
Abstract
The association between gastro-esophageal reflux disease (GERD) and asthma, although well established in adults, is less strong in the pediatric age group. Benefits of proton pump therapy are limited across age ranges. While there is a growing body of literature on the use of complementary treatments for both asthma and GERD, few studies have focused on treatment benefits for the GERD-asthma association. We present the case of a 2-year-old boy with asthma and GERD who was not responding to inhaled, low-dose corticosteroids, beta-mimetic therapy, and a 6-week course of proton pump inhibitor treatment. We noted a gradual disappearance of symptoms when he was given an oral preparation of Pulvis stomachicus cum Belladonna, an anthroposophic medication containing Matricaria recutita, Atropa belladonna, bismuth, and antimonite. Matricaria recutita and bismuth have known gastric protective properties, and Atropa belladonna contains anticholinergic agents that have a bronchodilatory effect. These complementary medications appear promising in terms of relieving the symptoms of GERD-associated asthma.
Introduction
The association between gastroesophageal reflux disease (GERD) and asthma is well established in adults and a possible link has been reported in children.1,2 Asthma in GERD patients can be caused by liquid and gaseous reflux leading to bronchial constriction and damage. On the other hand, GERD can be exacerbated in patients with cough and wheeze due to an increased pressure gradient across the lower esophageal sphincter.1,2 Despite our improved knowledge, treatment of these patients has been challenging.
A recent meta-analysis concluded that proton pump inhibitor (PPI) treatment of adults with asthma only results in a small clinical improvement in morning peak expiratory flow. 3 A possible explanation is that PPI treatment reduces acid production—which supports esophageal healing—but does not reduce reflux and underlying esophageal dysmotility.4,5 In asthmatic children with GERD, PPIs provide no clear benefit and were ineffective in children with asymptomatic reflux.6,7 In a cohort of children characterized as poor metabolizers of PPI due to a cytochrome P450 polymorphism, asthma worsened under PPI, probably because over-suppression of gastric acid increases susceptibility to respiratory pathogens which in turn affects asthma control. 8
Different complementary treatments exist for the treatment of asthma, but evidence supporting an effect vary widely, 9 as well as for GERD. 10 However, according to our database searches the only studies of complementary medicine for the GERD-asthma association focus on Chinese medicine. 11
Matricaria recutita and bismuth have known gastric protective properties,12,13 and Atropa belladonna contains anticholinergic agents that have bronchodilatory effect. 14 Complementary treatments containing these ingredients could be used to treat patient with GERD and asthma, and if effective, could be an additional treatment tool that could also reduce the use of long-term inhaled corticosteroids and proton pump inhibitor treatment and thus their side effects.
Anthroposophic medicine is an integrative medical system based on a multilevel concept of the human organism. 15 Specific anthroposophic treatments include medications based on plant, mineral and animal substances (often in low homeopathic potencies); art therapies; and specific nursing techniques.15,16 In this case report, we describe the effects of a number of anthroposophic treatments on a young boy with non-atopic asthma and GERD.
Presenting Concerns
A 2-year-old white boy presented to our clinic with frequent coughing episodes since 6 months of age. On presentation, a daily, mostly dry cough had been present for most of the preceding 12 months, exacerbated when running and when lying flat at night. His mother had to put 2 pillows under his head before he could sleep. Occasionally, mild wheeze was noted on auscultation. Daily inhalation with salbutamol and ipratropium bromide brought modest relief. On 2 occasions, cough was accompanied by fever but without tachypnea or crackles. On these 2 occasions, treatment with antibiotics cefaclor and cefuroxime did not stop the cough. On 2 further occasions, cough was accompanied by rhinorrhea. One month of montelukast (a leukotriene receptor antagonist) and later 3 months of twice-daily inhalations with fluticasone (a glucocorticoid) 50 μg brought no improvement to his cough. His mother described that he would often gag during meals and at night would smack and swallow from apparent regurgitation. He continued to develop well, following growth curves along the 50th percentile for height and 75th percentile for weight. The boy began daycare when he was 2 years old.
The child had been born by vaginal delivery after an uneventful, full-term pregnancy and had been breastfed for the first 5 months, supplemented with formula from the age of 6 weeks. Significant regurgitation was noted from a few days of life until cessation at 6 months of age. His mother reported an almost constant dribbling of milk from the angle of his mouth and occasional projectile vomiting after feedings. Thickening of formula was not tried. He became a “colicky” baby with considerable crying between 2 weeks and 5 months of age, but he slept well at night and had no additional feeding difficulties. Psychomotor development was normal. He crawled at 8.5 months, walked at 14.5 months, and began talking by the age of 2 years. He received all routine German vaccinations except the rotavirus vaccination. No family member had asthma or allergies, but his grandmother had suffered from gastroesophageal reflux since childhood.
Clinical Findings and Diagnostic Assessment
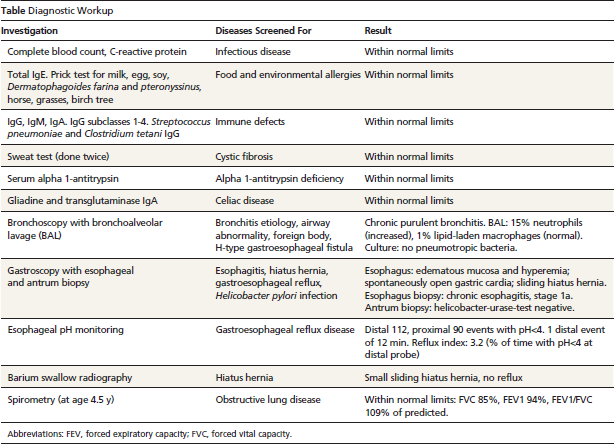
A timeline of events is presented in the Figure, and an overview of results from diagnostic investigations is presented in the Table. Diagnostic investigation for food and environmental allergies, immune defects, cystic fibrosis, alpha-antitrypsin deficiency, bronchial disorders, and GERD were done at a German children's hospital. The child's physical exam was normal at the time; oxygen saturation was 96%. Bronchoscopy revealed purulent bronchitis with increased leukocytes on bronchoalveolar lavage. Gastroscopy highlighted a spontaneously open gastric cardia and sliding hiatal hernia. Esophageal biopsy was consistent with esophagitis type 1a (Institute of Pathology, University of Mainz, Germany). Twenty-four-hour pH monitoring detected 90 reflux episodes (all <5 min) with pH <4 at the proximal pH probe and 112 episodes at distal probe (1 episode of 12 min). The Reflux Index (percentage of time with pH <4 at distal probe; normal = <3%, pathological = >7%) 17 was 3.2%. A diagnosis of GERD with associated asthma was made, and physicians recommended a hemi-fundoplication of the stomach for the sliding hiatal hernia.
Figure Timeline of events.

Therapeutic Focus
Following bronchoscopy and gastroscopy, the boy became febrile and was treated with oral cefaclor for 2 weeks. Clinicians started him on 10 mg twice-daily omeprazole (1.4mg/kg/day) to treat esophagitis. The mother sought a second opinion from another children's hospital, where a barium swallow revealed a small sliding hiatal hernia and no reflux (barium swallow has low sensitivity for reflux). Clinicians there advised her to add fluticasone inhalation to the omeprazole treatment, advice that the mother did not follow because previously fluticasone had no effect.
After 1 month of omeprazole administration and the child continuing to cough, the mother contacted our center (Filderklinik, Filderstadt, Germany) in light of the fact that we practice an integrative pediatric approach combining conventional medicine with anthroposophic medicine.
Three anthroposophic medicines were subsequently added to this child's treatment regimen (10 mg twice-daily omeprazole) in January 2012:
Pulvis stomachicus cum Belladonna (Weleda AG, Schwäbisch Gmünd, Germany), 2 pinches orally 3 times a day, containing Matricaria recutita, Atropa belladonna, bismuth, and antimonite, with all ingredients in the homeopathic strength D3 (in homeopathic nomenclature D3 denotes a 1:1000 dilution of the mother tincture);
Tabacum Rh D6 (Weleda AG, Schwäbisch Gmünd, Germany), 8 drops twice daily; and
Meteoreisen/Phosphor/Quarz (Wala Heilmittel GmbH, Bad Boll, Germany), 8 granules twice daily, containing Ferrum sidereum D11/Phosphor D50/Quarz D11.
The medications described are registered through “Commission C for anthroposophic medicinal products” of the German Federal Institute for Drugs and Medical Devices and are registered without therapeutic indication.
On her own initiative, the mother also began taking her son to artificial salt caves approximately twice a week. During the first 8 weeks of salt-cave visits, he would cough intensively at first before coughing decreased. The mother stopped omeprazole, Tabacum, and Meteoreisen/Phosphor/Quarz after 6 weeks because she felt that it had no effect. However, she continued treatment with Pulvis stomachicus cum Belladonna for 1 year. During 1 coughing episode, the boy inhaled Cuprum aceticum D4 (Weleda AG, Schwäbisch Gmünd, Germany), which the mother reports had some beneficial effect.
Follow-Up and Outcomes
During the following weeks and months after starting the anthroposophic medication and salt-cave visits, a gradual improvement in symptoms was noted by the mother. Gagging during meals stopped, as did the smacking and swallowing at night. Coughing episodes became shorter and considerably less frequent.
About 10 months into the anthroposophic treatment, coughing only occurred with exertion and then ceased entirely between March 2013 and December 2013. In the 2013–2014 winter period, the child had two 2-week coughing episodes when he had an upper respiratory tract infection. During these episodes, the mother again noted smacking at night (she felt reflux was triggered by coughing, not the other way around), and salbutamol and Pulvis stomachicus cum Belladonna brought relief. Due to the child's age, a lung function test first became possible in May 2014 when he was aged 4.5 years. This, therefore, took place when symptoms had already resolved and results were normal (forced expiratory volume in one second [FEV1] 94%, forced vital capacity [FVC] 85%, and FEV1/FVC 109% of predicted). 18
Diagnostic Workup
Abbreviations: FEV, forced expiratory capacity; FVC, forced vital capacity.
Mother's Perspective
I felt that his bronchitis and reflux healed due to Pulvis stomachicus and the salt-cave visits. It did not happen overnight but it was a gradual improvement over weeks and months. Whenever he has a shorter cough episode now, he again has this smacking at night. I then give salbutamol and Pulvis stomachicus and it helps.
Discussion
This boy's respiratory symptoms on presentation were consistent with non-atopic asthma. A diagnosis of GERD was appropriate, based on biopsy-confirmed esophagitis, high-frequency acid events during pH monitoring, and correlating symptoms of smacking and swallowing at night, dysphagia, and significant regurgitation during the first months of life. 17 The small sliding hiatal hernia certainly contributed to the development of GERD as a hiatal hernia compromises all anti-reflux barriers at the lower esophageal sphincter.1,2 Fundoplication was prematurely recommended to this patient prior to conventional GERD treatment being tried.
Treatment with Pulvis stomachicus cum Belladonna and visits to salt caves were the consistent elements associated with gradual clinical improvement. Spontaneous improvement with increasing age seems less likely considering the long duration of symptoms and compared with the relatively short time frame to a notable clinical improvement. Both long-term and short-term improvement were noted when the patient was taking Pulvis stomachicus cum Belladonna because the mother also observed cessation of smacking at night and cough when she used Pulvis stomachicus and salbutamol during the few recurring cough/regurgitation episodes.
Omeprazole brought no improvement of cough over 6 weeks and was then stopped prematurely by the mother. In studies, treatment refractory reflux has been defined as lack of symptom relief after 8 weeks of PPI, 19 and an initial 3-month PPI treatment is recommended for endoscopically diagnosed reflux esophagitis. 17 Healing of esophagitis might already have occurred after 6 weeks, but in any case did not stop the cough, possibly because liquid or gas reflux continued.
A potential effect of Pulvis stomachicus cum Belladonna, considered to improve reflux, mucosal erosions, and upper gastrointestinal motility problems, 20 is not implausible. Matricaria recutita (German chamomile) contains flavonoids, in particular apigenin, which has well documented antiinflammatory, antispasmodic, and gastric protective effect in animal studies. 12 Clinical studies indicate a possible effect on infants with colic and diarrhea. 21 Chamomile is also present in the combination STW5 (iberogast), which in trials has proven effective for functional dyspepsia. 22
Atropa belladonna contains agents with anticholinergic properties, such as atropine, scopolamine, and hyoscyamine. Anticholinergics have bronchodilatory effects, and Atropa belladonna has grade C evidence (GRADE rating for evidence) for airway obstruction.14,23 On the other hand, anticholinergics also relax the esophagus sphincter, so would not be expected to improve reflux at conventional dosage. Here the alkaloid content at the homeopathic dilution D3 was only 0.0001%, suggesting only a mild relaxing effect. 24 Using a different plant with bronchodilatory properties might be more logical for this combination.
Bismuth, apart from its actions on Helicobacter pylori, protects gastric tissue from excessive injury because it is cytoprotective, has ulcer healing effects on the mucosa and inhibits gastric acid secretion. 13
Antimonite and its substrates are known to have immune activating properties 25 ; however, its role in relieving symptoms of asthma and GERD is unclear.
Lastly, the natural salt-cave climate has been used for the treatment of respiratory conditions, particularly in Eastern Europe, with artificial caves now in operation (known as halotherapy). 26 Improved respiratory function among patients with asthma and chronic obstructive pulmonary disease has been noted in 3 case-control studies. 27
The time sequence of this case—continuous, treatment-refractory symptoms for 1 year, thorough work-up, then improvement on complementary treatment—was helpful for gauging treatment effect. Of interest is that both long-term improvement and, during cough recurrence, short-term improvements were noted. A disadvantage was that conventional treatment had not been maximized because the mother shortened PPI treatment and did not restart inhaled corticosteroids as recommended. This report relied on symptom reporting by the mother, who had kept a detailed symptom and treatment diary. There was no repeat pH monitoring because this is not needed in cases where a patient has a good clinical response. 17
In this boy, an oral preparation of Pulvis stomachicus cum Belladonna containing Matricaria recutita, Atropa belladonna, bismuth, and antimonite, as well as halotherapy, seemed to have led to improvement of GERD and associated non-atopic asthma. A short, preceding course of omeprazole may also have played a contributing role. We encourage others to publish their experience with this medication.
Informed Consent
The patient's mother read the final manuscript and gave written informed consent to publish these data. All patient information has been de-identified.
Author Contributions
RM was the treating pediatrician and critically reviewed the manuscript. TvSA conceptualized the report, wrote the manuscript, and prepared the figures. HK, GSK, and JV critically reviewed the manuscript.