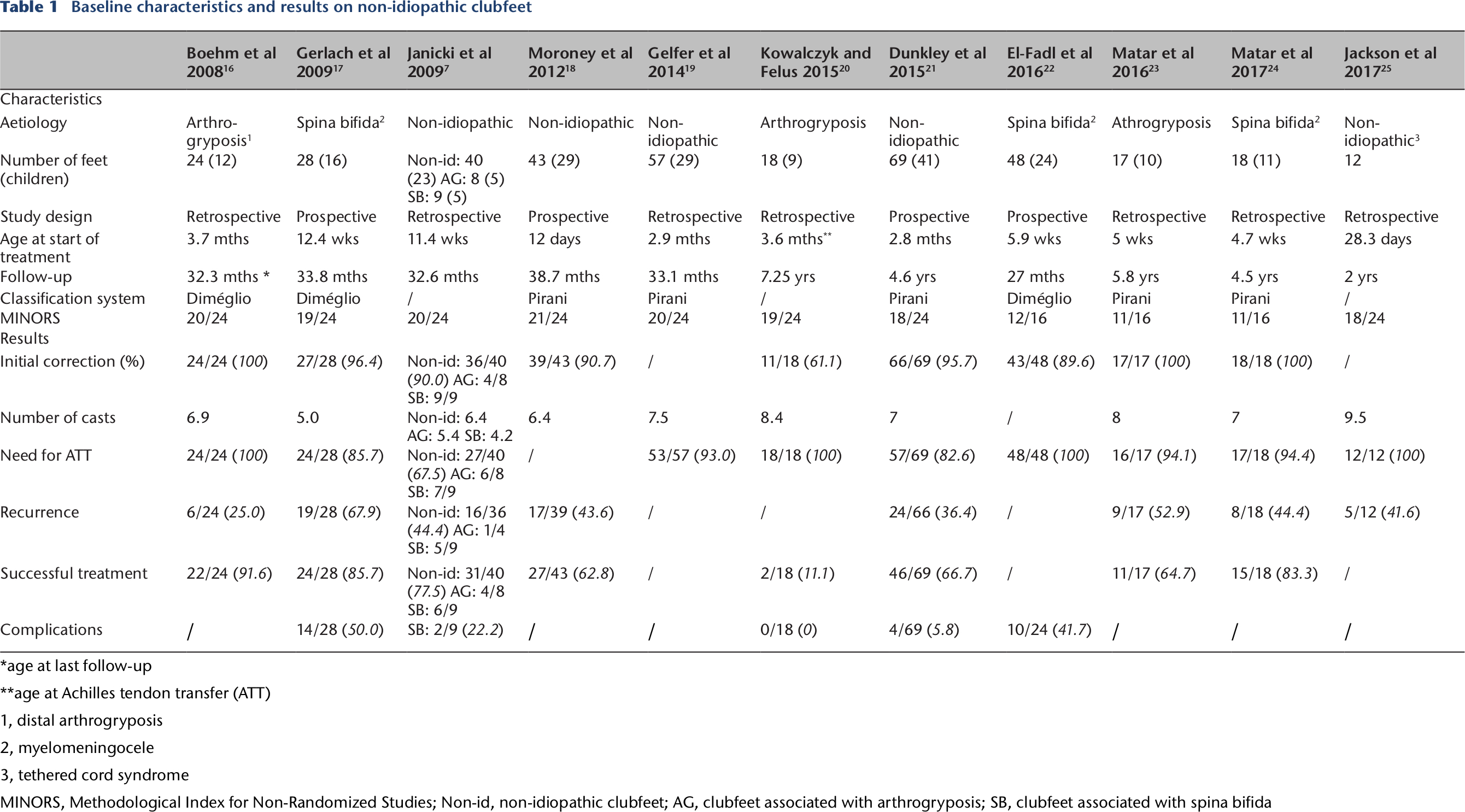
age at last follow-up
age at Achilles tendon transfer (ATT)
distal arthrogryposis
myelomeningocele
tethered cord syndrome
MINORS, Methodological Index for Non-Randomized Studies; Non-id, non-idiopathic clubfeet; AG, clubfeet associated with arthrogryposis; SB, clubfeet associated with spina bifida
Overall results on non-idiopathic clubfeet, clubfeet associated with arthrogryposis and clubfeet associated with spina bifida
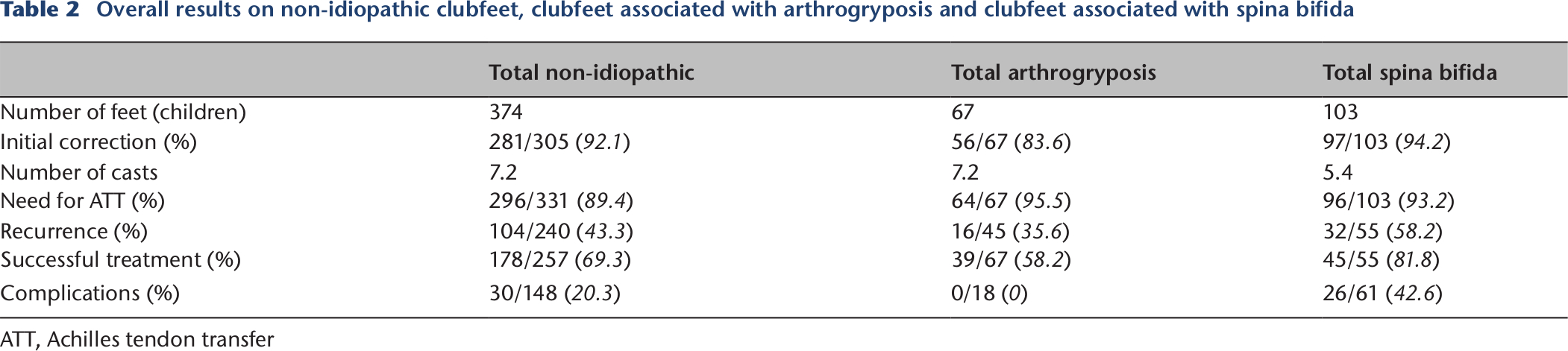
ATT, Achilles tendon transfer
Seven of the included articles matched their group of non-idiopathic clubfeet with a cohort of isolated idiopathic clubfeet treated at the same time with the same method.7,16–19,21,25 The baseline characteristics and results of the idiopathic group are presented in Table 3, together with the overall results. Eight feet (7.1%) presented with complications. Of these feet, five showed blistering and were classified as having mild complications. Intermediate complications in form of sores were found in the other three feet.
Baseline characteristics and results of separate articles on idiopathic clubfeet and overall results on idiopathic clubfeet
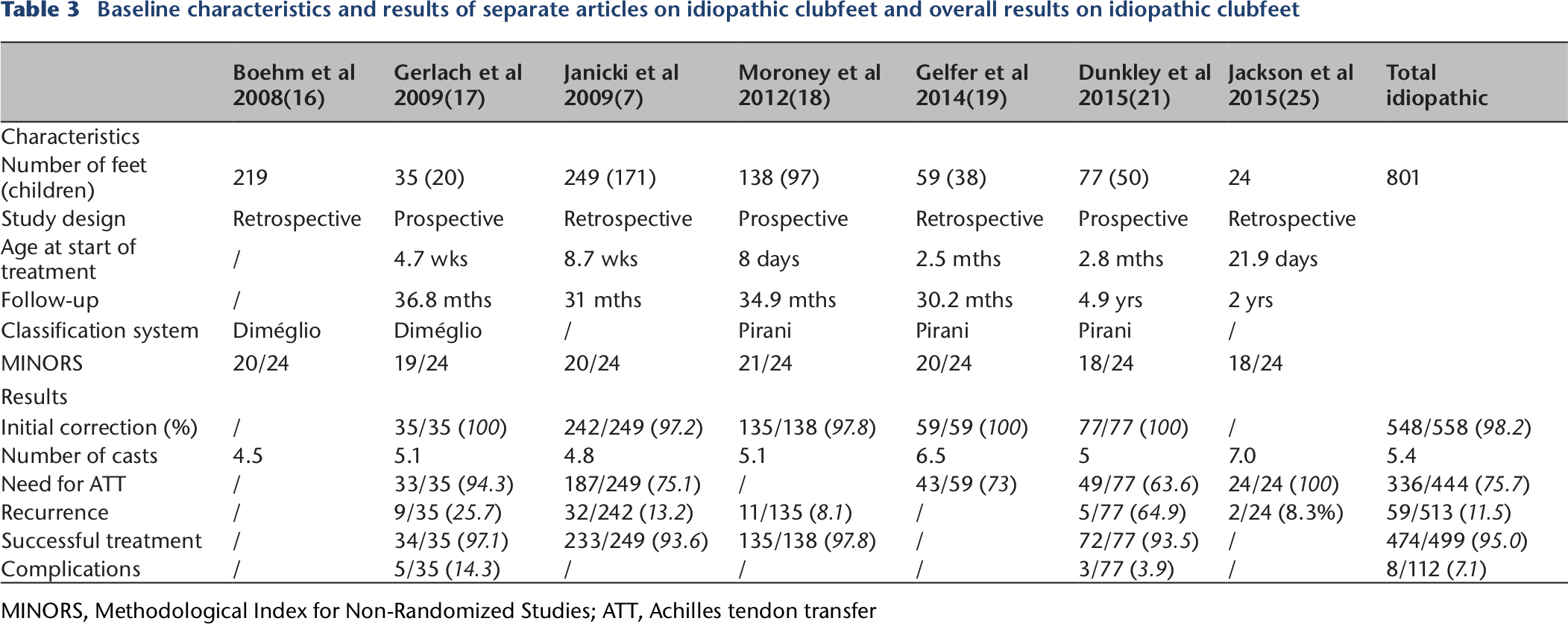
MINORS, Methodological Index for Non-Randomized Studies; ATT, Achilles tendon transfer
Arthrogryposis
Four of the included studies documented on non-idiopathic clubfeet in children diagnosed with arthrogryposis.7,16,20,23 The results of these studies were pooled (see Table 2). Only one of these articles studied the occurrence of complications and found no complications in feet that were treated solely with the Ponseti method.
Spina bifida
Four articles reported data on non-idiopathic clubfeet associated with spina bifida specifically.(7,17,22,24) Pooled results are summarized in Table 2. Complications were found in 26 feet (42.6%). Out of these 26 feet, 21 feet presented with mild complications, such as blistering, skin breakdown and skin hyperemia and swelling. Two feet with iatrogenic fractures and three feet with cast slippage required additional treatment and these were classified as having intermediate complications.
Discussion
Since its development and implementation in 1963, 27 the success of the Ponseti method in the treatment of idiopathic clubfeet has been widely accepted and confirmed.8–13 Its use in the treatment of non-idiopathic clubfeet remains, however, controversial. This systematic review reports results on treatment with the Ponseti method in non-idiopathic clubfeet. Initial correction was achieved in almost all clubfeet (92.1%) after an average of 7.2 casts. A high recurrence rate of 43.3% was found, although most of these relapsed feet could be successfully corrected with repeat casting and ATT only. This yielded successful treatment in 69.3% at final follow-up.
When compared with the idiopathic cohort, outcomes in non-idiopathic clubfeet were inferior to those in children with isolated clubfeet. Idiopathic clubfeet needed on average fewer casts to obtain correction (5.4 versus 7.2) and required less often ATT after casting (75.7% versus 89.4%). Lower recurrence rates were found in idiopathic clubfeet (11.5% versus 43.3%), as well as a higher rate of successful treatment at final follow-up (95.0% versus 69.3%). These findings are to be expected since non-idiopathic clubfeet are known to be more rigid and often present with other abnormalities which can complicate treatment of the clubfoot.
Although the Ponseti method is the benchmark of treatment in idiopathic clubfeet, 28 the best treatment method of non-idiopathic clubfeet remains to be established. Until recently, these feet were often corrected using surgical methods such as soft-tissue release (STR) and osteotomy. STR is viewed as the preferred treatment in younger children, whereas osteotomies are reserved for older children or as a salvage procedure in severe, rigid clubfeet that failed primary treatment.29,30 Serial casting and primary STR of non-idiopathic clubfeet yielded successful correction without recurrence after an average follow-up period of 15.4 years in 25.5% according to a study by Kowalczyk and Felus. 20 The same authors reported a complication rate of 23.0%. Flynn et al 29 found good results in 62.5% after serial casting and primary STR of non-idiopathic clubfeet. The average follow-up period was 96 months. Complications were found in 15.3%. Widmann et al 31 reported good results in 50% of cases after an average follow-up period of 4.3 years and Niki et al 32 in 46.3% after an average follow-up period of 118 months following treatment of non-idiopathic clubfeet with serial casting and primary STR. We report successful primary treatment of non-idiopathic clubfeet with the Ponseti method in 69.3% after a minimum follow-up period of two years and a complication rate of 20.3%. Surgery is a valuable, and often the only, option in older children with clubfeet, since they present with more foot stiffness and more advanced bone deformities. 29 However, the Ponseti method with or without ATT is a non-invasive treatment option with comparable short-term results with surgical interventions when used as primary treatment method in young children. The main issue remains a high recurrence rate (43.3%). Although most recurrences were successfully corrected using repeat casting and/or ATT only, more research with longer follow-up is necessary to evaluate the long-term effect of the Ponseti method in non-idiopathic clubfeet.
The most common aetiologies associated with non-idiopathic clubfeet are arthrogryposis and spina bifida.6,7 Better results were found in clubfeet associated with spina bifida when compared with arthrogrypotic clubfeet. Clubfeet associated with spina bifida needed on average less casts to obtain correction (5.4 versus 7.2) and presented with a higher rate of successful treatment at final follow-up (81.8% versus 58.2%). However, they did have a higher recurrence rate compared with arthrogrypotic clubfeet (58.2% versus 35.6%). These differences can be partly explained by heterogeneity in baseline characteristics between the different study groups. In addition to this, it is very likely that differences in disease characteristics also account for the discrepancies we found. Spina bifida is associated with motor paralysis or spasticity and sensory loss, which probably leads to the higher recurrence rate. Arthrogryposis is characterized by contractures in at least two different areas of the body with often very stiff clubfeet. 33 This accounts for the higher number of casts needed for correction and the lower rate of successful treatment at final follow-up. Non-idiopathic clubfeet are often viewed as a whole and categorized as one group, while they are in fact associated with a broad range of different aetiologies. More research is needed to study the influence of the different aetiologies associated with non-idiopathic clubfeet on treatment outcomes.
Only five of the eleven included articles report on complications occurring in feet treated with the Ponseti method. Gerlach et al 17 found complications in 50% of their study cohort, of which 64.3% was classified as mild and 35.7% as intermediate. All healed without long-term consequences. Janicki et al 7 report intermediate complications in two out of nine clubfeet associated with spina bifida (22.2%). Complications were found in 5.8% in a study from Dunkley et al 21 and all were classified as intermediate. El-Fadl et al 22 saw complications occurring in 41.7% and all were classified as mild. Kowalczyk and Felus 20 report one complication after revision STR but none in clubfeet treated solely with the Ponseti method. Non-idiopathic clubfeet are thought to be at higher risk to develop complications such as pressure sores and pathologic fractures because they often present with sensory loss and more severe contractures. 34 More research is necessary before conclusions can be drawn on this topic.
We found a recurrence rate of 43.3% after treatment of non-idiopathic clubfeet with the Ponseti method. Six out of the included studies report causes for recurrence. The reported causes are multiple and include noncompliance or intolerance with bracing protocol, reduced evertor muscle function, severity of initial deformity and concurrent deformities. Because of the limited data, further research is needed. We suggest studies with prospective collection of data on causes of recurrence after treatment of non-idiopathic clubfeet with the Ponseti method since this would provide valuable, reliable and relevant information on the management of these feet.
This study has several limitations. Due to restriction of our literature search to the English language, it is possible that not all studies on use of the Ponseti method in non-idiopathic clubfeet were included. This also limits our conclusions as they may not be applicable to all ethnicities. In addition, publication or reporting bias cannot be ruled out since abstract-only articles were excluded and this may have caused elimination of studies with negative findings that did not become full-text publications. Furthermore, results of 11 articles with different baseline characteristics were pooled and this heterogeneity limits the power to draw general conclusions from our findings. Finally, many of the included articles have low MINORS scores, small sample sizes, short follow-up periods and are retrospective in study design, which naturally affects the quality of this review.
The strengths of this review are that it is the first to systematically summarize current evidence on treatment of non-idiopathic clubfeet with the Ponseti method and that it highlights the importance of further research on this topic. Additionally, the MINORS score was used to assess methodological quality of the included studies, which allowed for more objective assessments.
In conclusion, the Ponseti method is a valuable option for the treatment of non-idiopathic clubfeet. It is a non-invasive treatment method with comparable short-term results with surgical interventions when used as primary treatment in young children. Studies with longer follow-up are necessary to evaluate its long-term effect.