
Editorial
Unexpected survivors in extracorporeal membrane oxygenation – When the margins of life expand
Justyna SwolORCID
Select search scope: search across all journals or within the current journal
The Extracorporeal Life Support Organization (ELSO) has progressively transformed its guideline framework to meet the increasing clinical, scientific, and operational demands of modern extracorporeal life support. Since its establishment in 1989, ELSO has supported Extracorporeal Membrane Oxygenation (ECMO) programs worldwide through education, data reporting, and consensus-building. Recent expansions in ECMO utilization, coupled with rapidly growing evidence, have necessitated a more structured, transparent, and internationally representative approach to guideline development.
In 2023, ELSO expanded the Guideline Subcommittee (GSC) to ensure participation from all ELSO chapters and key professional disciplines. This expansion enables the implementation of a standardized workflow encompassing proposal submission, methodological review, authorship requirements, external peer review, plagiarism screening, and final Board approval. The updated process emphasizes consistency, timely production, and methodological rigor across all ELSO guidelines.
This manuscript summarizes the current ELSO guideline development process and highlights four recently published guidelines addressing early mobility, adult neuromonitoring, ECMO in pregnancy and the peripartum period, and accidental hypothermia. Each guideline reflects the available evidence integrated with multidisciplinary expert input, with the goal of providing globally applicable, practical recommendations for ECMO clinicians. The review also outlines the formal guideline update cycle and ELSO’s expanding collaborations with international societies to produce joint guidance documents.
As ECMO practice continues to evolve, ELSO remains committed to advancing high-quality, accessible guidelines that support consistent standards of care across diverse healthcare systems. Future priorities include guidelines on ECMO during cardiopulmonary resuscitation, trauma, and other high-impact clinical areas, along with enhanced education and training pathways to strengthen ECMO practice globally.
Extracorporeal membrane oxygenation (ECMO) provides life support for patients with refractory cardiac or respiratory failure. The complexity of ECMO management and associated mortality necessitates high-accuracy clinical decision-making systems. Artificial intelligence (AI) has emerged as a potential approach to address challenges in ECMO management, from patient selection to real-time assessment and outcome prediction.
To synthesize the current evidence of AI application in adult ECMO, addressing predictive modelling for patient outcomes, real-time decision support systems, and complication prevention, as well as the evolving regulatory challenges governing medical AI deployment in critical care settings.
A narrative literature review was conducted across PubMed/MEDLINE, Embase, Cochrane Library, IEEE Xplore, and preprint servers (arXiv/medRxiv). The search strategy combined ECMO-relevant terms (“V-A ECMO”, “V-V ECMO”) with AI terminologies (“artificial intelligence”, “machine learning”, “deep learning”, “digital twin”). Studies were included if they focused on adult cohorts (age ≥18 years) and were published in English between 2018 and 2025.
The review found several AI algorithms under development for different stages of ECMO therapy. AI algorithms have been developed to assist in the initiation, prognostication, complication detection, real-time control, and weaning of ECMO. However, none have been clinically translated thus far.
While AI for precision ECMO management is promising, several prerequisites remain unmet, including the integration of high-frequency device data, prospective external multicenter validation, and the development of robust regulatory frameworks. Securing these advances will bridge the gap between algorithm development and the clinical arena.
Pediatric extracorporeal membrane oxygenation (ECMO) is a highly complex therapy characterised by rapidly evolving physiology, high complication rates, and substantial cognitive demands on multidisciplinary teams. Management requires continuous integration of physiologic, laboratory, ventilatory, and circuit-derived data to support time-critical decisions related to gas exchange, haemodynamics, anticoagulation, transfusion, circuit surveillance, and weaning. Despite technological advances and growing international standardisation, morbidity and mortality continue to be driven by neurologic injury, bleeding and thrombosis, and clinical factors influencing successful liberation from ECMO support.
To review contemporary artificial intelligence (AI) and machine learning (ML) applications relevant to pediatric ECMO and evaluate their potential role as clinically aligned decision-support tools for clinicians and ECMO practice.
A narrative review of English-language literature (2020–2026) was conducted using PubMed, MEDLINE, and Scopus to identify AI/ML studies, systematic reviews, and guideline documents addressing pediatric ECMO outcomes, complication prediction, circuit surveillance, and weaning or decannulation support, as well as methodological and governance frameworks relevant to clinical implementation.
Most ECMO-AI applications employ supervised learning or deep learning approaches integrating demographic, clinical, laboratory, and ECMO device time-series data. Recent studies demonstrate emerging promise for neurologic risk prediction, bleeding and transfusion risk forecasting, circuit anomaly detection, and dynamic assessment of weaning readiness. Progress has included registry-based analyses, externally validated pediatric models, and time-series frameworks aligned with clinical workflows. However, heterogeneity in data quality, outcome definitions, and validation strategies remains substantial.
AI-guided tools in pediatric ECMO are transitioning from early feasibility studies toward more mature, clinically aligned decision-support applications. With rigorous validation, transparent reporting, and strong governance, AI has the potential to enhance situational awareness and consistency of care while preserving the central role of expert multidisciplinary judgement.
Extracorporeal Life Support (ECLS) services are characterised by variability in resource availability, specific expertise, device management and team organisation, especially regarding the role of perfusionists. This international survey aimed to investigate perfusionists’ education, training and role within the ECLS team.
This is a descriptive, self-reporting, cross-sectional, voluntary, confidential international survey addressed to professionals involved in ECLS management, including perfusionists. The survey was distributed from April to August 2025 through congress, newsletter and social media platforms.
A total of 178 ECLS centres submitted completed surveys. Most centres provided both cardiac and respiratory support (
This international survey revealed marked variability in perfusionist education, training and roles within the ECLS teams, and related organization. Despite their technical responsibilities, a growing multidisciplinary collaboration is reshaping team dynamics. The absence of a standardized education remains a critical gap, requiring appropriate actions and planning by professional and scientific societies.
The HEART-UA (Healthcare Extracorporeal Assessment and Resource Tracking in Ukraine) survey represents the first nationwide evaluation of extracorporeal life support (ECLS) and renal replacement therapy (RRT) availability in Ukraine. The study aimed to systematically characterize national ECLS and RRT capacity, assess temporal changes before and during the conflict, and identify major operational limitations affecting access to extracorporeal organ support.
A structured cross-sectional survey was conducted among Ukrainian hospitals providing ECLS and/or RRT. Data collection included institutional characteristics, ECMO device availability, case volumes in 2021 and 2023, staffing models, barriers to ECLS provision, and the availability of CRRT and intermittent hemodialysis. Responses were clustered at the institutional level, and duplicates were merged. Categorical variables were compared between the pre-war and wartime periods using Fisher’s exact or chi-squared tests where appropriate.
Twenty-two institutional responses were analyzed, including 15 ECLS centers, 16 CRRT centers, and 19 IHD-capable institutions. Geographical distribution showed regional clustering of ECLS resources. No statistically significant expansion in ECMO device availability or procedural volumes was observed between 2021 and 2023. The predominant barriers to ECLS provision included shortages of consumables (60%), insufficient trained personnel (53%), and inadequate numbers of ECMO devices (47%). CRRT availability was higher, but most centers reported major limitations due to shortages of consumable circuits, machine availability, and infrastructural instability. Humanitarian aid related to extracorporeal support was received by only 27% of institutions and was irregular, fragmented, and insufficient to meet national needs.
The HEART-UA survey demonstrates that Ukraine’s capacity to provide extracorporeal organ support has remained critically constrained during the war. Device availability, trained personnel, and consumable supply chains are still major limiting factors. Although many centers continue to provide lifesaving ECLS, CRRT, and IHD despite extreme operational challenges, the overall system is highly dependent on inconsistent humanitarian aid.
Despite major advances in temporary mechanical circulatory support (tMCS), cardiogenic shock remains associated with high mortality. Early management strategies were dominated by the intra-aortic balloon pump (IABP), widely adopted on physiological grounds despite limited randomized evidence and later declining use due to downgraded guideline recommendations. Subsequent shifts toward more potent tMCS devices, including transaortic micro-axial flow pumps and venoarterial extracorporeal membrane oxygenation (VA ECMO), were driven by the pursuit of improving systemic perfusion and ventricular unloading. However, enhanced hemodynamic support has not consistently translated into superior clinical outcomes and is frequently accompanied by substantial device-related complications. Increasing recognition of the complex and patient-specific physiology of cardiogenic shock has fueled a transition from device-centred to patient-centred strategies, emphasizing tailored support configurations, multimodal monitoring, and physiology-driven decision-making. Adjunct left ventricular unloading during VA ECMO has emerged as a promising yet controversial approach, with ongoing trials expected to clarify its clinical role. Recent evidence, including the DanGer Shock trial, suggests that timely initiation of appropriately selected tMCS may improve longer-term outcomes in selected populations. Parallel advances in biomedical engineering have enabled physiology-based cardiovascular simulators that allow systematic comparison of tMCS strategies, pharmacological support, and device hemocompatibility under controlled conditions. When extended to virtual populations, these in silico approaches can complement clinical evidence through virtual clinical trials, potentially reducing the size and cost of traditional studies. Together, these developments highlight a new era of patient-centred critical care and biomedical innovation in cardiogenic shock.
Post-cardiotomy cardiogenic shock (PCCS) remains one of the most lethal complications of cardiac surgery, with high in-hospital mortality despite major improvements in operative techniques, and intensive care management. Temporary mechanical circulatory support (tMCS) is widely applied as a rescue therapy for refractory PCCS. However, outcomes remain suboptimal, also due to delayed initiation after the onset of severe hemodynamic collapse and irreversible compromised end-organ states. This review summarizes current concepts of PCCS management and evaluates the emerging role of prophylactic tMCS within the framework of “protected cardiac surgery”.
A narrative review of the current international guidelines, expert consensus statements, and major observational studies addressing post-cardiotomy tMCS and prophylactic support strategies was carried out. Emphasis was placed on pathophysiology, indications, timing of support, and device selection.
Prophylactic tMCS has been applied in selected high-risk scenarios including acute coronary syndromes, acute valvular dysfunction, ventricular septal rupture, papillary muscle rupture, advanced heart failure requiring bridge-to-decision or to-transplant, or difficult and complex weaning from cardiopulmonary bypass. The concepts of preoperative (Type 1), planned intraoperative (Type 2), and unplanned early intraoperative (Type 3) protected cardiac surgery provide a practical framework for a timely evaluation and related action aiming at metabolic stabilization to reduce or prevent postoperative low cardiac output syndrome. Successful implementation depends on multidisciplinary Heart Team decision-making, advanced hemodynamic assessment, and tailored perfusion strategies as well as device selection also based on local resources and expertise.
Prophylactic tMCS represents a paradigm shift from reactive rescue therapy toward proactive cardio-circulatory protection in selected high-risk patients undergoing cardiac surgery procedures. While early observational data are encouraging, prospective trials, standardized risk stratification tools, and cost-effectiveness analyses are required to define its role in modern cardiac surgery.
Venovenous extracorporeal membrane oxygenation (VV ECMO) is a potentially lifesaving yet resource-intensive organ support option for patients with very severe respiratory failure refractory to optimized conventional management. Mortality remains high, and ECMO is associated with significant complications, including bleeding, thrombosis, and vascular injury. Indication and timing of ECMO initiation are critical, as premature and also delayed use can affect outcomes. Current evidence, including findings from the CESAR and EOLIA trials and subsequent meta-analyses, supports the consideration of ECMO in very severe acute respiratory distress syndrome (ARDS) when lung-protective ventilation, prone positioning, and adjunctive therapies fail to ensure adequate gas exchange. Patient selection should rely on individualized risk-benefit assessment considering age, comorbidities, organ dysfunction, reversibility of lung injury, and patient-centered goals, rather than any single exclusion criterion. Management during ECMO focuses on ultra-protective ventilation to minimize ventilator-induced lung injury, early detection of complications, and tailored anticoagulation strategies, although optimal anticoagulation protocols remain undefined. When performed in experienced centres, prone positioning during ECMO is feasible and safe, but evidence for a survival benefit is inconclusive. Extracorporeal carbon dioxide removal (ECCO2R) may facilitate ultra-protective ventilation but lacks a proven mortality benefit. Therefore, its use is currently not recommended outside the setting of well-designed clinical trials. Weaning from ECMO should be structured and guided by physiological readiness while maintaining lung-protective ventilation. Optimal outcomes are achieved in high-expertise, multidisciplinary centres, with ongoing research needed to refine patient selection, ventilation strategies, and complication management. Overall, VV ECMO remains an essential tool in the management of severe respiratory failure, requiring careful balancing of risks, resources, and individualized clinical decision-making.
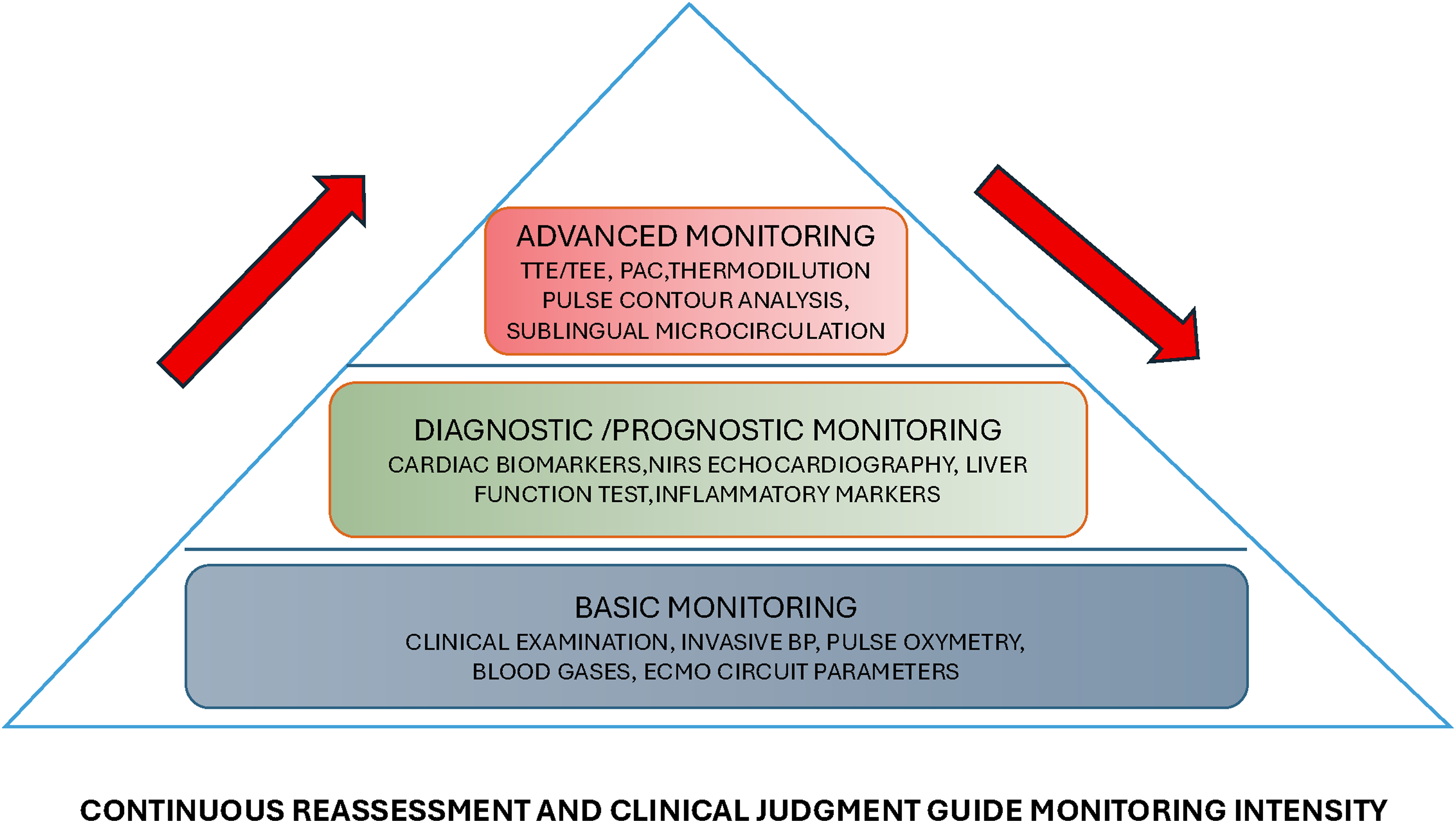
In adult patients receiving veno-venous Extracorporeal Membrane Oxygenation (VV ECMO), cardiovascular performance plays a critical role in determining oxygen delivery, organ perfusion and safe titration of extracorporeal support. Despite the increasing VV ECMO use, contemporary guidance on hemodynamic monitoring remains limited and largely experience-based. This scoping review aimed to map available basic and advanced monitoring approaches and to identify current evidence gaps.
PubMed, EMBASE, and Cochrane CENTRAL were searched from inception until September 2025, along with reference lists of relevant articles. We included studies of any design reporting techniques, targets, or protocols for hemodynamic monitoring during VV ECMO.
Of 465 records screened, 106 met inclusion criteria. No protocolized, evidence-based hemodynamic monitoring protocol specific to VV ECMO was identified. The available evidence was heterogeneous and mostly derived from physiologic studies or single-center observational cohorts. Findings were narratively synthesized across three domains: basic bedside monitoring, diagnostic/prognostic tools and advanced assessment of cardiopulmonary interaction. Across studies, no monitoring strategy consistently reduced time-to-wean or mortality. Observational data suggested that care bundles and multidisciplinary approaches may reduce complications. However, the risk of bias limits causal inference.
Despite the complex interaction between native cardiovascular function and extracorporeal circulation, VV ECMO lacks consensus on evidence-based hemodynamic monitoring pathways. A pragmatic core monitoring bundle with tiered triggers for escalation is necessary. Future priorities include implementation models based on multidisciplinary teams, specific training, standardized bundles, and multicenter studies aimed to define right ventricular-centered targets to improve safety and clinical decision-making.
Extracorporeal membrane oxygenation (ECMO) is increasingly used as an adjunct in the management of critically injured trauma patients requiring operative intervention. Although trauma represents a small proportion of overall ECMO use, its application has expanded due to advances in circuit technology, cannulation strategies, and anticoagulation practices. This review examines the role of ECMO in stabilizing operative trauma patients across preoperative, intraoperative, and postoperative phases. Preoperatively, ECMO is most commonly indicated for refractory hypoxemia or severe acidosis resulting from thoracic or airway injury, aspiration, transfusion-related acute lung injury, or acute respiratory distress syndrome. Early cannulation can restore gas exchange, improve hemodynamic stability, reduce ventilator-induced lung injury, and facilitate safe transport to the operating room during damage control resuscitation. Emerging evidence also supports selective use of ECMO in patients with traumatic brain injury requiring urgent neurosurgical intervention. Intraoperatively, ECMO has been used during high-risk damage control procedures, including trauma pneumonectomy, retrohepatic inferior vena cava injury, and operations complicated by hemorrhage, hypothermia, and acidosis. Veno-venous ECMO may improve oxygenation and reduce right ventricular strain, while veno-arterial ECMO may be appropriate in select cases of traumatic cardiogenic shock. Postoperatively, ECMO is most often employed for delayed respiratory failure due to acute respiratory distress syndrome, transfusion-related lung injury, or bronchopleural fistula, allowing lung-protective ventilation and recovery. Although evidence supporting ECMO for traumatic respiratory failure continues to grow, data for other perioperative indications remain limited. Prospective multicenter studies are needed to refine patient selection, timing, and outcomes in operative trauma populations.
Extracorporeal membrane oxygenation (ECMO) is an established life support technique for refractory acute cardiorespiratory failure in children and adult patients. However, ECMO support is provided only by specialized centers; therefore, demand for ECMO transport retrieval services is increasing. Mobile teams assess, accept, implant ECMO, and then transport for continued support at an ECMO center.
To provide an updated practical review to support ECMO teams for safe and effective transports.
We retrospectively reviewed literature limited to ECMO transport published between January 2014 to October 2025.
Forty-five manuscripts were included in this narrative review. Patient selection focused on reversible, refractory respiratory or cardiac failure not responding to maximal conventional therapy. Time to reach the referring hospital is the most frequent factor limiting the feasibility of transport; both ground ambulances and aircraft were the most common means used, depending on distance. Weather and road conditions may influence transport safety. Familiar equipment was generally used during transport, but with adaptation and certification for transport. Team experience and training were important factors for safe transport since complications frequently occurred, requiring fast decision and action. Foreign country missions required involvement of insurance, legal, and administrative support.
Regional, national, and international inter-hospital ECMO transports can be conducted safely. Preparation of ECMO transport services regarding adapted equipment, checklists, and comprehensive training for ECMO team members is essential to ensure secure transport, enabling early identification and appropriate management of adverse events. International transports operate within different regulatory frameworks and therefore require special considerations.
Hyperoxemia is associated with increased mortality and acute brain injury (ABI) in patients receiving veno-arterial extracorporeal membrane oxygenation (VA-ECMO), though the role of native cardiac function in this relationship is unclear. Pulse pressure (PP) can reflect the proximal shift of dual circulation between ECMO and native heart function. We aimed to investigate the relationship between PP, hyperoxemia, and ABI.
We included adults (≥18 years) receiving peripheral VA-ECMO for cardiogenic shock from the ELSO Registry (2013–2024).
ABI occurred in 1012/8486 (11.9%) patients. In multivariable logistic regression adjusting for demographic and clinical covariates, severe hyperoxemia (PaO2 ≥ 300 mmHg) remained independently associated with ABI (aOR: 1.40, 95% CI: 1.04–1.86). Low pulse pressure (PP) was more frequent among ABI patients, but PP was not independently associated with ABI after adjustment (aOR: 1.01, 95% CI: 0.81–1.25). PaO2 and PP were inversely related. In mediation analysis PP accounted for 8.2% of the total effect of hyperoxemia on ABI overall (14% in the non-LV-vented cohort).
Severe hyperoxemia during ECMO was associated with increased ABI risk. Low PP was not. PP mediated the relationship between hyperoxemia and ABI. Reduced cardiac function may drive proximal dual circulation shift, predisposing patients to hyperoxemia and ABI. Hyperoxemia appears modifiable, and improved PP may reduce ABI.
Refractory end-stage lung failure may benefit from extracorporeal life support (ECLS) as a bridge to lung transplantation. Venovenous (VV) extracorporeal membrane oxygenation (ECMO) is indicated in patients who have failed conventional medical treatment and mechanical ventilation. The Avalon Elite Bi-Caval Dual-Lumen Catheter (Getinge) and the Crescent Jugular Dual-Lumen Catheter (MC3, Inc., Medtronic) have been used for this configuration. Venoarterial (VA) ECMO may be used in patients with acute right ventricular (RV) failure, haemodynamic instability or refractory respiratory failure. Peripheral percutaneous approaches such as dual-site single-lumen cannulation for venopulmonary (VP) ECMO or single-site dual-lumen (dl)VP ECMO using the ProtekDuo right ventricular assist device (RVAD) cannula have been considered more recently as a bridge to transplant. These configurations support the right ventricle, prevent recirculation by placing the tricuspid and pulmonary valve between drainage and return cannulas, provide direct introduction of oxygenated blood into the pulmonary artery, and decrease the incidence of acute kidney injury (AKI) requiring continuous renal replacement therapy (CRRT) in certain disease states. This promotes haemodynamic stability and allows sedation-weaning trials, extubation, mobilisation, and pre-transplant rehabilitation. The aim of this review is the evaluation of the feasibility, outcomes and reported complications associated with dual-lumen cannulas – specifically the Avalon Elite, Crescent and ProtekDuo – used for VV and VP ECMO in adult patients requiring bridge to lung transplantation.
A web-based literature search in PubMed and EMBASE was undertaken following a combination of key words. The PICOS and PRISMA approach was used.
Nine studies were identified out of 489 articles with a total of 251 patients placed on VV or VP ECMO as a bridge to lung transplantation. The age range was 23–68 years. The duration of ECMO support ranged from 42 h to 200 days. About 60% of patients were awake and underwent mobilisation. Survival to lung transplantation ranged from 25% to 100%. All relevant data were reviewed and integrated in the discussion.
Single-site dual-lumen cannulation has an established role in VV ECMO bridging strategies and an emerging role in VP ECMO for patients with RV injury. Broader adoption of VP ECMO as a bridging strategy will require rigorous reporting and inclusion into multicentre registries to generate high-level evidence.
Post-Cardiotomy Cardiogenic Shock (PC-CS) after Mitral Valve Replacement (MVR) is a rare but severe complication, which may require ECMO for the acute phase of the illness. These PC-ECMO (Post-Cardiotomy ECMO) are particularly complex cases, as the low flow through the newly replaced valve may cause a very rapid formation of thrombus, blocking the leaflets, that worsens the blood stasis inside the left atrium, extending the thrombosis. To maintain the trans-mitral flow during PC-ECMO, three milestone should be present: the transpulmonary flow should be maintained, the blood reaching the left atrium should be free to cross the mitral prosthesis and the left ventricle should be fully unloaded. The selection of the appropriate PC-ECMO configuration should be guided by the specific functional status of the right ventricle (RV) and left ventricle (LV). When only one ventricle is failing, monoventricular support is preferable. However, when PC-CS involves both ventricles, ex-BiVAD might be a valuable option, but it requires invasiveness on the LV and may be challenging to manage, especially in the early phase of the illness. Conversely, when minimal residual LV function is preserved, the blood flow drained by the venous cannula (V) can be divided into two components, supporting respectively the RV and the systemic circulation. This newly proposed configuration may be referred to as V-PaA ECMO. In this case series, we analyse the physiological implication and the management consideration of three different ECMO configurations: Vpv-A ECMO, V-Pa\LVxA ECMO (ex-BiVAD) and our newly proposed configuration for biventricular support, V-PaA ECMO. This case series underscores how tailoring PC-ECMO configuration to ventricular physiology can critically influence clinical outcomes, highlighting the need for individualized support strategies after MVR.
The mortality of patients with mechanical complications following myocardial infarction is high. Surgical repair is challenging due to the fragility of ischemic myocardial tissue. The course is frequently complicated by cardiogenic shock, acute kidney injury and respiratory failure.
We present a patient with out-of-hospital cardiac arrest due to myocardial infarction and left ventricular free-wall rupture, who received extracorporeal cardiopulmonary resuscitation (ECPR), early surgical repair and prolonged veno-arterial extracorporeal membrane oxygenation (VA ECMO) support. The physical outcome of the patient was good with satisfactory exercise tolerance (NYHA II) and there were no neurological deficits following ECPR.
In select cases, VA ECMO can be an option to stabilize patients before and after surgical repair to allow for myocardial scarring and hemodynamic recovery. Advanced hemodynamic monitoring should be considered during the run and weaning from ECMO.
Cases of free-wall rupture and cardiogenic shock are challenging and multidisciplinary teamwork of cardiac surgeons, cardiologists, intensivists and nurses is indispensable.
Extracorporeal Cardiopulmonary Resuscitation (ECPR) is a lifesaving intervention for in-hospital (IHCA) and out-of-hospital cardiac arrest (OHCA). However, severe aortic regurgitation (AR) has traditionally been considered an absolute contraindication for veno-arterial extracorporeal membrane oxygenation (V-A ECMO).
A 63-year-old man with aortic regurgitation experienced IHCA with 50 min of low-flow time. The patient received ECPR and emergent valve-in-valve (ViV) transcatheter aortic valve implantation (TAVI) through a rapid multidisciplinary approach. Despite transient focal neurological symptoms in the early post-resuscitation period, the patient steadily recovered and was discharged with a favourable Cerebral Performance Category (CPC) of 2.
This case challenges the absolute contraindication of severe aortic regurgitation for veno-arterial extracorporeal membrane oxygenation (V-A ECMO) and ECPR candidacy, demonstrating that a multidisciplinary approach with planned venting strategies and rapid definitive intervention can lead to satisfactory patient outcomes.
Severe aortic regurgitation may not absolutely preclude candidacy for peripheral V-A ECMO. A pre-emptive approach integrating detailed venting strategies with emergent transcatheter interventions expands the salvageable population with valvular heart disease.
A 58-year-old male wearing a wearable cardioverter defibrillator due to severe dilated cardiomyopathy with multi-vessel coronary disease presented a cardiac arrest (CA) with ventricular fibrillation refractory to conventional cardiopulmonary resuscitation (CPR). The decision was made to expand CPR to extracorporeal cardiopulmonary resuscitation (ECPR) using extracorporeal life support in the prehospital setting. ROSC was obtained after pump activation, and the patient was admitted to the intensive care unit, sedated and mechanically ventilated while under ECPR support. Despite an initial hemorrhagic shock due to mispositioning of the initial arterial canula requiring surgical repair, neurological evaluation was favorable and allowed for emergency heart transplantation candidacy. The patient was transplanted on day 7 after CA and discharged neurologically intact for rehabilitation on day 60. This case report shows how ECPR can be a bridge to definitive treatment if adequately integrated into an optimized out-of-hospital cardiac arrest chain of survival.
Extracorporeal membrane oxygenation (ECMO) provides lifesaving support for severe respiratory and cardiac failure. Hybrid modes such as venoarteriopulmonary (VAP) may be necessary when conventional modes fail to meet complex physiological demands.
A 31-year-old woman with dermatomyositis-associated interstitial lung disease developed severe respiratory failure. She was initiated on venovenous (VV) ECMO, later complicated by right ventricular injury (RVI) requiring conversion to venopulmonary (VP) ECMO, and ultimately required hybrid VAP ECMO for progressive RVI and cardiogenic shock while awaiting heart-lung transplantation. The unique cannulation configuration provided additional cardiorespiratory support and hemodynamic stabilization, which later enabled safe transfer for transplantation.
Hybrid VAP ECMO may provide effective rescue support for patients with refractory RVI and respiratory failure despite VP ECMO, preserve a surgically naïve chest, avoid differential oxygenation, and serve as a bridge to combined heart-lung transplant.
Hybrid VAP ECMO represents an effective salvage strategy and bridge-to-transplant in complex cardiopulmonary failure.
Venous cannulation can be challenging in newborns, especially those under 3 kg or presenting with vascular malformations. Left subclavian vein cannulation is an alternative site described in adults and infants. We report the first neonatal case of left subclavian cannulation as a last-resort venous access in a newborn presenting with a right-sided congenital diaphragmatic hernia associated with right internal jugular vein malformation. The patient required extracorporeal membrane oxygenation (ECMO) support in the context of refractory septic shock at day 6 of life. ECMO was weaned after 16 days, and cannula was removed without bleeding complications. This alternative venous access may be a viable option for venous cannulation in cases where the right jugular vein is unavailable.
Persistent asystole following restoration of mechanical circulation during extracorporeal cardiopulmonary resuscitation (E-CPR) is typically considered fatal. However, in profound hypothermia, electrical silence may not reflect irreversible myocardial injury.
A term neonate with severe meconium aspiration syndrome (MAS) was initially supported on veno-arterial ECMO at a regional hospital and transported to a tertiary ECMO facility. Following decannulation, she suffered cardiac arrest. Mechanical circulation was achieved after prolonged E-CPR with central cannulation, but the patient remained asystolic in the context of profound hypothermia (31.2°C). Electrical activity reappeared only after controlled rewarming to 33°C. She was discharged home on day 35 with a good long term neurological outcome.
Neonates are particularly prone to rapid hypothermia during resuscitation. Controlled rewarming is essential to determine cardiac viability before establishing futility.
Under profound hypothermia, asystole after restoration of mechanical circulation does not preclude irreversible myocardial damage. Cautious rewarming is mandatory to assess myocardial prognosis.
The combined use of extracorporeal cardio-pulmonary resuscitation (ECPR) and large bore mechanical thrombectomy represents an emerging strategy for patients experiencing cardiac arrest secondary to catastrophic pulmonary embolism.
This retrospective, single-center study included patients treated between January 2023 and June 2025 who experienced cardiac arrest due to catastrophic pulmonary embolism and underwent ECPR followed by large bore mechanical thrombectomy. Primary outcomes were 90-days post-discharge survival and cerebral performance category (CPC) at discharge. Secondary outcomes included support duration, complications during support, and ICU and hospital length of stay.
Fifteen patients were included. Four (27%) sustained out-of-hospital cardiac arrest, and twelve (80%) presented with pulseless electrical activity. All patients underwent large bore mechanical thrombectomy using the Inari FlowTriever System (Inari Medical, Irvine, CA) within 6 hours of arrest in the cardiac catheterization laboratory. Eight patients (53%) survived to discharge with favorable neurological outcomes (CPC 1–2). Seven patients died following withdrawal of care due to cerebrovascular accident or anoxic brain injury (
ECPR followed by large bore mechanical thrombectomy is a feasible resuscitative strategy for patients presenting with catastrophic pulmonary embolism. Larger, multicenter studies are warranted to better define outcomes and the overall impact of this combined approach.
Paradoxical coronary embolism (PCE) is an uncommon cause of acute myocardial infarction (AMI), typically occurring when venous thromboemboli cross a right-to-left shunt in the setting of elevated right-sided pressures. We report a case of mixed obstructive and cardiogenic shock caused by simultaneous pulmonary embolism (PE) and PCE. A previously healthy 43-year-old woman developed profound hypoxemia and inferior ST-segment elevation 3 days after knee surgery. Coronary angiography revealed distal right coronary artery occlusion, successfully treated with aspiration thrombectomy and percutaneous coronary intervention. Persistent hypoxemia, right ventricular injury, and hemodynamic collapse prompted initiation of venoarterial extracorporeal membrane oxygenation (VA ECMO). Subsequent imaging identified extensive bilateral PE and a patent foramen ovale with significant right-to-left shunting. Catheter-based pulmonary embolectomy improved cardiopulmonary function, followed by percutaneous PFO closure. She recovered fully and was discharged home neurologically intact. This case highlights the importance of early recognition, appropriate ECMO configuration, and comprehensive management of PCE with concurrent PE.
Sugammadex (Bridion®, MSD, Seoul, Republic of Korea) is widely used for neuromuscular blockade reversal at the end of general anesthesia. We report a rare case of refractory cardiac arrest secondary to sugammadex-induced anaphylaxis, successfully managed with extracorporeal cardiopulmonary resuscitation.
A 44-year-old man with no history of cardiovascular disease underwent robotic-assisted partial nephrectomy for a renal mass; 3 min after sugammadex intravenous administration, the patient developed ventricular fibrillation. Advanced cardiac life support was initiated, and the extracorporeal membrane oxygenation (ECMO) team was activated. Venoarterial ECMO was initiated 37 min after cardiac arrest onset. The patient was successfully weaned off the ECMO the following day. During admission, intradermal and ergonovine provocation tests confirmed a hypersensitivity reaction to sugammadex and coronary artery spasm, respectively. The patient was discharged on postoperative day 71, without any neurological sequelae.
This successful extracorporeal cardiopulmonary resuscitation (ECPR) in refractory perioperative cardiac arrest due to sugammadex-induced anaphylaxis, highlights that early ECMO team activation and rapid ECPR implementation may lead to favorable neurological recovery.
One potential indication for ECPR is drug poisoning complicated by shock and severe cardiac failure. Over the past 3 years, only one case of in-hospital cardiac arrest due to poisoning was managed with ECPR at our center.
The patient was a 12-year-old girl with a body weight of 60 kg. She attempted suicide by ingesting molsidomine and cinnarizine tablets. Shortly after admission, she developed cardiac arrest, and ECPR was indicated. After 67 min of CPR, ECMO support was established. A pigtail catheter was subsequently inserted for left ventricular unloading. During treatment, the patient was converted to V-V ECMO due to the development of Harlequin syndrome. Finally, she was discharged from the hospital with a good neurological outcome.
Recent advances in ECPR highlight its potential role in the management of drug-induced cardiac arrest. Centers providing ECPR must be prepared for subsequent ECMO management, including the need for conversion to alternative ECMO configurations.
The use of ECPR, particularly in cases of cardiac arrest caused by drug overdose, is justified and effective, as ECMO provides time for drug metabolism and subsequent organ recovery.
Refractory cardiac arrest carries a poor prognosis. Extracorporeal cardiopulmonary resuscitation (ECPR) can be lifesaving but is associated with high morbidity and mortality. We report a likely underdiagnosed complication — non-occlusive mesenteric ischemia (NOMI) — following ECPR, emphasizing the diagnostic challenges and the role of early endoscopic evaluation and an interdisciplinary assessment of these patients.
A 48-year-old man presented with ST-elevation myocardial infarction and developed refractory cardiac arrest due to ventricular fibrillation. ECPR was initiated, and extracorporeal membrane oxygenation (ECMO) flow was achieved after 77 min of cardiopulmonary resuscitation. Early after arrest, the patient passed bloody stool, raising suspicion of mesenteric ischemia. Computed tomography was inconclusive, but colonoscopy revealed ischemic bowel injury. Given the fatal potential of untreated NOMI, prompt colectomy was performed. The patient stabilized postoperatively, recovered progressively, and was discharged from the intensive care unit in good condition after 14 days.
NOMI should be considered in ECPR patients presenting with gastrointestinal bleeding, even when cross-sectional imaging findings are inconclusive. Early colonoscopy enables timely diagnosis and surgical intervention, potentially improving survival in this high-risk setting.
