
Abstract
Background
Excessive gestational weight gain (EGWG) places women at increased risk for complications during pregnancy and also increases the likelihood that they will remain overweight after pregnancy. The Institute of Medicine (IOM) has recommended weight gain guidelines based on pre-pregnancy body mass index (BMI), but evidence-based strategies to achieve these goals are limited.
Objective
This review discusses factors associated with EGWG with the goal of identifying targets for future intervention.
Methods
A search was performed using the PubMed database to identify all English-language papers published between 1995 and 2014 related to excessive weight gain in pregnancy. Papers were grouped by theme: preconception BMI, sociodemographics, diet and exercise, psychosocial characteristics, and type of prenatal care.
Results
Studies found that women who were overweight or obese at the time of conception were at higher risk of EGWG and that increased physical activity protected against EGWG. Studies on diet and sociodemographic characteristics were inconclusive. Psychological factors, specifically accurate perceptions of BMI, also appear to play a role in EGWG. Limited studies on methods of prenatal care delivery did not show improvement of weight parameters with group compared to one-on-one visits.
Conclusion
Pre-pregnancy BMI is most strongly associated with EGWG, indicating that healthy weight habits throughout adult life may be especially important in periods of expected weight change, such as pregnancy. To decrease EGWG, providers should focus on improving pre-conception BMI through appropriate counseling on healthy eating and increased physical activity as well as encouraging pregnant women to continue moderate exercise during pregnancy when appropriate.
Introduction
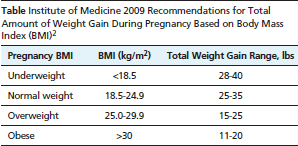
Historically, women struggled to obtain sufficient nutrition to support healthy weight gain during pregnancy. Today, two-thirds of American women are overweight or obese, 1 and up to 50% of American women gain weight in excess of current recommendations. 2 Excess weight can complicate pregnancy and is often retained after pregnancy; thus, gestational weight gain is an important concern. The Institute of Medicine (IOM) published guidelines in 2009 with recommendations for gestational weight gain based on a woman's pre-pregnancy body mass index (BMI) (Table). 2 The guidelines for singleton gestations are referenced to 4 BMI categories: underweight (<18.5), normal weight (18.5–24.9), overweight (25–29.9), and obese (≥30). A weight gain beyond the recommended amounts is termed excessive. Analyses of the 2010 US Pregnancy Risk Assessment Monitoring System (PRAMS) data revealed that rates of excessive gestational weight gain (EGWG) were 20.3% for underweight, 37.2% for normal weight, 64% for overweight and 58.7% for obese women. 3 EGWG has been associated with gestational diabetes, hypertensive disorders, prematurity, increased risk of cesarean delivery, large-for-gestational-age infants, increased postpartum weight retention, and long-term obesity.3,4
Institute of Medicine 2009 Recommendations for Total Amount of Weight Gain During Pregnancy Based on Body Mass Index (BMI) 2
To reduce these potential complications, the American Congress of Obstetricians and Gynecologists, the Royal College of Obstetricians and Gynaecologists, and Royal Australian and New Zealand College of Obstetricians and Gynaecologists have guidelines recommending that providers counsel patients on both obesity-related complications and strategies for avoiding EGWG.5,6 However, a 2014 US national survey demonstrated that pregnant women were less likely than non-pregnant women to receive counseling on weight management. 7 A toolkit for implementation of the IOM pregnancy weight gain guidelines with materials for providers and patients was developed, and its widespread utilization was encouraged by the 2013 IOM dissemination workshop. The toolkit encourages care providers to counsel patients on diet and exercise in pregnancy and to make referrals to nutritionists as needed but does not discuss risk factors associated with EGWG nor provide methods for effective counseling. Thus, the aim of this review is to describe the factors that influence gestational weight gain that can be addressed by providers during prenatal care in an effort to curb EGWG and the associated maternal and fetal sequelae.
Methods
PubMed was searched for articles in English between 1995 and 2014 to identify relevant articles. Search terms included “maternal weight gain”, “gestational weight gain”, “obesity in pregnancy”, “excessive gestational weight gain”, “pregnancy”, “weight”, “race”, “centering”, “group prenatal”, “diet”, “exercise”, “psychosocial”, and “demographics.” The reference lists from the identified articles were also reviewed to obtain additional sources. This search method revealed a total of 36 relevant articles, which were then grouped into 5 themes: BMI at conception, diet and exercise, sociodemographics, psychosocial, and type of prenatal care (Figure).
Bmi at Conception
A woman's BMI at the time of conception was the strongest predictor of EGWG. An analysis of 4619 postpartum women in Arkansas, United States, examined the associations between EGWG and age, race, parity, education, receipt of nutrition assistance or subsidized medical care from the government, and prenatal care. Pre-pregnancy BMI was the strongest predictor of gestational weight gain, and women who were overweight or obese prior to pregnancy were significantly more likely to exceed weight guidelines. The odds ratio (OR) for EGWG in overweight women was 3.21 (95% CI: 2.64–3.91), and for obese women the OR was 4.37 (95% CI: 3.5–5.46). 8

Graph depicts the number and percentage of articles cited in each of 5 categories of the total 36 articles.
Findings from an Australian prospective multicenter cohort study of 1950 nulliparous women corroborated the association of early pregnancy BMI with EGWG. These investigators found that overweight women were 3 times as likely to exceed recommended weight gain parameters (95% CI: 2.2–3.82), while obese women were 2.5 times as likely (95% CI: 1.79–3.52). Interestingly, obese women in this study had an absolute weight gain that was 2 kg less than women in other BMI categories, but because of stricter weight gain recommendations, they were still more likely to exceed the recommended gestational weight gain. 9
Similar associations were reported in 4 additional studies that examined the relationship between pre-pregnancy BMI and EGWG, with rates of excessive gestational weight gain in overweight and obese women ranging from 44% to 69%.10–13 The health consequences are significant, as baseline overweight combined with EGWG leads to an increased risk of fetal complications related to delivery and macrosomia and a higher long-term likelihood of remaining overweight or obese. 14
Sociodemographic Factors
While more than one-third of adult women in the United States are obese, rates differ by race. Obesity rates are 50% for black women, 40% for Hispanic women, 30% for white women, and 10% for Asian women. 15 Yet despite higher rates of obesity among black and Hispanic women, studies indicate lower rates of EGWG. The PRAMS study found lower odds of EGWG among black women, multiparous, and Hispanic women. 8 Another retrospective study of 2760 women from urban community clinics in Minneapolis, Minnesota, United States, from 2004 to 2008 found that among normal weight and obese women, black women gained less weight than white women in the first and second trimesters. Overweight black women gained significantly less than white women in all trimesters. In this study, in the majority of normal weight, overweight, and obese black and white women, 49% to 80% of them exceeded the IOM guidelines for weight gain in the third trimester, with highest EGWG among white women. 16 A retrospective study of 133,000 women in South Carolina, United States, in 2014, similarly demonstrated the highest risk of EGWG among white women. 17 Understanding the differences in pre-pregnancy obesity rates and maternal weight gain during pregnancy associated with race or socioeconomic status can be used to develop more effective ways of directing counseling for women during the prenatal period.
Socioeconomic status, independent of race/ethnicity, may also affect maternal weight gain during pregnancy. Women of low socioeconomic status (SES) are more likely to be obese than those of higher SES. The obesity prevalence is 29% for those at or above 350% of the poverty line compared to 42% for those less than 130% of the poverty line. 18 Yet rates of EGWG were lower among women who had government subsidized health insurance (Medicaid) at any point in the pregnancy, 8 indicating a complex relationship. Huyn et al examined a sample of 56,911 births in New York City from 1999 to 2001 to assess the impact of maternal education, race/ethnicity, and neighborhood SES on EGWG defined as >40 lbs. They found that the association between maternal education and EGWG was affected by both SES and race/ethnicity. Having a college degree and beyond was protective against EGWG for non-Hispanic white women (prevalence ratio [PR]=0.81; 95% CI: 0.67–0.96), but was associated with EGWG for Hispanic women (PR=1.25; 95% CI: 1.12–1.44). Having a college degree or beyond was also associated with increased risk for EGWG for women in low and medium SES neighborhoods (PR=1.26, 95%CI: 1.04–1.53); however, there was no significant association for women in high SES neighborhoods. 19 Mendez et al evaluated neighborhood socioeconomic disadvantage and gestational weight gain in Pittsburgh, Pennsylvania, United States. Of the 55,000 women in the study, 55% gained in excess of guidelines. They found that women who had higher socioeconomic disadvantage scores were more likely to be black and have pre-pregnancy BMI either underweight or obese but were less likely to gain in excess during pregnancy. 20 These studies highlight the complex relationship between SES and other demographic factors when evaluating gestational weight gain.
Psychosocial Factors
Body image, body type, and a woman's perception of self and empowerment also affect weight gain during pregnancy. A prospective, observational study by Hill et al of 108 pregnant women used the Body Attitudes Questionnaire to assess feeling fat, strength and fitness, salience of weight and shape, and attractiveness, and the data were correlated with patient-reported gestational weight gain. Although overall body attitude was not predictive of gestational weight gain, feeling fat in late pregnancy and feeling attractive in mid-pregnancy were related to lower gestational weight gain, and low levels of attractiveness in early and mid-pregnancy were related to higher gestational weight gain. 11 These data suggest that a woman's sense of attractiveness, often influenced by culture and society, can affect gestational weight gain.
A woman's ideal body type may also play a role in gestational weight gain. Mehta et al surveyed 1192 pregnant women using the Body Image Assessment for Obesity tool to compare current body image against ideal body image around 15 weeks’ gestation. Those with a high level of discrepancy (wanting to be lighter) had a decreasing risk ratio for EGWG as pre-gravid BMI increased: RR=0.80 (95% CI: 0.71–0.90) for BMI 36 and RR=0.65 (95% CI: 0.55–0.78) for BMI 42. Women with a pre-pregnancy BMI <26 actually had an increased risk for EGWG: RR=1.20 (95% CI: 1.11–1.30) for BMI 24 and 1.54 (95% CI: 1.33–1.76) for BMI 17. Logically, those who desired to be heavier had increasing gestational weight gain with increasing BMI. 21
In contrast, Sui et al found that increasing discrepancy between actual and ideal body size led to a statistically significant higher gestational weight gain. In this study, 442 pregnant women were asked to identify ideal body size using a Stunkard figure-rating scale; 70% underestimated and 4% overestimated their BMI. Those who were younger and obese were less likely to correctly identify their own BMI. Those who could not identify their own BMI (mostly by underestimating) were more likely to have excessive weight gain. 22 Herring et al conducted a prospective study of 1537 prenatal patients who were assessed for EGWG after self-identifying their pre-pregnancy BMI as normal weight or overweight/obese. Normal weight women who inaccurately perceived themselves to be overweight/obese had an adjusted OR (aOR) for EGWG of 2.0 (95% CI: 1.3–3.0), and overweight/obese women who inaccurately perceived themselves to be normal weight had an aOR of 7.6 (95% CI: 3.4–17.0). 23 These findings suggest that inaccurate perception of weight may be a factor in EGWG.
Overall, psychological factors such as one's sense of attractiveness as well as accuracy in assessment of one's weight have been shown to be associated with gestational weight gain. However, the discrepancy between actual weight and ideal weight and how this affects gestational weight gain is less clear with contradicting results among studies. An understanding of these factors may be helpful in the development of useful gestational weight gain counseling tools.
Type of Prenatal Care
There is a growing body of evidence that group prenatal care models such as CenteringPregnancy 24 may be associated with improved perinatal outcomes,25–27 though only 2 studies evaluated the influence of the model on gestational weight gain.28,29 In their retrospective pilot project of 110 women participating in CenteringPregnancy groups, Klima et al reported higher weight gain among Centering women than controls (32.2 lbs vs 28.5 lbs; P<.05). In contrast, Trudnak et al found no difference in EGWG between Centering and control women after controlling for age, education, employment, marital status, parity, and pre-pregnancy BMI. 29
Diet and Exercise during Pregnancy
Diet and exercise are important factors in weight gain during pregnancy just as they are throughout life. Evidence indicates that pregnant women are less active than non-pregnant women and that activity levels decline during pregnancy. 30 Several large observational studies have investigated the relationship between physical activity and EGWG among different populations using a diverse array of methods.9,12,13,31–33 These have consistently demonstrated that (1) limited or reduced physical activity during pregnancy is associated with higher rates of EGWG9,13 and (2) physical activity during pregnancy is associated with lower rates of EGWG.12,13,31–33 The observational studies reviewed have limitations because they group together all BMI categories in their analyses and they lack standardized definitions or measurement for physical activity. Observational studies focusing on the relationship between physical activity and gestational weight gain among obese, overweight, or other higher-risk subsets of women are lacking.
Observational studies have also been conducted to investigate the relationship between diet and EGWG; however, the results from these studies are disparate and somewhat difficult to interpret.12,33,34 Several studies suggest a significant association between total energy intake and greater gestational weight gain, and others have identified specific relationships between greater gestational weight gain and various aspects of daily food intake, such as protein intake, energy density, dairy intake, fried foods, and the number of food servings per day.33,34 Similarly, lower gestational weight gain has been associated with carbohydrate intake amount and a vegetarian diet. 34 Other studies, however, have failed to identify any relationship between diet and gestational weight gain.12,34 Because of the lack of overlap with the measured dietary characteristics between studies and the conflicting results, it is difficult to draw conclusions about the relationship between diet and EGWG.
Studies to determine the effectiveness of specific interventions can help guide providers in appropriately counseling patients. Many such trials have been conducted, and a number of well-designed systematic reviews and meta-analyses have been performed to synthesize their results35,36 A few of these reviews, including the 2012 Cochrane Review, were unable to find a consistent or significant effect of lifestyle interventions on gestational weight gain.35,36 This is largely due to the heterogeneity of interventions and outcomes measures, which interfered with the ability to identify trends or to pool data for larger analysis.35,36 Other systematic reviews and meta-analyses, however, did pool data from trials with widely varying lifestyle interventions and identified a significant positive effect of a broad range of lifestyle modifications on gestational weight gain.37–41 In their 2011 review and meta-analysis of 9 trials (N=906), Streuling et al focused on high-frequency physical activity interventions only (ie, structured aerobic exercise activities at least 3 times per week for at least 20 minutes per session). 39 Although the results of the individual trials were conflicting, the meta-analysis of the pooled data showed a significant reduction in gestational weight gain in the exercise groups compared to controls (P=.03) with a mean difference in weight change of –0.61kg (95% CI: –1.17 to –0.06). 39 They further examined the mean difference in weight change by energy expenditure and found no evidence of a dose effect. 39 In addition, a randomized control trial conducted in Sweden suggested that just providing counseling on gestational weight gain recommendations and then tracking and discussing a patient's weight may reduce EGWG. This trial showed that these low-cost interventions reduced overall weight gain, although not statistically significantly. 42 These results suggest that providers can counsel their patients to reduce gestational weight gain by engaging in moderate aerobic exercise activities at least 3 times per week for at least 20 minutes, unless it is medically contraindicated.
In their 2011 review and meta-analysis of 13 trials (N=1434), Tanentsapf et al attempted to isolate the effect of dietary interventions on gestational weight gain by focusing on trials that included a dietary intervention. 41 All of the trials included dietary intervention, but they varied in terms of intensity, frequency, type of intervention, and use of counseling and/or educational materials. 41 About half of the interventions, however, also included physical activity, meaning that dietary interventions cannot entirely account for the observed effects. 41 The review found that the interventions significantly reduced total gestational weight gain with a weighted mean difference in weight change of –1.92 kg (95%CI: –3.65 to –0.19). 41 They also noted that the 2 studies that showed the strongest effect included a relatively high-intensity dietary intervention using food-intake diaries as a guide to individualized dietary modifications.43,44 They then repeated their analysis excluding those 2 studies, and they again observed a positive effect of lower-intensity dietary modifications on gestational weight gain. 41 Their results suggest that dietary interventions may help to limit GWG regardless of the intensity of the intervention, but higher intensity interventions with close monitoring and individualized dietary guidance may be more effective.
The Wolff et al and Thorton et al studies were among the 4 trials reviewed by Tanentsapf et al that stratified their results based on pre-pregnancy BMI.43–45 Interestingly, the 2 trials of lower-intensity dietary interventions,45,46 such as receiving educational materials or a single counseling session on diet and exercise, were found to be effective only among women with normal BMI. The higher-intensity interventions, however, that included food intake monitoring and individualized dietary modifications, were found to be effective among women in overweight or obese BMI categories.43,44 These results suggest that higher-intensity dietary interventions including intake-monitoring and individualized dietary recommendations may be more effective in women at greater risk of EGWG.
Finally, in their 2013 review and meta-analysis of 7 trials (N=721), Choi et al focused on trials of physical activity interventions among women in overweight or obese BMI categories. 40 The interventions varied in terms of frequency, duration, and structure/supervision of the physical activity, and some of the interventions also included lifestyle modification counseling. 40 The meta-analysis of the pooled data showed a significant reduction in gestational weight gain among overweight and obese women. 40 The strongest effect was seen with supervised physical activity plus dietary intervention (weighted mean difference –1.17 kg [95% CI: –2.14–0.21]). These findings support the concept that reducing gestational weight gain among obese and overweight women may require higher-intensity interventions in diet and physical activity.
Discussion
Obesity among reproductive-age women is an increasing problem worldwide, and providers need tools to protect women against the consequences of excessive weight gain during pregnancy. The 2009 IOM guidelines provide a goal weight gain for pregnant women based on pre-pregnancy BMI, and the 2013 IOM dissemination workshop aims to facilitate efforts to reduce EGWG by providing providers with more resources for educating and counseling patients. This review aimed to identify risk factors for EGWG, discuss interventions with demonstrated efficacy, and determine areas where further investigation is needed to allow providers to tailor their counseling efforts around gestational weight gain. The weight at which a woman enters pregnancy is the most predictive factor for EGWG. Thus optimizing healthy weight habits throughout adulthood is crucial. Weight should be addressed by primary care providers, during preconception counseling, and at non-obstetric visits related to reproductive health.
Socioeconomic status, race, and ethnicity play significant roles in many health outcomes, and low-income minority women have higher rates of obesity than affluent and white women. However, associations between race, ethnicity, or education and EGWG are complex. Despite higher overall rates of obesity, black and Hispanic women had lower rates of EGWG than white women overall. Other socioeconomic factors had complex relationships with race and class, with higher educational attainment being protective for white women while increasing the risk of EGWG for Hispanic women and women from lower socioeconomic classes. Thus further studies are needed to help explore the complex relationships between race, class, geographic location, and EGWG.
Women who remain physically active during their pregnancies have less risk of EGWG. There is clear guidance for providers in this area: the US Department of Health and Human Services Physical Activity Guidelines recommend that healthy pregnant women who are not already highly active get at least 150 minutes of moderate intensity aerobic activity per week. 47 Dietary interventions had less conclusive results, and intensive interventions may be needed to prevent EGWG in overweight and obese women.
An understudied and potentially modifiable risk factor is inaccurate weight perception as a risk factor for EGWG. Women who underestimated their level of obesity were significantly more likely to gain excess weight. Obese women were also less likely to receive weight counseling, perhaps due to providers’ reluctance to broach a sensitive topic. However, making women aware of their true BMI in a sensitive manner may be helpful to prevent EGWG. Research on the effectiveness of interventions focused on increasing the accuracy of women's weight self-perception are warranted.
Group pregnancy visits, in spite of their growing popularity and improved perinatal outcomes, are no better and may be worse at limiting EGWG compared to traditional prenatal care. 48 However, the data are currently limited, and this area merits future study.
Limitations
Given the complexity of this topic, we chose to include the most widely studied factors contributing to EGWG but acknowledge that additional factors likely play a role. In addition, most articles reviewed were retrospective surveys based on patient reports, and some did not control for confounding variables. There is a dearth of prospective randomized controlled trials on effective interventions to limit EGWG, limiting our ability to provide strong guidance to providers.
Conclusion
EGWG is a multifactorial problem. While pre-pregnancy BMI and reduced physical activity have the strongest association with EGWG, there is conflicting evidence linking sociodemographics, psychological factors, diet, and type of prenatal care to excessive weight gain. While there are a myriad of factors that likely effect EGWG, until there is more conclusive evidence, the focus should be on the following: preconception counseling to encourage a healthy BMI prior to pregnancy, emphasizing healthy eating and continued physical activity during pregnancy, and—for women with a BMI greater than 25—-provision of specific counseling regarding immediate and long-term sequelae of EGWG and referrals to resources such as nutritional counseling when needed to help them achieve their weight gain goals.