
Abstract
Fragmented and non-interoperable information systems (ISs) generate poor quality information and adversely affect the provision of healthcare services and the management of the Slovenian healthcare system. Advanced implementation of the eHealth project, encompassing the construction of a national health information system (HIS), could play a pivotal role in overcoming these challenges, which significantly compromise further development of the Slovenian healthcare system. This paper initially presents a review of the recent developments concerning HIS and identifies its main operative deficiencies. Subsequently, the paper outlines the construction of a 3LGM2-based conceptual HIS model and provides generally applicable recommendations and guidelines for effective implementation of HISs. This research employs a single explanatory/exploratory case study design, while the validation of the hypothesized constructs was undertaken through structured interviews with 15 prominent experts from the Slovenian healthcare system. The findings provide valuable insight into the operative, construction, and implementation aspects of HIS, which can, subject to proficient coordination with other ecosystem factors and pending structural reforms, ensure better utilization of public healthcare resources and provide tangible public health benefits.
1. Introduction
The Slovenian healthcare system has been facing serious structural problems in recent years. Due to objective circumstances [1, 2] these problems cannot be avoided, and will require fundamental changes in the current healthcare arrangements. Healthcare system reform is becoming a social imperative that calls for a comprehensive and innovative approach in the coming years. One of the essential instruments that would allow the challenges facing the Slovenian healthcare system to be effectively tackled is comprehensive informatization [3–5], representing one of the key long-term goals of the public sector. The experience of developed countries shows that effective implementation of the informatization projects and construction of the national health information system (HIS) is of immense strategic importance for the further development of the healthcare system [6–8], but also has important implications for an increase in social welfare [9, 10], economic growth [11, 12], and the development of the information society [13–15].
Wilson [16] defined HIS as a set of tools and procedures that a health programme uses to collect, process, and transmit health data in order to facilitate monitoring, evaluation, and control in the healthcare system. Lippeveld and Sapirie [17] applied a broader definition as they outlined HIS as a mechanism with the ability to integrate data collection, processing, reporting, and use of the information necessary to improve healthcare service effectiveness and efficiency through better management at all levels of the healthcare system. HIS plays an important role in ensuring that reliable and timely health information is available for operational and strategic decision-making, thus providing better healthcare services and enhancing public health [18, 19]. Regardless of their definition and research perspective, virtually all authors emphasize that the main goal of HIS should be to contribute to high-quality, efficient patient care and the effective performance of the healthcare system [20–23, etc.].
Despite their importance, HISs in many developing countries are weak, fragmented, and often focused exclusively on disease-specific programme areas [24, 25]. Notwithstanding the potential of HISs, in practice, the collection, compilation, analysis, and reporting of health data are riddled with major problems [5, 26, 27]. Furthermore, the data received are often not helpful for healthcare management decision-making because they are incomplete, untimely, and unrelated to the priority tasks of healthcare professionals [28–30].
The quality performance of HISs is thus linked not only to technical determinants such as data quality, system design, or adequate use of information technology (IT) [23]. Other determinants are also involved, such as: 1) organizational and environmental determinants that relate to the information culture within the country context [31, 32], the structure of HIS [33, 34], the roles and responsibilities of the different actors and the resources available for HIS [30, 35]; and 2) the behavioural determinants such as knowledge and skills, attitudes, values, and motivations of those involved in the production, collection, collation, analysis, and dissemination of information [36]. For successful implementation and exploitation of HIS, certain prerequisites need to be in place [37]:
Information policies – referring to the existing legislative and regulatory framework for public and private providers, use of standards;
Financial resources – investment in the processes for the production of health information (e.g., the collection of data, collation, analysis, dissemination, and use);
Human resources – adequately trained personnel at different levels of the healthcare system;
Communication infrastructure – infrastructure and policies for the transfer and management or storage of information;
Coordination and leadership – mechanisms to effectively lead HIS.
Transformations in the way healthcare is delivered are creating new opportunities for innovative applications of IT [38, 39]. Healthcare systems are currently undergoing many changes, including the integration of modern IT solutions that are breaking down the organizational barriers that have stood between stakeholders in the healthcare system. Newly emerging healthcare delivery patterns and business models [40, 41] are supported by, and in some cases reliant on, the widespread use of IT and integrated HISs.
Although the basic informatization of the healthcare system was established relatively early, Slovenia still does not have an interoperable and comprehensive HIS. The majority of such systems have been developed within individual healthcare organizations and are designed specifically to meet their own needs, while they are not adequately interoperable and do not provide reliable, relevant, and timely information [30, 42]. The already initiated national project of healthcare system informatization from 2005, named eHealth, is supposed to result in a wide-ranging HIS, which should be able to integrate all fragmented information systems (ISs) into a functional mechanism and offer a complete solution benefitting all interested parties [3, 43].
The aim of this paper is to provide a review of recent developments and concerns facing the recent introduction of the HIS, hypothesize the construction of the HIS, and propose an appropriate course of action ensuring the successful implementation of the Slovenian HIS in upcoming years. Construction of the HIS presented in this paper is partly based on the three-level graph-based model (3LGM) and mainly on its later version, i.e., a three-layer graph-based meta-model (3LGM2) approach. This comprehensive modelling approach was introduced by Winter and Haux in 1995 in order to support the systematic construction of HISs and facilitate high-level strategic information management in hospitals [44]. Accordingly, this paper primarily focuses on the following interrelated research objectives:
a review of the recent development activities in the HIS field and identification of its main operative deficiencies;
construction of the 3LGM2-based conceptual HIS model, corresponding to the growing information needs of the Slovenian healthcare system;
provision of generally applicable recommendations and guidelines for the cost- and time-effective implementation of HISs.
2. Methods
2.1 Research Design
This study employs a single explanatory/exploratory case study design. The case study on the 3LGM2-based conceptualization of HIS and the provision of general recommendations and guidelines for its implementation was conducted in the second half of 2013. The selection of the research method was adapted to the particularities of the research problem [45, 46], given that quantitative empirical research could not yield a satisfactory and credible picture, since this complex field of research is still in an early stage of development and it would be difficult to ensure the representativeness of the research sample. Iterative, structured interview processes complemented by a literature review and observations were used as the main data collection techniques during the formative research phase.
2.2 Sample
The selection of the potential interviewees was based primarily on their experience and expertise in the construction of HISs. Good knowledge of the informational, structural, and contextual characteristics of the healthcare system by the selected interviewees ensures the credibility and validity of their views and recommendations. The final sample size comprised 15 (n=15) prominent experts from a cross section of areas strongly related to the concept of HIS.
All 15 interviewees came from different healthcare-related institutions. Five experts were chosen from each key area: healthcare professionals (two specialists from public hospitals and three general practitioners from public healthcare centres), IT experts from healthcare and government institutions (two analysts from government institutions and three IT consultants from public clinics and a public hospital), and healthcare managers (two managers of a public healthcare centre and a public hospital and three managers of public clinics). The interviewees occupied senior positions at different levels of the healthcare system (information, medical, and financial directors of healthcare centres/clinics, heads of government sectors and departments, etc.). The age and gender of the interviewees reflect the situation in Slovenian healthcare system management practice. The participants were aged between 43–61 years, and the ratio between men and women was 4:1.
2.3 Data Collection
Before commencement of the interview process, three pilot interviews were carried out, including with one expert from each of the designated areas. The final set of questions was revised in line with their comments and suggestions, which helped to resolve some conceptual weaknesses and ambiguities. The response rate was 100%, as all invited experts responded to the invitation and participated in the interviews. The interviews were carried out in the period from October to December 2013. Since new information and knowledge on the subject appeared after certain interviews, interviewees went through an iterative interview process consisting of several interview meetings. The interviews, which lasted approximately 90 to 120 minutes, were conducted by the author in person at the official premises of the interviewees. All participants were told the purpose and objectives of the study. Interviewees gave informed consent and were provided anonymity, and assured the confidentiality of the information obtained.
The interview comprised eight open-ended questions, which were based on a review of the existing literature (journal articles, papers, strategy documents, project reports, online resources, etc.) and related to the study objectives. The questions were broadly focused on exploring the different dimensions of the Slovenian healthcare system, the concept and potentials of the HIS in the healthcare environment, the operative and construction aspects of the HIS, characteristics and applications of the 3LGM2, and specification of the necessary preconditions and measures for the effective implementation of the HIS in the upcoming years. Unresolved issues, existing limitations, potentials, and future directions were further analytically discussed with the interviewees in an iterative manner. Namely, the role of the healthcare experts within the proposed case study was threefold. First, they had to summarize the recent developments concerning the HIS and identify its main operative deficiencies. Second, they had to outline the construction of the 3LGM2-based conceptual HIS model. Third, drawing from their own experience and knowledge of the healthcare system, they had to provide their vision of the further expansion and integration of the HIS, and ultimately propose a set of recommendations and guidelines for minimizing risks and ensuring enhanced implementation of the HIS in the forthcoming years. Given the iterative nature of the overall interview scheme and the active role of the interviewees in the later stages of the research, special content authentication (authorization) of their responses was not required. The responses of the interviewees to the questions were recorded in writing by the interviewer.
2.4 Data Analysis
This research phase included an analysis of two datasets, namely: 1) literature (journal articles, papers, strategy documents, project reports, online resources, etc.), and 2) interview data (contained in the interview transcripts). The data obtained through the theoretical and empirical qualitative research were analysed by the authors in accordance with the guidelines proposed by the case study methodological framework. Multiple analyses of the data obtained (re-analysis after each round of interviews), their interpretation, construction of the 3LGM2-based conceptual HIS model, and the subsequent provision of recommendations and guidelines for the implementation of the HIS were carried out in collaboration with the experts from the healthcare system, who assumed a constructive role throughout all phases of the study. The final structure and contextual characteristics of the conceptual HIS were achieved through the joint efforts, whereas the resolution of inconsistencies and reaching consensus demanded a great deal of patience, and extensive communication and coordination between the author and the participating experts.
After an extensive review of the literature and investigation of primary and secondary online resources, papers, strategies, project reports, and other materials containing HISs-related content, the author systematically analysed the HIS concept, different aspects of the 3LGM2 modelling approach, and the necessary steps for overcoming the existing technical, organizational, policy and other constraints and obstacles. The analysis of the case study evidence served as a platform for the construction of the 3LGM2-based conceptual HIS model and the final provision of recommendations and guidelines for its effective implementation. Based on an analysis of the case study evidence, the author and the expert group had to perform a transformation of the 3LGM2 generic modelling approach (hospital-based) and facilitate its adaptation to the specific healthcare environment in Slovenia (national-based). The transformation and adaptation process was challenging, since the translation of the generic modelling approach procedures, building blocks and their characteristics to the concrete needs of the healthcare system required maintaining their original functionality and inherent role in the newly formed HIS, while facilitating a custom-made solution.
The application of the specific methodological framework and the respective data collection techniques were instrumental for the overall data analysis. The latter provided a basis for the interpretation of data obtained by the review of HIS-related sources, and synthesis of data obtained by the conducted interviews, which ultimately facilitated the 3LGM2-based conceptualization of HIS and the establishment of coherent recommendations and guiding principles for the implementation of the HIS.
3. Results
3.1 HIS in Slovenia
The Ministry of Health has been dealing with the informatization of the Slovenian healthcare system for almost two decades. The eHealth project in its latest form consists of 17 sub-projects aimed at the extensive renewal and integration of local ISs in the healthcare domain. The strategic goals and objectives within the eHealth strategy should be implemented by the year 2023, facilitating a fully integrated national HIS enabling monitoring of on-going treatments and related costs, faster access to medical data, clinical services as well as cost evaluation, online ordering and coordination of waiting lists, an increase in the efficiency and transparency of the healthcare system and optimization of the business processes taking place in healthcare institutions [4, 47]. Building a comprehensive HIS requires the inclusion of a widespread network of stakeholders and the harmonization of many information subsystems at different levels of healthcare [5]. Informatization of the Slovenian healthcare system should provide opportunities for high quality and professional work with patients and long-term development, whereas relevant and credible economic, administrative and clinical data provided by the HIS should facilitate better quality planning, control and management of healthcare organizations and the healthcare system in general [30, 42].
Based on the Strategy for the Informatization of the Slovenian Healthcare System 2005–2010 and the Resolution on the National Healthcare Plan for the Period 2008–2013 [3, 4], all activities in the field are aimed at realizing the eHealth project. A summary of its development goals is presented below:
The establishment of a basic IT infrastructure, including: a network used for communication and data exchange, Diagnosis Related Groups (DRG) and standardized definitions of health and social data required for the development and management of electronic health records (EHR), personal health records (PHR), ePrescriptions, as well as improvement of the healthcare Smart Card functionalities (the Smart Card allows access to medical data containing information on: the cardholder, the person liable for the health insurance contribution, compulsory health insurance, voluntary health insurance, one's chosen personal physician and general practitioner (GP), issued medication, issued prosthetic equipment, potential organ and tissue donation for transplantation, etc. After the construction of a comprehensive HIS, the Smart Card will allow all users to remotely access their own health data). Currently, EHR content is still not defined explicitly, while its structure comprises free text, preventing its full exploitation. Existing diagnoses as well as clinical procedures are standardized and structured according to the ICD 10 AM 1 classification [48]. Whereas EDIFACT 2 [49], HL7 3 [50], and XML 4 [51] are the current data standards for the transfer of messages.
Integration and merging health and social IS into a comprehensive national HIS and establishing a central, unified health information portal that will allow all stakeholders within the healthcare system secure and reliable exchange of data and execution of electronic services, as well as standardized and transparent information and interoperability with similar systems in the EU.
The introduction of eBusiness as a standard way of conducting operations and processes in the Slovenian healthcare system and promoting and encouraging the use of eHealth applications by all healthcare system stakeholders.
The eHealth project is thus divided into three substantially separate yet related areas [3], (Figure 1). The first area is the establishment of a national HIS, comprising a Health Network (hNET), a health portal (hAOP), and EHR. The second area represents the establishment and operation of a Centre for Healthcare Informatics, which will take the central role in managing the HIS. This area also includes upgrading and maintenance activities for the entire project after its completion. The third area will enable the improvement of healthcare processes and access to healthcare services, as well as education and training for target groups.

The position of the HIS within the eHealth project
Despite the ambitious eHealth strategy, most of the project goals have remained unfulfilled. Namely, the current HIS infrastructure includes components facilitating only a few peripheral functionalities (Smart Cards, professional cards), which do not yield tangible benefits for either patients or for healthcare professionals and healthcare system managers. Due to leadership issues and a lack of coordination, as well as financial restrictions and technical problems, eHealth development has recently stagnated in almost all key areas, while the main project deliverables in the form of infrastructure building blocks have not reached the desired level of development according to the schedule. Consequently, the current HIS infrastructure is not fully functional and causes considerable time and resource losses.
3.2 Review of recent developments
The HIS is still deep in the phase of implementation and due to technical difficulties and public finance restrictions, the date of its completion is rather difficult to determine. However, the analysis of the European Commission and the OECD report regarding eHealth and HIS development in EU Member States [6, 7, 52] revealed various deficiencies of the Slovenian HIS, namely Slovenia is lagging behind the EU28 average in almost every aspect.
The author and the expert team outlined the main components of the HIS and tried to provide an expert evaluation of these components based on their level of sophistication. The level of sophistication was evaluated by applying the following grades (explanations in parentheses):
Conceptual phase (the component and its operations are based only on the conceptual design; development, sourcing, and implementation procedures have not yet been defined or started);
Development phase (there is a concrete blueprint for the construction of the component encompassing all planned operations. Development, sourcing, and implementation procedures have been defined, initiated, and monitored);
Partly functional (some of the planned component operations are implemented, functional, and applied in practice within the healthcare environment);
Functional (all of the planned component operations are implemented, functional, and applied in practice within the healthcare environment).
Results disclosed significant deficiencies concerning the hitherto development of the HIS (Table 1). Investigation of the functionality and deficiencies of the existing HIS exposed substantial discrepancies that have a significant impact on data collection and aggregation, and consequently do not allow their effective utilization for improving healthcare services and evidence-based management of the healthcare system.
The main components and operative deficiencies of the HIS

Taking into account the complexity of the components listed above, the time required for their transfer into operational use, and current budgetary restrictions, it is clear that operations depending on these components, and consequently the entire HIS, will not become fully functional for a long time. The deficiencies exposed have a significant impact on the overall healthcare process and evidence-based management of the healthcare system. The most significant deficiencies concerning the development and implementation of the HIS on the national level are summarized below:
absence of top-down support for the implementation of the HIS;
poorly defined healthcare policies, strategies, and HIS objectives;
an unadjusted and hyper-regulated normative framework;
a lack of management skills, leadership issues, human resources, irregular and inadequate funding;
fragmentation and a large number of diverse legacy ISs at all three levels of the healthcare system;
incompletely defined communication network standards and data exchange standards;
a lack of standardized definitions of health and social data required for the development and management of EHR, PHR, and DRG;
disregard for the interoperability perspective while procuring an increasing number of narrowly specialized ISs;
inadequate and vague evaluation practices in the fields of major IT projects;
a lack of experience in the execution of complex and long-term national (IT) projects;
a lack of awareness of the potential benefits of the HIS and a lack of IT skills on the part of healthcare professionals;
a lack of consensus on development priorities and a lack of cooperation and coordination between key stakeholders.
3.3 Construction of the conceptual HIS model
Depending on the multidimensional structure of healthcare systems and the increasing particularization of IT portfolios, HISs are inherently heterogeneous. They contain a wide variety of diverse, locally deployed, and narrowly usable software and hardware products, which appreciably hinder their integration into a consistent apparatus for healthcare information management and decision-making support.
This situation has triggered the development of several generic methodologies for the design and construction of HISs. We used adapted 3LGM methodology and its upgraded version 3LGM2 as a meta-model for modelling HISs. The original 3LGM2 concept was presented nearly two decades ago [44], in order to reduce complexity and eliminate redundancy during the planning and construction of HISs, and thereby obtain a transparent overview of the interactions and corresponding information flows between the entities in the healthcare system. 3LGM2 had been designed to support HIS planning and construction as well as information management on all levels of the healthcare system.
3LGM2 distinguishes three layers of HISs that provide a framework for describing both information processes at the domain layer and communication paths between application components and their interdependencies [53, 54]. The domain layer of 3LGM2 outlines a healthcare system independently, regardless of its enterprise functions. Enterprise functions have to be performed by the healthcare organizations executing their business processes in order to achieve their goals. In order to perform these enterprise functions, information of a certain type about the physical or virtual elements of healthcare organizations is needed. These types of information are represented as entity types. Enterprise functions may interpret or update information about entities of certain entity types. The logical tool layer focuses on application components supporting enterprise functions. Application components are responsible for the processing, storage, and transfer of data representing entity types. Component interfaces ensure communication between application components. The physical tool layer consists of data processing components that are physically connected via data transmission connections. They carry the application components [54].
While our research concentrated predominantly on the construction of a conceptual HIS model corresponding to the needs of the Slovenian healthcare system, the pertaining 3LGM2 tool was not applied. In constructing our own conceptual model, we focused primarily on the lack of information connections and the exchange of clinical and managerial data between the key stakeholders of the healthcare system. The latter issue was identified in our study as the main deficiency of the current HIS, as it is still under construction. Below we will present short descriptions of the construction phases and individual layers according to the authors of the 3LGM2, their visual representation, and their final integration into the conceptual model.
3.3.1 Domain layer
The domain layer (Figure 2) describes a healthcare system independently of its enterprise functions. Enterprise functions need information of a certain type about the physical or virtual elements of the healthcare system. These types of information are represented as entity types. The access of a function to an entity type can be represented as a ‘using’ or an ‘updating’ notation that is expressed by the attribute access type of the association class access [54]. Enterprise functions and entity types can be hierarchically structured using the respective ‘is_part_of’ associations [54]. Designated functions are performed by organizational units. Which entity types and functions are modelled depend on the specific national characteristics of the healthcare system. The domain layer of the meta-model outlines just the static view of the healthcare system. Thus, there are no associations between functions that represent processes.

Example of the domain layer
3.3.2 Logical layer
At the logical tool layer (Figure 3), application components are the main segment. Application components support enterprise functions and are responsible for the processing, storage, and transmission of data representing entity types. Computer-based application components are controlled by application programmes. Communication interfaces ensure the communication among application components (component interfaces), but also between an application component and a user (user interfaces) [54]. A component interface is based on a message exchange standard and can receive or send messages of a certain event-message type. Event-message types are composed of an event type and the message type or document type caused to be communicated by that event type. For communication among application components, communication links can be defined as relations between two communication interfaces [53, 54]. Each communication link is described by the eventmessage types that in fact are communicated. Figure 3 presents an example of a logical layer designed with the 3LGM2 tool [54], it shows computer-based application components: a patient management system (PMS), a radiological information system (RIS), a laboratory information system (LIS), a communication server (ComServ), a healthcare management system, and some further sectoral application components.
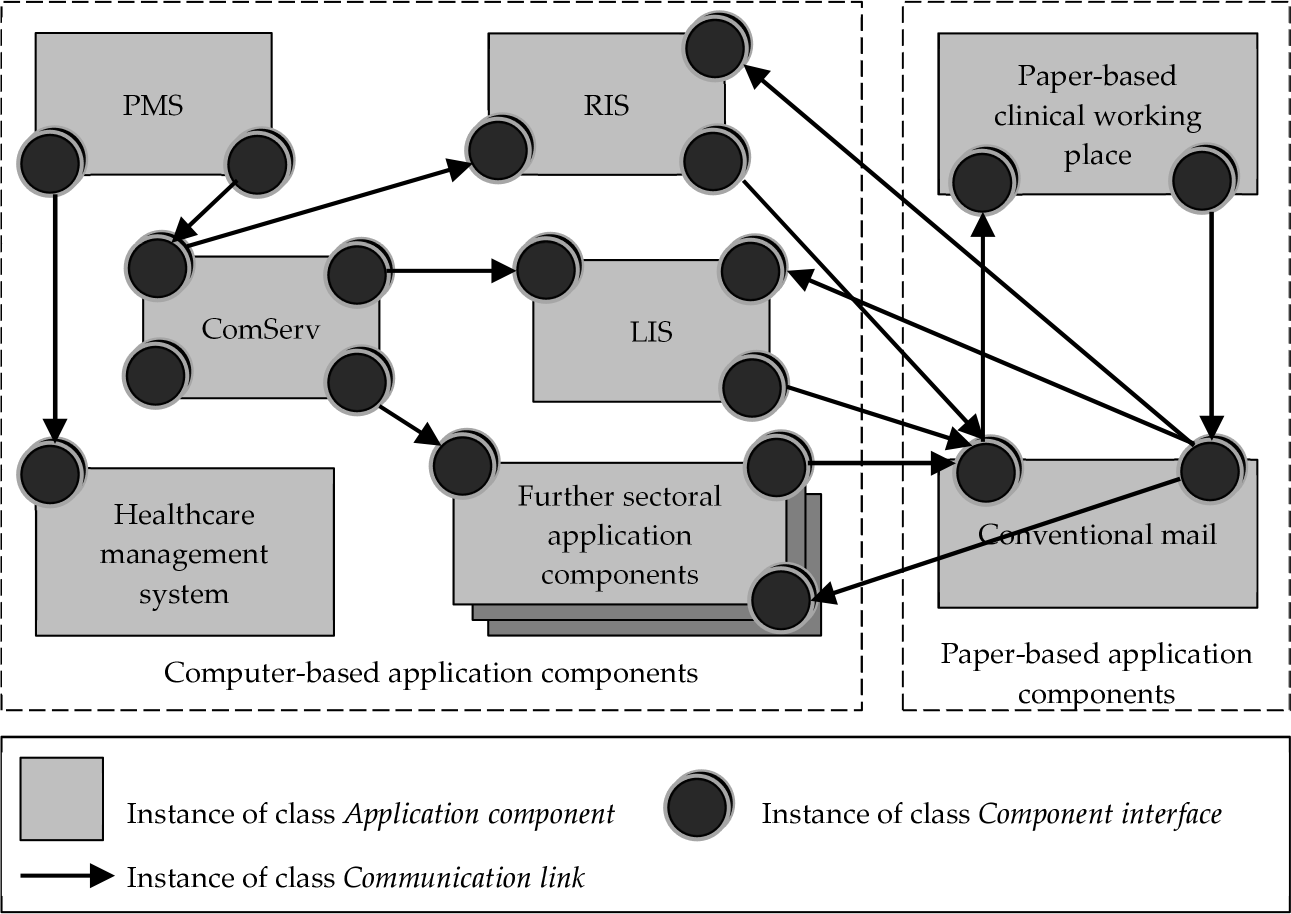
Example of the logical layer
3.3.3 Physical layer
The physical tool layer (Figure 4) is a set of physical data processing components that are used to realize the computer-based application components. Physical data processing components can be the human actors, telephones, books, and patient records that are used to support the paper-based application components, or computerbased components (such as terminals, servers, personal computers). Components can be physically connected via so-called data transmission connections (e.g., data wires) [53, 54]. The constellation of these connections between computer-based components leads to physical networks that are based on the network protocols. Figure 4 shows an example of the physical layer. In this example, we see a server for each sectoral application component (LIS server, RIS server, and the server for further sectoral application components) and a central server where the PMS and the healthcare management system are installed [53, 54]. Each server is connected to a set of personal computers.

Example of the physical layer
By merging all three layers, we present a conceptual HIS model below (Figure 5). A variety of dependencies, called inter-layer relationships, exists among the concepts of different layers. These inter-layer relationships may be used to detect shortcomings at the logical or physical layers which make it impossible to satisfy the information needs at the domain layer. Considering the domain layer and the logical layer, the most important relationship is between enterprise functions and application components [54]. While constructing our conceptual model we focused especially on the healthcare system entities, data, and information flows, and their operative and functional integration. Our study revealed that this is one of the biggest problems concerning the construction of a comprehensive national HIS and in facilitating the wide-ranging informatization of the Slovenian healthcare system.

Conceptual HIS model
The presented 3LGM2-based conceptual HIS model integrates all levels of the healthcare system (primary, secondary, and tertiary levels) including citizens via the National Health Portal, and all key institutional stakeholders within the healthcare system:
The Ministry of Health;
The Health Insurance Institute of the Republic of Slovenia (HIIS);
The National Institute of Public Health of the Republic of Slovenia (NIPH);
The Statistical Office of the Republic of Slovenia (SORS);
Insurance organizations – public and private;
Pharmacies – public and private.
Business (functional and structural) and informational (logical and physical) elements, including inter-layer relationships (connections, dependencies) and information flows are positioned on three individual layers. All three layers are merged into the single 3LGM2 framework presented in Figure 5. The inherent characteristics of the individual layers facilitate horizontal integration of complementary components on each layer as well as communication and data exchange between matching components on each layer in the vertical direction.
The domain layer focuses on the business aspects of the healthcare system, outlining the behaviour of the organizational units within such and their actions. This layer defines business functions, processes, activities, and tasks that are dependent on the certain type of information needed for the execution of these actions and subsequent achievement of the strategic business objectives. Different types of information are designated as entity types.
The logical layer outlines the integrated and business process-oriented application components. They facilitate the processing, storage, and transfer of clinical, managerial, and administrative data to the domain layer, thus enabling the execution of business functions, planning, and management of the healthcare organizations and the healthcare system in general. Controlled by application programmes, application components use interfaces to assist standardized communication between each other, and between application components and users at the domain layer.
The physical tool layer consists of physical data processing components. This layer provides a platform that enables the operative functioning of application components at the logical layer. The physical data processing components that appear at this layer can act as subjects or objects (human resources, personal computers, mobile devices, servers, paper documents, etc.). Physical data processing components connected via data transmission connections form internet-based networks, which should be able to support the operations of upper layers and provide much needed flexibility and scalability of the HIS.
The main objective of the 3LGM2 model is to maximize HIS synergies and provide informational integration of all entities within the healthcare system. The 3LGM2 concept is intended to facilitate IT support for the execution of healthcare, managerial, and administrative processes, and consequently improve the operation of the entire healthcare system. Coordinated action of the three layers is the main advantage of the 3LGM2 concept and should constitute the central segment within the informational architecture of the healthcare system. In order to develop effective applications and optimally exploit the potentials of the integrated national HIS, the entire IT architecture must be embedded in a broader enterprise architecture framework. Its foundation has to contain a comprehensive and thoughtful strategic base, while its upgrade should include a corresponding implementation plan ensuring the realization of the business and healthcare objectives. The successful development of healthcare enterprise architecture has to be supported on one hand by consistent strategic and operational documents, while the complete architectural solution must be built on the basis of robust architectural principles and business objectives, taking into account the interests of stakeholders as well as various healthcare system restrictions.
Conceptualization of the HIS based on the 3LGM2 model facilitates transparency and control in all phases of the construction process. The 3LGM2 modelling technique expedites the analysis of information needs and information flows in the vertical direction through all levels of the healthcare system, as well as in the horizontal direction, thus encompassing individual healthcare organizations and the healthcare system in general. Quality construction of each layer (domain, logical, and physical layer) based on the 3LGM2 model and a precise definition of the building blocks, especially in the reference model of the domain layer [55], enable the establishment of consistent interconnections between elements at different layers and effective data interchange between the entities involved. The presented approach allows for important interrelationships to be identified, including alignments between application components and organizational functions, reducing the risks of fragmentation, duplication, and a lack of interoperability. Moreover, the transparently structured design of the 3LGM2 model alleviates complexity problems, which significantly expedites the construction and implementation of the HIS, and ultimately promotes its application. A 3LGM2-based HIS enables effective communication and unrestricted exchange of management, administrative, and medical data between the key stakeholders in the healthcare system. The main constraints of 3LGM2 utilization can be seen particularly in the exhaustive and time-consuming construction process, requiring a lot of preparatory work and pre-prepared items (for example, a pre-defined reference model of the domain layer), as well as detailed knowledge of the organizational, structural, business, and information entities taking part in the healthcare process.
4. Recommendations and Guidelines
While analysing the recent developments in the field and opportunities for the application of 3LGM2 methodology for the construction of the national HIS, we identified various deficiencies which, in our opinion, have substantially affected the hitherto development and implementation of the HIS. Some of the problems identified were expected, given the scope and complexity of the HIS, while the other complications appeared unpredictably and resulted from poor planning, inaccurate analysis, and inadequate funding. The identified issues are of paramount strategic importance as they can seriously mark the future course of the HIS in Slovenia, and in some cases can even pose a fatal threat to the final and highly anticipated introduction of the HIS into the healthcare system. Stemming from the Slovenian experience, the findings could also provide a useful platform for HIS development and implementation in other countries facing similar problems, despite different contextual factors and system dynamics.
Synthesis of the case study evidence and derived deductions are presented in the form of recommendations and guidelines below:
Ensure political support from the highest level, bring together stakeholders from the public sector, not-for-profit organizations, and the private sector; ensure the necessary funds, human and other resources; prepare credible and viable strategy documents, feasibility studies, and action plans (define all parameters of the HIS project and set measurable objectives, align project objectives with healthcare system objectives, analyse the different informational needs of the primary, secondary, and tertiary levels of healthcare, define appropriate medical, administrative, and financial indicators for management needs, check the financial parameters and financial projections related to the HIS budget in the medium and long term, examine potential obstacles to the realization of the HIS, assess the risks and conduct a sensitivity analysis, etc.); promote international collaboration; provide evidence-based projections for the development of the HIS in the future;
Mobilize all stakeholders to ensure commitment and material and moral support; encourage their active participation and constructive criticism; promote collaboration between policymakers, healthcare professionals, healthcare management, IT professionals and users; adopt an inclusive plan for the continuous education of stakeholders and communication within the project team;
Promote legislative amendments and adopt necessary regulations concerning the implementation of the HIS (personal data protection, liability and risk issues, data storage and security, professional ethics, intellectual property, terms of use, electronic signatures, record keeping, transfer of data and lab results for medical purposes, maintenance of the system, recovery of data, etc.) and harmonize national legislation with international standards, recommendations, and resolutions (international cooperation, bilateral and multilateral agreements, healthcare service and health insurance issues, the transfer of medical data to other countries, etc.);
Examine current and projected healthcare issues; incorporate country specificities; determine national healthcare priorities; identify health targets and beneficiary groups; define the nature and coverage of services and projected results; and provide an action plan clearly specifying how the HIS will contribute to addressing the national healthcare priorities, as well as to enabling the desired reorganization, business process reengineering, and restructuring of the healthcare system itself;
Establish a robust evaluation framework including the motivations and objectives of evaluation, stakeholder groups, benchmark and evaluation metrics, qualitative and quantitative data; define and specify strategic and operative measures;
Select a top manager and a quality project team with experience in large IT projects; form a steering committee including diverse experts; assess risks and define change management issues; clearly structure the project plan, project phases, budgets, and deliverables for each phase; determine the objectives and timeline of the project by reaching mutual consensus with all stakeholders; distribute assignments and strictly monitor and inspect work on the project;
Ensure adequate resources before the start of each phase of the project and make realistic plans in both temporal and financial terms; define milestones; and analyse capital and operating costs;
Enhance the preparation and implementation of public tenders (materially and procedurally) related to the procurement of IT equipment and the realization of smaller tasks within the overall HIS project; arrange for joint public procurement;
Perform constant supervision and strict control of already executed project tasks with respect to substantive and temporal objectives and ensure close monitoring of tasks that are in the execution phase;
Improve or build a comprehensive IT infrastructure (assess the current IT infrastructure, departmental ISs, legacy ISs, interoperability issues, broadband connections, operating systems, technical solutions, interoperability platforms, network protocols, data standards); provide a blueprint for future enterprise architecture (business, application, and technology layers); encourage the transfer of good practices (case studies, international experience, consultancy, etc.); specify and adopt standard technical and medical protocols (e.g., DICOM 5 [56] for imaging, XML, HL7, ICD 10 AM for the exchange of medical data); deploy intended HIS components and technical solutions; ensure testing, optimization, and a technology watch; ensure quality maintenance of the system and focus on innovations and development;
Test the applicability of HIS components in pilot projects and gradually implement HIS solutions in healthcare institutions; promote the application of HIS services (ensure contingency plans); organize education and training of medical staff; facilitate internal and external communication and collaboration; provide service standardization; align business processes with medical protocols; organize a new business model; ensure openness to user opinions, ideas, and criticism; provide a reasonable transition period; arrange for early detection and problem solving;
Inform and sensitize the public; promote hitherto project achievements; organize a marketing campaign to popularize the HIS project and increase user acceptance of HIS services; facilitate helpdesks in healthcare institutions (online); gain support from the media, experts, and citizens; the HIS is a socio-technical project.
The listed recommendations and guidelines depend on several success factors and cannot be easily transferred into practice. They provide a multitude of necessary activities, some of which can be carried out simultaneously, while others have to be performed in chronological order. All these cooperative activities must be combined into functional and well-coordinated actions, which is essentially the most challenging task of the management team. Delays in HIS development and implementation require a detailed analysis of the current situation, accommodation of new resources, and well-coordinated implementation of operational tasks, which will gradually bring HIS development to its final phase. These measures usually necessitate a radical change in the project management and government financial stimulus. An alarming socio-economic situation can jeopardize the latest efforts and compel the government to focus on predominantly short-term economic issues and lower investments in the development and implementation of the HIS, which could result in far***reaching and irreversible implications for public health in the future [57]. The determination to resolve the problems concerning the HIS, enable better exploitation of IT, and eventually provide clinical and economic benefits as well, will therefore require the mobilization of all stakeholders and experts in the field, the definition of clear and measurable objectives, and a consensus on the necessary public expenditures, which will continue to grow with each day of delay.
5. Conclusion
Being aware of the almost unparalleled role of IT in the modern healthcare system, the HIS is currently a very hot topic in Slovenia (and possibly elsewhere), and it may define the main trajectory of healthcare system development in the upcoming years. Its level of sophistication and distinctive trends in the field authentically reflect the ambitions of the healthcare system, and reliably articulate the long-term goals of national health policies. Construction of a comprehensive HIS, bringing together a wide variety of fragmented and often non-interoperable legacy ISs, requires the alignment of health policies and informational, organizational, business, and other factors within the healthcare environment into an efficient mechanism, which can contribute to the improvement of public health. Insights and experience from other countries have shown that operative strategies and a well-developed modelling approach decrease the hazard of costly mistakes stemming from applying provisional IT solutions and deploying the HIS in an unplanned and unstructured manner. Nevertheless, it is evident that the difficulties in the development of the Slovenian HIS extend to various areas, while the ongoing financial and economic crisis has simply revealed the magnitude of the associated problems, further undermining public trust and stakeholder engagement. Successful development and implementation of the HIS clearly requires government impetus, the mobilization of all stakeholders, and their maximum consensus on the various and often conflicting issues within the healthcare system.
The presented research does not seek to impose a ‘one-size-fits-all’ solution to the myriad of problems related to the development, implementation, and utilization of HISs. However, it could provide an applicable platform for the identification and definition of acute problems, and hopefully accelerate the enactment of appropriate measures for the impending implementation of the HIS in Slovenia. Although reasonably susceptible to subjective interpretations, the conducted case study provides valuable insight into the recent developments concerning the HIS in Slovenia, presents a potential modelling approach for the construction of HISs, and provides a set of general recommendations and guidelines for the effective development and implementation of HISs. Despite certain methodological dilemmas, the conducted case study reveals the intricate dynamics behind the informatization process, related deficiencies and barriers, while designated recommendations and guidelines may eventually provide the groundwork for further development and gradual implementation of multifaceted and costly HISs. The main limitations of the research probably relate to the 3LGM2-based conceptualization of the HIS, which, due to obvious reasons, was hypothesized without empirical testing and practical validation in a healthcare environment (although it was conceptualized in collaboration with experts from the healthcare system). Accordingly, the issues related to the construction of adequate HIS layers (the pertaining components and building blocks), and their objective definitions, raise some important questions of principle, while the research outcomes may therefore be arguable. These issues should be properly resolved in further research and successive experiments aimed at establishing a practically validated modelling approach and its trial testing in a real healthcare environment. Notwithstanding these difficulties, the development and implementation of a comprehensive HIS in Slovenia, and possibly elsewhere, certainly represents a development opportunity which can, subject to proficient coordination with other ecosystem factors and pending structural reforms, ensure better utilization of public healthcare resources and provide tangible public health benefits.
Footnotes
1
International Statistical Classification of Diseases and Related Health Problems (ICD 10 AM) is a medical classification list developed by the WHO. It codes for diseases, signs and symptoms, abnormal findings, complaints, social circumstances, and external causes of injury or diseases.
2
Electronic Data Interchange for Administration, Commerce and Transport (EDIFACT) is an international standard developed under the United Nations. It comprises a set of internationally agreed upon standards, directories, and guidelines for the electronic interchange of structured data between independent computerized information systems.
3
Health Level Seven (HL7) is a set of international healthcare informatics interoperability standards developed by Health Level Seven International. The HL7 network provides a framework and related standards for the exchange, integration, sharing, and retrieval of electronic health information.
4
Extensible Markup Language (XML) is a markup language that defines a set of rules and standards for encoding documents in a format that is both human***readable and machine-readable. It was developed by the World Wide Web Consortium (W3C).
5
Digital Imaging and Communications in Medicine (DICOM) is the international standard for medical images and related information (handling, storing, printing, and transmitting information in medical imaging). It defines the formats for medical images that can be exchanged with the data and quality necessary for clinical use.