
Abstract
Background
The outcomes movement has emphasized the importance of the patient in evaluating treatment outcome. However, concern has been raised about the ability of children, particularly those with multisystem disease, to evaluate their disability.
Purpose
To determine whether children with spina bifida and muscular dystrophy and their parents agree when asked about the relative difficulty of daily activities and the severity of symptoms experienced by the child.
Methods
First, a list of symptoms and activity restrictions was generated from the literature, clinicians, and interviews with families with spina bifida and muscular dystrophy. Second, another group of parents and children with spina bifida (with hip dislocation or scoliosis) and with muscular dystrophy (with scoliosis), including those before and after surgery, independently rated the severity and importance of their objective and subjective complaints.
Results
The correlation between parents and their children was high for both objective (median Spearman's = 0.70; standard deviation [SD] = ±0.17; range = −0.05–1.00) and subjective (median Spearman's = 0.76; SD = ±0.14; range = 0.13–1.00) complaints, with an overall excellent level of agreement (Kappa = 0.75; 95% confidence interval [CI]: 0.73, 0.76).
Conclusion
Children with spina bifida and muscular dystrophy are capable of understanding and assessing their disability.
Introduction
Quality of life and health status are important components of a complete evaluation of orthopaedic interventions. The orthopaedic literature is replete with health outcome scales and few treatment evaluations would be complete without an assessment of health status or quality of life [1, 2]. Health-related quality of life describes the impact of disease or illness from the individual patients’ perspective [3]. Because clinicians may consider and put values on states of ill health differently than their patients [3], it is important to assess the concerns of patients to gain an accurate appraisal of success.
While evaluating adults is relatively straight forward, the measurement of health status in children poses specific challenges. First, children, particularly those younger than 8 years of age, may not be able to read or understand questionnaires. Second, it is uncertain whether the appraisal of health status should be based on the opinions of parents or children. Third, it is uncertain whether children with chronic multisystem diseases like spina bifida and muscular dystrophy are able to assess their health status.
The purpose of this study was to determine whether children and parents agree when asked about the relative difficulty of daily activities and severity of symptoms experienced by children with muscular dystrophy and spina bifida. We chose to evaluate these two conditions because many of these children have orthopaedic surgery at some time during their life.
Materials and methods
Spina bifida is often complicated by hip dislocation and scoliosis [4, 5]. The role of surgery for these conditions is controversial. Children with spina bifida achieve lower performance scores on intelligence tests as a function of the level of lesion [6, 7]. Children with Duchenne's muscular dystrophy, a genetically determined disorder characterized by progressive degeneration of skeletal muscle [8], lose the ability to walk in childhood and later develop scoliosis. While steroids may alter the prevalence of scoliosis, many of these adolescents receive spinal instrumentation and fusion. Cognitive delays, present in many of these children, is believed to be linked to specific missing dystrophin isoforms [9].
In the first stage of this study, we developed a list of concerns relevant to parents and children with spina bifida and muscular dystrophy. The rationale for these three scales was the lack of disease-specific scales to evaluate treatment effectiveness [10–12]. In both stages of the study, English-speaking families were selected, based on the irrespective of the children's cognitive abilities, the presence of scoliosis more than 10° in children with spina bifida and muscular dystrophy, and dislocated hips in children with spina bifida. Briefly, we first performed a literature review. Second, we interviewed orthopaedic surgeons, paediatricians, nurses, physical therapists, and occupational therapists. Finally, we also interviewed families concerning the difficulties faced in performing daily activities and the severity of problems experienced by these children. From those multiple sources, we eliminated overlapping or redundant concerns to create 241 questions concerning symptoms and functional disabilities potentially important to parents and children with muscular dystrophy with scoliosis, spina bifida with scoliosis, and spina bifida with dislocated hips [10–12].
In the second stage of the study, we interviewed separate groups of parents and children, with the inclusion noted above for patients with muscular dystrophy and spina bifida (with dislocated hips or scoliosis). Parents and children responded to each question using a standard five-point Likert scale, along with a sixth category (for not applicable). Parents and children separately and independently rated each concern for both difficulty/severity and importance. For example, if the question was “how difficult is it to go up stairs,” the options would be; not difficult, a little difficult, moderately difficult, very difficult, and unable to do. The same question would then be asked in the second section as “how important is it to go up stairs” and the options would be; not important, a little important, moderately important, very important, and extremely important.
We further subcategorized questions as objective (i.e., externally perceived, such as walking ability) and subjective (i.e., perceived only by the child, such as pain) questions (Table 1). The exact breakdown and number of questions for each questionnaire are displayed in Table 2.
Examples of the types of questions asked for each disease group
These same questions were also asked in terms of their relative importance
Number of questions divided by category
Represents objective and subjective questions from both severity and importance categories
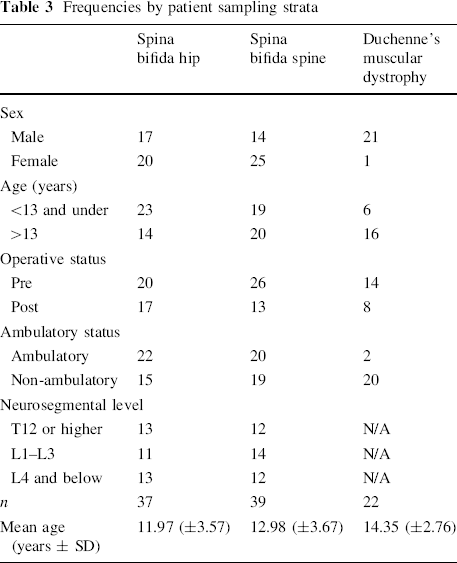
For each patient, we also recorded their age, sex, operative history, hip status, and ambulatory devices used. Children were sampled using three strata; sex, age (<13 or >13 years), and operative status (pre-op or post-op) (Table 3) to ensure that a broad range of concerns were addressed. Because children may gain weight during puberty, leading to a decline in function, or may have a change in self-image, hastening a shift to full-time chair use, we deemed it important to evaluate both pre- and post-pubertal children. Operative status was used in order to consider concerns and issues experienced by both pre-op and post-op patients.
Frequencies by patient sampling strata
Analysis of correlation was carried out for each question using Spearman's test because the data were ordinal. Median correlations were reported across all subcategories of questions. The level of agreement between each child and their respective parent was determined by using the Kappa statistic (a chance-corrected measure of agreement for categorical data). The independent estimates of Kappa were combined into an overall score with respective confidence intervals (CIs). In subsequent analyses, we confirmed that the questionnaires demonstrated test–retest reliability and construct validity, thereby, confirming the ability of patients to reliably respond to the questions and the validity of those responses [13–15].
Results
The number of patients and sampling strata are represented in Table 3. Ten pairs were not included in the statistical analysis because of missing responses from either the parents or child.
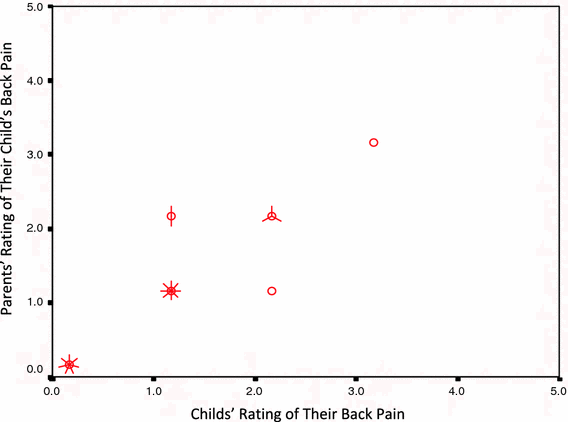
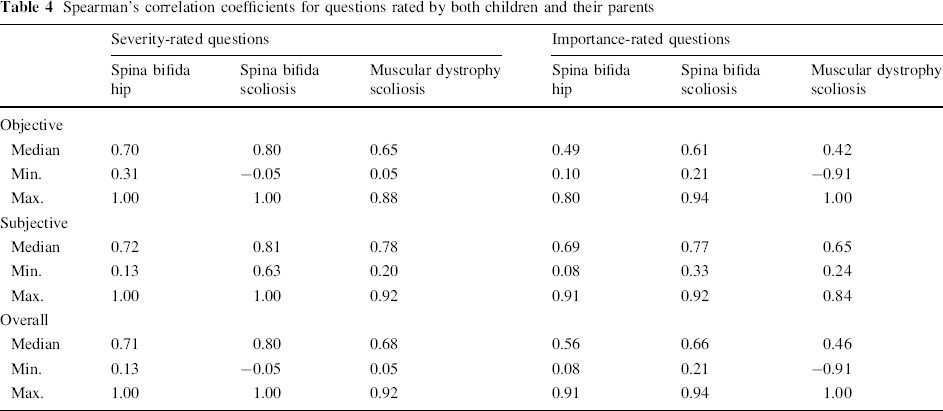
A strong positive relationship was found (median Spearman's correlation coefficient = 0.67; scores ranged from −0.91 to 1.00) for all questions across all three disease entities. The median Spearman's correlation coefficient across all questions for the spina bifida hip questions was 0.66 (with scores ranging from 0.08 to 1.00), for spina bifida spine 0.73 (with scores ranging from −0.05 to 1.00), and for muscular dystrophy 0.58 (with scores ranging from −0.91 to 1.00). Scatter plots (Figs. 1 and 2) provide an illustration of the strength of correlations for individual questions. A strong positive correlation coefficient was found for both objective- and subjective-rated severity questions across each of the three disease entities (Table 4). Lower correlations were found for the rating of importance of activities or problems faced by the children on a daily basis (Table 4).
Scatter plot showing a moderate correlation for a spina bifida hip question that asked about the relative difficulty of wheeling oneself in their wheelchair. The circles indicate a single parent–child pair, with each line emanating from them indicating additional child–parent pairs Scatter plot showing a strong correlation for a muscular dystrophy scoliosis question that asked about the relative severity of pain in their back while sitting out of their wheelchair. The circles indicate a single child–parent pair, with each line emanating from them indicating additional child–parent pairs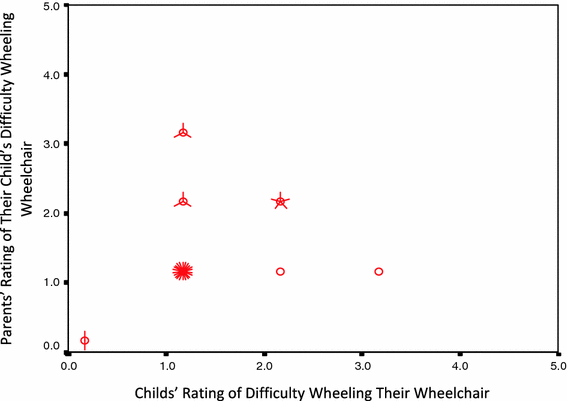
Spearman's correlation coefficients for questions rated by both children and their parents
An ‘excellent’ level of agreement (Kappa = 0.75; 95% CI 0.73–0.76) was found between parents and their children. An excellent level of agreement was also found between parents and children with spina bifida hip and spina bifida scoliosis, and moderate agreement was found between parents and children with muscular dystrophy (Table 5).
Levels of agreement between parents and children for each disease entity
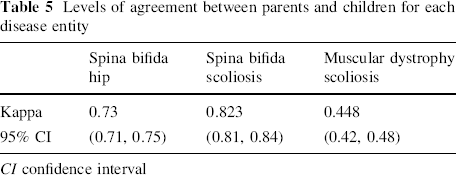
CI confidence interval
Discussion
Health-related quality of life is an essential and important component in the evaluation of treatment in children. One of the key issues in assessing health status in the paediatric population is whether to judge therapy based on the ratings of parents or children. Agreement between parents and children is reassuring in evaluating therapy. Furthermore, strong correlations between parent and children responses is generally assumed to indicate that children are competent reporters of their disease state.
Few studies have investigated the degree of parent and child agreement for concrete physical symptoms as well as more subjective features, such as pain. In rheumatology patients, parents and children have generally agreed when asked about physical function [14, 15]. Thus, prior authors have concluded, based on high agreements between parents and children, that children are capable of expressing and rating the extent of their musculoskeletal activity restrictions.
Children and parents, however, do not always agree in their appraisal of subjective concerns. Doherty et al. [2] studied agreement when asking questions regarding musculoskeletal pain for rheumatologic diseases and found low levels of agreement. Herjanic et al. [5] used a structured interview concerning facts, behavior, psychiatric symptoms, and mental status. Although Herjanic et al. found that children do describe themselves in terms similar to those used by their parents [16], a later study using a standard psychiatric questionnaire answered both by mothers and their children found high levels of agreement only for those questions concerning symptoms that were concrete, observable, severe, and unambiguous. Low agreement was found for questions that judged the severity of a problem and subsequent behaviors. Thus, low agreement for subjective psychiatric symptoms raises concerns about who should be the respondent.
The generally high overall agreement found in this study for the severity rating, both for subjective and objective concerns, is reassuring. These findings suggest that children with spina bifida and muscular dystrophy are able to accurately assess their activity restrictions. Furthermore, this suggests that parents are able to provide accurate assessments of their children's activity restrictions. Thus, in evaluating therapy, either parents’ or children's appraisal would be appropriate.
The area where parents and children diverged most was in the rating of the importance of their concerns. While the correlations were moderate, this divergence was most apparent in the Kappa statistics for the muscular dystrophy patients. The origin of these differences is not apparent from this study and will require further investigation. When children and parents disagree, the question is whose appraisal is the most accurate. In the development of the Activity Scale for Kids (ASK) [12], a questionnaire that aims at assessing what children with activity limitations are able to do and what they think they are capable of doing, Young et al. found that children were able to distinguish between different aspects of their disability and were just as good or better than their parents at articulating their activity restrictions in open-ended interviews [12]. Herjanic et al. also found that children, when questioned directly about psychiatric issues, did not hesitate to report subjective symptoms or experiences usually considered to be unusual or strange. Both groups suggested that children may be the best sources of information for research requiring the answers to very personal questions relative to themselves. When making decisions about treatment, it is essential to know that the importance attached to symptoms and activities is quite important. Thus, children, particularly those in their teens, should be included in discussions of surgeries that may have an impact on their functional abilities because, in this area, their opinions and choice of therapy may differ from their parents.
The main limitation of this study is that we did not formally assess the cognitive capabilities of our sample group. However, because the children in this study were typical of children with spina bifida and muscular dystrophy, they would have had the range of cognitive abilities found in these patients.
In conclusion, the strong level of agreement between parents and children suggests that children with spina bifida and muscular dystrophy are capable of understanding their health status. The wide variations in the responses to certain questions and their relative importance suggests that children should be considered in situations where there are differences in the opinions between parents and their children on aspects of their functional abilities, disease symptoms, or when choosing therapy.
Footnotes
Acknowledgments
The manuscript is based on the combined findings from three separate studies. Each study had its own funding source but all grants were used for salary support. The studies were entitled; “Measuring the functional outcome of spine surgery in children with spina bifida,” funded by the Spina Bifida Association, “Measuring functional outcomes of spine surgery in children with muscular dystrophy,” funded by The Easter Seals Research Institute, and “Measuring functional outcome of hip surgery in children with spina bifida,” which was funded by Physician Services Incorporated. In addition to these, a portion was also supported by the Samuel Lunenfeld Research Summer Student Program, which was provided through our institution.
None.