
Abstract
Introduction
Active Assisted Living (AAL) technologies have emerged as a multidisciplinary endeavor driven by the imperative to enhance the lives of older adults. However, users’ perspectives on the ethics of AAL technology use are often secondary considerations.
Objectives
The objective of this scoping review was to synthesize the literature on users’ perspectives on the ethics of AAL technologies to bridge the gap in both academic and non-academic contexts.
Methods
This scoping review was conducted comprehensively using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses-Scoping Reviews (PRISMA-ScR) in Covidence, focusing on peer-reviewed publications from 2000 to 2023. Our search strategies integrated concepts of AAL technologies, ethics, and user perspectives. Inclusion criteria encompassed qualitative and mixed methods that obtained users’ perspectives on AAL technologies in smart home communities. A gray literature review was also conducted to retrieve documents for analysis that incorporated guidelines, standardization, and/ or recommendations.
Results
Five relevant articles utilized qualitative methods (n = 3) and mixed methods (n = 2). Privacy and data protection were highlighted, with users expressing concerns about data tracking (n = 4). Respect for autonomy was emphasized in decision-making regarding technology use (n = 3). Accessibility issues pertained to missing accommodations for some physical abilities (n = 2). Diversity and social inclusion were important for social engagement and mental health support (n = 2). Perceived beneficence was also cited as a factor in improving health outcomes (n = 3). Transparency and accountability by the AAL technologies implementers were deemed essential for building trust (n = 1). The gray literature review yielded six relevant documents that included discussions on ethics and the use of AAL-related technologies for older adults.
Conclusions
Older adults are willing to include wearables and Internet of Things devices in their AAL technologies ecosystem, especially when they co-design the technology, but it is contingent on the implementation of ethical principles such as safety, security, and privacy to counter intrusive monitoring systems. This scoping review has the potential to offer valuable insights to various stakeholders, including tech developers and designers, providers, health policymakers, providers, and regulatory agencies.
Keywords
Introduction
Background and motivations
Active/Ambient assisted living (AAL) technologies are used to support older adults (aged 65 years and above) and individuals with disabilities to live as independently as possible in their daily lives 1 —these AAL technologies have prompted discourse on ethical implications. Such discourse often centers on care recipients’ risk of social isolation versus empowerment (autonomy) and the ensuing privacy concerns.1–3
The inception of AAL can be traced back to the early integration of simple assistive devices into living spaces in the 1990s. The first of its kind AAL technology for older adults was geared toward response systems in personal, social, and community settings. 4 Older adults would wear a pendant or alarm button could be used during a fall to call for assistance from a 24-hour call center. 4 Then, after the second generation of AAL technology appeared in the early 2000s, due to ICT advancements, there was a paradigm shift in the mid-2000s away from reactive systems designed to respond to specific demands to proactive environments capable of anticipating the needs of residents. 4 More recent and significant advancements in sensor technologies, machine learning, and ubiquitous computing have catapulted this evolution even further.
Integrating smart sensors and devices into the domestic environment has been a cornerstone of AAL technology development. 4 These sensors collect data on environmental conditions and the activities of residents, allowing for real-time monitoring and response. 4 The miniaturization and reduced cost of sensors have facilitated their widespread adoption in creating ‘smart homes’ tailored to the needs of older adults. 5 Furthermore, the development of AAL technologies has been influenced by the growing field of human-computer interaction, focusing on creating user-friendly interfaces and interactions. 6 Considerations of ergonomics, usability, and accessibility have been paramount, ensuring that AAL systems are adaptable to the varied capabilities of older adults. 6 Machine learning algorithms have also played a pivotal role in advancing AAL technologies. These algorithms process vast amounts of data that sensors collect to learn behavior patterns and detect anomalies that may indicate emergencies or deteriorating health conditions. 7 The predictive capacity of these systems offers a proactive approach to healthcare and personal assistance.
Interdisciplinary research has significantly contributed to refining AAL technologies, incorporating insights from behavioral sciences to understand the needs and preferences of older adults, especially where stigma is attached in cases of dementia. 8 This has led to the development of systems that support individuals with physical limitations and cater to cognitive and social well-being. Moreover, the progression of AAL technologies has been marked by an emphasis on care recipients-centered design principles. 9 This approach ensures that the development of technology solutions is aligned with the real-world needs and preferences of the care recipients, facilitating greater acceptance and effectiveness. The funding and collaboration across public and private sectors, including healthcare providers, technology companies, and academic institutions, have been instrumental in driving the research and development of AAL technologies. Also, government initiatives have often played a crucial role in providing the necessary resources and regulatory frameworks to foster innovation in this field. 10
Therefore, it follows that the development of AAL technologies should continue to be a multifaceted endeavor that reflects a synergistic effort among various stakeholders. It should encapsulate a forward-thinking approach to accommodate shifting demographics and preparing for a future where technology seamlessly integrates into the fabric of daily living to enhance the autonomy and quality of life of older adults.
Early ethical considerations in AAL technologies
Historically, AAL technologies used to support elderly adults and individuals with disabilities in their daily routines have prompted significant ethical discourse. Such discourse often centers on users’ autonomy, privacy concerns, and the risk of social isolation versus (individual and social) empowerment. 11
One of the earliest ethical issues in the field of AAL revolved around the balance between safety and privacy. 12 Technologies such as monitoring systems that track an individual's movements or physiological functions were perceived as intrusive. In response, guidelines were developed to ensure that such systems were implemented with the utmost respect for the care recipients’s privacy and consent. 13 This was often achieved through transparent data policies and care recipients-centered design principles emphasizing empowerment and care recipients’ control. Furthermore, the potential for AAL technologies to contribute to social isolation has been another point of ethical scrutiny. As a countermeasure, researchers and developers were encouraged to design technologies that promoted social interaction and community engagement, thereby ensuring that AAL solutions contributed positively to the care recipients’s social well-being. 14
Ethical issues have also been studied in the field of biotechnology and healthcare as bioethics, and have played a significant role in developing and guiding the use of AAL technologies. Bioethics encompasses a range of concerns, including the ethical implications of biotechnology 15 and the moral dilemmas created by advanced medical technologies. 16 These concerns are particularly relevant in AAL technologies, which often involve biotechnology and advanced medical devices.
Current research on the ethical considerations of AAL technologies ecosystems
Existing research often lacks a comprehensive analysis of the ethical implications of data management within AAL systems. The nuances of data ownership, the rights of individuals post-data collection, and the long-term stewardship of sensitive information require deeper investigation. Another significant gap is the limited scope of ethical considerations in diverse cultural and socio-economic contexts. Much of the current literature focuses on AAL technology implementation in high-income, westernized settings, leaving a dearth of understanding concerning how these ethical principles translate across different global contexts and cultural norms. 17
There is insufficient exploration of the ethical ramifications of AAL technology failure or malfunction. The moral and legal responsibilities in such scenarios remain underexamined, particularly concerning the care recipients ‘s safety and the continuity of care. 18 Although reviews on the ethical discourse around AAL technologies have included the perspectives of caregivers and healthcare professionals from a clinical and residential context in recent years, they frequently overlook the perspectives of care recipients interacting with these AAL technologies in their living environment. 18 Their insights into consent processes, autonomy, and care recipients’ engagement with AAL technologies are critical yet often marginalized in the literature. Moreover, the current body of research tends to treat care recipients using AAL technologies as a homogenous group, failing to adequately address the varying needs and ethical concerns of subpopulations such as those with cognitive impairments or chronic illnesses.
There is an emerging need to evaluate the ethical considerations of developments in AAL, such as the incorporation of artificial intelligence and machine learning. 19 The predictive algorithms and decision-making processes intrinsic to these advancements introduce complex ethical considerations yet to be fully explored, but this is beyond the scope of the review. The motivation for this scoping review emanates from the need to synthesize our knowledge of the ethical use of AAL technologies. Essential considerations such as who owns the data, data safety, usability of technology, and consistent provision of remote care merit further examination, and this review aims to fill those gaps. To understand how these technologies affect care recipients in the long term, this review will collate existing knowledge and suggest ways to conduct additional research. This is necessary to help us understand how AAL technologies may affect people's independence and privacy over time.
In doing so, we hope to offer ideas for managing data responsibly in AAL settings by exploring these issues. Another reason for this review is to ensure that the discussion about AAL ethics considers different socio-cultural and economic backgrounds. Since access differs among the care recipients using AAL technologies, we want to ensure that ethical guidelines are fair and consider everyone's needs. Finally, as AAL technologies keep advancing, especially with new developments in AI, we need to consider the ethical issues that might arise. The scoping review, or review, is driven by the need to create ethical guidelines to keep up with these fast-paced developments without sidelining the perspectives of the care recipients since, historically, caregivers’ and healthcare professionals’ viewpoints about these technologies have been substantially documented. This review has the potential to offer valuable insights to various stakeholders, including developers, designers, health policymakers, providers, patients, researchers, and health insurance companies.
Objectives
Our objective was to synthesize the literature on the ethical use of AAL technologies from care recipients’ perspectives. Essential considerations, such as who owns the data, data safety, usability of technology, and consistent provision of remote care, merit further examination, and this review aimed to fill those gaps. In phase 1 of our Ethics in AAL Technologies project, we sought to answer the research question, “What are the ethical considerations of AAL technologies use in the context of seniors’ continuum of care from the perspective of patients/clients?”
Our scoping review findings will be used to inform phase 2 of our project (whose results will be published elsewhere), and address the research question, “Based on the evidence on ethical considerations from the perspective of patients/clients, what are the best practices for the implementation of AAL technologies use in the context of seniors’ continuum of care?”
The research questions were developed from the research proposal submitted to Mitacs (our funding agency) and our industry partner, the CSA Group, in 2021, for a multiyear and multiphased project.
Methods
A scoping review protocol was drafted but not registered on the PROSPERO platform as PROSPERO does not accept scoping reviews.
The research team was led by an expert in AAL Technologies research studies (PPM) and managed by a seasoned public health sciences researcher (THP). The research team has expertise in gerotechnology, especially in deploying and applying smart home sensors, health informatics, machine learning, and health policy. The research team has prior experience crafting multiple scoping reviews and applying qualitative research methods.
We used the principles outlined in Arksey and O’Malley
20
and improved in Levac et al.
21
Identifying the research question (The research question was identified in a team meeting). Identifying relevant studies (This step was completed using agreed upon search terms). Study selection (This step was completed using the Covidence platform). Charting the data (This step was not followed in terms of two people charting). Collating, summarizing, and reporting the results (This phase was done iteratively through the writing process). Consultation (The first draft was shared with the CSA Group to critique).
In our methodology, we employed a content analysis approach elucidated by Vaismoradi and colleagues, which includes the researcher: (a) “Being immersed in the data and obtaining the sense of whole, selecting the unit of analysis, deciding on the analysis of manifest content or latent content and (b) utilizing open coding and creating categories, grouping codes under higher-order headings, formulating a general description of the research topic through generating categories and subcategories as abstracting.”22(p. 402) As such, quotes on experience with and/or AAL technology highlighted in the studies and relevant to the research questions were embedded in the review using predetermined categories. The categories included: (a) privacy and data protection, (b) respect for autonomy, (c) accessibility, (d) diversity and social inclusion, (e) beneficence, and (f) transparency and accountability.
We attempted to link them to an unvalidated framework of what stakeholders should consider when engaging with older adults and their use of AAL technologies: (a) “challenges of independent living; (b) availability of behavioral options to cope with challenges; (c) personal thoughts on technology use, (d) influence of their social network; (e) influence of organizations; and (f) the role of the physical environment,” 23 which coupled with the quotes further guided the discussion of our findings.
We conducted a systematic literature search using Covidence, a web-based platform, to streamline the review process. On 26 July 2023, we created a search term adapted to the source databases’ requirements and imported relevant references from multiple academic databases, including PubMed, IEEE—Xplore, and Scopus. Eligible literature was limited to peer-reviewed publications from 2000 to 2023. The year 2000 was a good place to start exploring the ethical considerations of AAL technologies because the systems were more advanced and generating data unprompted. 3 Due to the topic and its focus on health, Medline was excluded because of duplications appearing in PubMed, while Web of Science and EBSCOhost did not generate the results that were needed in our trial searches.
The search results were saved and organized within Covidence for further assessment and summarized in a Word document. The screening phases were divided into title and abstract screening and full-text screening. Two reviewers, THP and GM, independently evaluated each reference based on predefined inclusion and exclusion criteria. GBN resolved any conflicts in results between THP and GM for the title and abstract screening. Three reviewers, GM, SA, and THP, also independently conducted full-text screening based on predefined inclusion and exclusion criteria. THP resolved any conflicts in findings among GM, SA, and THP. Data extraction was completed on 1 November 2023 and the data was exported into an Excel CSV document.
Academic literature search strategy
Recently, Zhu and colleagues conducted a systematic review of the ethical issues surrounding smart home-based elderly care.
24
The focus of the systematic review was to generate knowledge on how nurses can best promote ethical awareness and practice when implementing AAL technologies by using the perspectives of older adults and stakeholders. Their search strategy generated 15 eligible studies from Chinese and English-language databases, including PubMed, EBSCO, Cochrane Library, and Web of Science. Studies that only had older adults’ perspectives were excluded. The publications were limited to 2015 to 2021. The focus was on seniors, AAL, information and communication technology/ ICT/ technology/ gerotechnology/ telecare and homecare/ community care, and ethics/ morality. [(“Elderly” OR “aged” OR “old people” OR “senior” OR “older adult”) AND (“smart senior care” OR “ambient assisted living” OR “AAL” OR “information and communication technology” OR “ICT” OR “technology” OR “Gerontechnology” OR “telecare” OR “homecare” OR “community care”) AND (“ethics” OR “morality”)]
Their search strategy generated seven eligible studies from English-language databases, including Scopus, PubMed, and IEEE-X. The publications timeline was expanded from 2000 to 2023.
Their search strategy resulted in 15 eligible studies from Chinese and English language databases, including PubMed, EBSCO, Cochrane Library, and Web of Science. 3 The publications were limited to 2015–2021, focusing on seniors, AAL, information and communication technology/ ICT/ technology/ gerotechnology/ telecare and homecare/community care, and ethics/morality. 3 The significant difference between Zhu and colleagues’ systematic review and our review was the incorporation of not only the perspectives of the older adults (alone) on the ethics of AAL technology use but also the addition of results of gray literature review including relevant standards and guidelines. Moreover, while Zhu and colleagues focused on nurses and their clinical work and how it impacted AAL technologies for older adults, they also required included studies to have both older adults’ perspectives and other stakeholders’ perspectives, which means they excluded our scoping review's included studies.
Although a systematic review ranks higher than a scoping review, our attempt at a scoping review was still justified because the systematic review excluded studies that only included older adults’ perspectives. We brainstormed different ideas and came up with a preliminary search plan and presented it to the university librarian JS responsible for the Faculty of Health. According to the librarian's suggestion, we used the following headings to develop our search strategy: Concepts, AAL, Technology, Location, and Ethical considerations. Each heading was then used to develop keywords for the search.
Concepts: “[tiab] = title/abstract, [tw] = title/abstract/ keywords/MeSH; AAL: Ambient assisted living, Active assisted living, Wearable, GIS tracking, Smart home, Technology: Technolog*, Sensors, Device*; Location: Smart communities, Homecare, Independent living, Retirement homes, Retirement villages Ethical considerations: Ethics, Ethical, Informed consent, Freedom.
Since our core focus was on older adults (65+ years) as a significant and aging demographic group, the current review was justified in constructing an academic search strategy using the concepts of seniors, ambient assisted living, sensors/devices/smart technology, ethics/rights, and smart communities/home care/independent living/retirement homes/ retirement villages/retirement.
Our final search term was: [“elderly” OR “senior” OR “old* adult” AND “AAL” OR “ambient assisted living” OR “active assisted living” AND “technolog*” OR “sensor*” OR “device” OR “smart tech*” AND “ethic*” OR “rights” AND “smart communities” OR “home care” OR “independent living” OR “retirement homes” OR “retirement villages” OR “retirement”]
Eligibility assessment and study selection from the academic literature
The initial search yielded N = 501 studies with n = 364 and n = 61 from Scopus and PubMed databases, respectively. Citation searching yielded an additional 76 studies. Covidence screening tool was used to manage the screening process. Fourteen (n = 14) duplicates were removed by Covidence and n = 487 studies were screened by English title and English abstract. At this stage of the screening process, n = 433 studies were excluded because they did not include all the relevant constructs from the search term (above) and the inclusion and exclusion criteria (below) necessary to proceed to full text screening (Table 1). Additional contact with authors was initiated via ResearchGate and by email to obtain full texts. Only one group responded, and we were able to review their paper, which was not eligible for inclusion.
Inclusion and exclusion criteria—academic literature search.

The data points were extracted from the studies into a table including authors and year of publication, country, target population, aims and purpose of the study, type of study and data collection method. Concepts to assess the relevancy of the studies included, ethical considerations, or synonyms, smart home AAL technologies or synonyms, and perspectives of older adults. Next, we conducted a content analysis of the quotes within the qualitative/mixed methods studies to find themes that matched existing themes in ethical considerations and to create new ones where there were gaps.
Gray literature search strategy
The gray literature search was conducted between 13 May 2024, and 31 May 2024. The search plan was developed with the guidance of two University of Waterloo librarians (JS and RB) using four different sources: (1) relevant databases, (2) Google search, (3) targeted websites, and (4) consultation with a Canadian Group advisor (FM). The relevant databases included the Institute of Electrical and Electronics Engineers [IEEE], the International Electrotechnical Commission [IEC], and the American Society for Testing and Materials [ASTM]. On Google, 11 targeted websites included The Canadian Standard Association, The Canadian Agency for Drugs and Technologies in Health, The Organization for Economic Co-operation and Development, International Standard Organization, Public Health Agency of Canada, Health Canada, Canadian Public Health Association, European Commission, World Health Organization, Canadian Institute for Health Information, Canadian Best Practices Portal.
Utilizing the librarians’ advice and similar to the academic literature review process, we used the following headings to develop our search strategy: Concepts, AAL, Technology, Location, and Ethical considerations. The search terms were developed to encompass the proposed search strategy and included AAL, Ambient assisted living, Active assisted living, AAL technology, Ambient assisted living technology, Smart communities, Smart homes, Home care, Agetech, Independent living, Ethical considerations, Ethical considerations of active assisted living, Ethical considerations of ambient assisted living technology.
The institutional librarians were consulted intermittently for guidance throughout the literature review process. The search strategy was developed using concepts deemed relevant to AAL technology in the context of older adults’ care. Four search terms were used to search the databases and organizations (active assisted living, ambient assisted living, ethical considerations for active assisted living, and standards for active assisted living) while additional keywords (ethical considerations of AAL technologies, best practices for AAL technologies, smart communities, standards for AAL technology, standards for active assisted living technology) were included in the Google search. All results from the databases were screened, while the first five pages of results from the target organizations and Google search results were screened for each keyword.
A research assistant (IM) conducted the screening process in five stages and organized the information in an Excel spreadsheet.
Initial screening of titles; Screening of abstracts, executive summaries, and table of contents; Removal of duplicates; Full-text screening; and Charting data.
Eligibility assessment and study selection from the gray literature review
The title and source organization of relevant documents that were obtained using the search approaches were added into an Excel sheet, and duplicates eliminated with Excel's duplicates removal feature. Since abstracts are often unavailable in gray literature documents, 3 the initial screening entailed reviewing the executive summary, abstract, or table of contents (whichever was available) for each document to determine relevance to the research objectives. If a document had multiple elements, then all were assessed for relevance. The next step involved the full-text review of all items that were moved to the second stage. The reasons for excluding any document at this stage were noted in a separate column. All documents that met the eligibility criteria after the full-text screening were included in the review: (1) Standards, books, editorials, letters, notes, practice guidelines, (technical) reports, whitepapers, commentaries, and preprints, (2) Documents that discussed ethical considerations of active assisted living (AAL) technologies, and (3) Documents that focused broadly on AAL technologies (Table 2).
Inclusion and exclusion criteria—gray literature search.

Articles that were excluded include: (1) Conference proceedings and articles published in academic journals, (2) Documents without ethical considerations of AAL technologies, and (3) Documents that did not explicitly include care recipients’ perspectives in the text.
A complete overview of the scoping review screening process is presented in Table A1.
Results
Academic literature search results
An institutional librarian who specializes in the health sciences recommended using the following databases for this scoping review: Scopus, IEEE Xplorer and PubMed, and excluded CINAHL, Web of Science, MedLine and Google scholar. The justification for not using the Web of Science is that it contains non-health related disciplines, which can create noise in the data. CINAHL was excuded because it is best suited for nursing and allied health, hence the reason Zhu and colleagues included the database in their systematic review. Since MedLine is accessible through PubMed, excluding it avoids redundancies, while the decision to exclude Google Scholar was due to its design limitations—it is not currently designed to capture academic literature only that can be seamlessly imported into the Covidence online platform.
Using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses-Scoping Review (PRISMA-ScR) reporting method embedded in Covidence, 501 studies were retrieved from three databases: Scopus (n = 364), IEEE Xplorer (n = 76), and PubMed (n = 61). Next, 14 duplicates were removed before the title and abstract screening (see Figure 1). After removing duplicates, 487 studies were screened, and 433 were excluded. Then, 54 studies were assessed for eligibility, and 45 were excluded. The reasons for exclusion were the following: Wrong outcomes (n = 1); Not in English (n = 1); Full text not available (n = 1); Wrong patient population (n = 1); Not “original research” (n = 20); No discussion of care recipients’ perspectives (n = 9); and no discussion on ethical considerations from the perspective of care recipients (n = 12).

PRISMA-ScR flowchart.
Finally, studies were included for full-text review. However, three were excluded at the data extraction stage because of either the wrong study design (n = 2: not qualitative) or included perspectives but not the targeted perspectives (n = 1: no care recipients’ perspectives). Therefore, our analysis will be based on five studies,25–29 summarized in the next section. All the search stages are summarized in a PRISMA-ScR flow chart in Figure 1. The search results excluded all the findings from Zhu and colleagues and, thus, there was no overlap making our review unique.
Summary statistics for the academic literature review
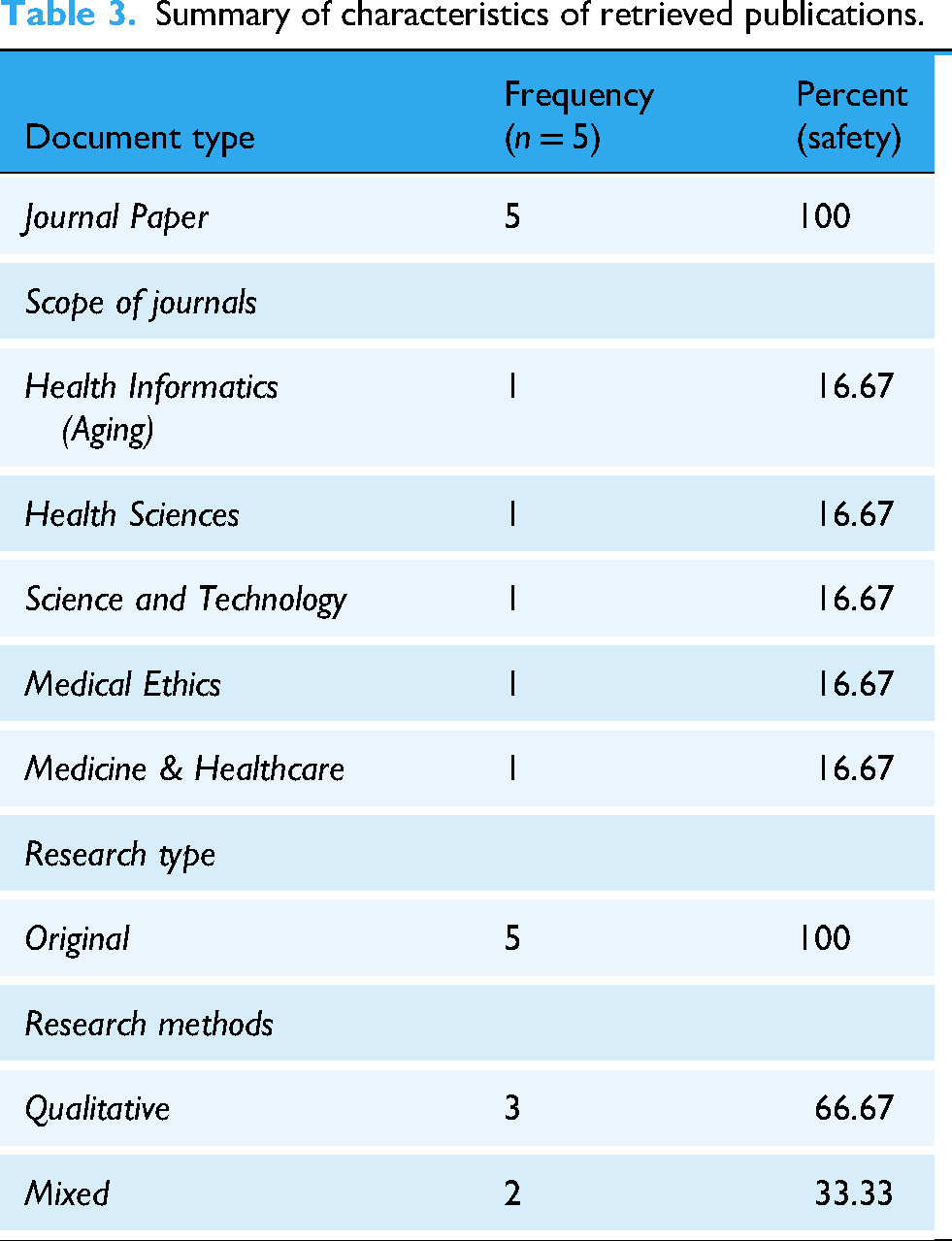
Through a systemic literature search, the review yielded five relevant articles and identified their characteristics (Table 3). These original studies were published in diverse journals with varying impact factors (1.9–4.8). The journals’ overarching themes were health, science, and technology, with a few focusing on aging specifically (n = 1). Summary statistics for the included studies are outlined under authors and year, country, target population, aims and purpose of the study, type of study and data collection method (Table 4). Findings were also assessed for relevancy to the scoping review by determining whether the articles discussed ethical considerations, AAL Technologies, and older adults’ perspectives.
Summary of characteristics of retrieved publications.
Summary of statistics for included studies.

Among the included publications, one was published between 2000 and 2010, two between 2010 and 2020, and three between 2020 and 2024 (Figure 2). Location-wise, three out of seven studies were conducted and reported in the USA alone, two studies were conducted and reported in Europe (Germany and the UK), and one study had multi-country sites in North America (Canada and the USA) (Figure 3). Finally, a third of the studies used a mixed-methods design, while two-thirds utilized solely qualitative methods (Figure 4).

Yearly distribution of published articles.

Country of study distribution of published articles.

Study type distribution of selected articles.
A more comprehensive overview of the search results is attached in Table A1.
Summary statistics for gray literature review
The gray literature search was conducted between 13 May 2024 and 31 May 2024. A total of 12,374 documents were extracted from searching Google (n = 969), 11 targeted websites (n = 4262), and three databases, including the Institute of Electrical and Electronics Engineers (IEEE) (n = 405), the International Electrotechnical Commission (IEC) (n = 4065), and the American Society for Testing and Materials (ASTM) (n = 2673) (Table 5). The eligibility criteria were applied to identify 12 standards and 29 non-standards (n = 41 documents) for full-text screening. Documents were excluded from the full-text screening if they (a) could not be accessed (n = 2), (b) were a conference proceeding (n = 1), (c) did not discuss ethical considerations of AAL use, or d) discussed ethical considerations in artificial intelligence but not in the context of AAL use (n = 21). One document recommended by a CSA Group advisor was also screened and included in the gray literature review.
Summary of research results.

Note. IEEE = Institute of Electrical and Electronics Engineers; IEC = International Electrotechnical Commission; and ASTM = American Society for Testing and Materials.
Seven documents fulfilled all eligibility criteria and were included in this review after the screening process was completed (Table 6). They included an IEC Systems Development Reference, a CSA Group Technical Report, an Alzheimer's Society factsheet, an Age Space guide, a European Cooperation in Science and Technology whitepaper, a Canadian Journal of Health Technology technical report, and a project report by AGE-WELL.
Document types.

These documents were published between 2015 and 2024 (Figure 5) in three different countries, namely the United Kingdom, Belgium, and Canada (Figure 6), from two Europe and North America, respectively.

Distribution of the year of publication of included documents.

Distribution of the country of publication of included documents.
Gray literature search findings
The gray literature search results identified one systems development reference and five documents from organization reports, blogs, guides, and factsheets that discussed the ethical considerations of using AAL technologies and the standards and best practices for implementing them in older adults’ continuum of care. A complete summary of the gray literature discussed in Table A2.
Perspectives of older adults on ethics for AAL smart technology use
The themes that emerged from the content analysis have been summarized below, with accompanying quotes where available. They include privacy and data protection (n = 4), respect for autonomy (n = 3), accessibility (n = 3), diversity and social inclusion (n = 2), beneficence (n = 3), transparency and accountability (n = 1). Privacy and data protection were highlighted by older adults in four out of six studies, thus emerging as the primary theme while transparency was the least discussed with the study highlighting care recipients’s concerns.
Privacy and data protection
As smart home technologies involve gathering personal data for visualization purposes, it is important to ensure that participants’ privacy is protected throughout the design process and that their data is handled securely. Some of the findings show that care recipients felt the tracking and monitoring of the data was beneficial for their general and specific health needs. I’m not sure I’d like my family to know when I take a bath or if I take a bath; it's something of an invasion of privacy, but I can see how … if you were unconscious, and [you needed help], I could see how it's a good thing. (Liza, 72 years)
26
Yet still, other care recipients expressed concerns about them being captured on video for the data points as being intrusive. I don’t like for anyone to know that I went out and didn’t get back until midnight or something like that—I don’t think anyone needs to know that. (Anonymous)
25
Because I think from the data you could monitor your life because you don’t monitor yourself, right, and I could be sitting here watching TV for about four hours and then if you keep on looking at the data, this is what you are doing every day… (Molly)
28
However, some older adults weighed the “cost” of moving into long term care and would opt for AAL technologies if that meant they could stay independent and at home for longer. If [AAL] meant being able to stay … home longer, then privacy would go out the door. (Sarah, 78 years)
26
In the gray literature, including the IEC SRD 63416:2023, the 2015 Alzheimer's Society Factsheet and the 2023 Canadian Journal of Health Technology (CJHT) report by Clark et al., and an Age Space report indicated that AAL devices should primarily benefit the care recipients and not inadvertently constitute a threat to them or their privacy.30–33 Subsequently, critical questions like who should access the care recipient's data, to what extent the data should be utilized, and under what circumstances the AAL system can act to enhance the safety of AAL users, should not be ignored. Whenever possible, AAL technology users or the substitute decision maker where applicable should be allowed to make decisions on who controls and oversees their personal health information. Data from AAL technologies should not be used in isolation and independent of the end users.
Respect for autonomy
Older adults should have agency in their decision-making regarding their participation in co-design activities. Their preferences and choices should be respected throughout the process. Some care recipients felt conflicted despite the perceived benefits of the social circle and caregiving ecosystem. So, my inner attitude rejects this [scenario involving the use of assistive technologies]. Whether it is beneficial or not is another issue. But my inner attitude says no. I don’t want this. […] (Interview 1, Anonymous)
28
So, you know, I don’t want it to be too Big Brotherish but somehow… (Bethan, 67 years)
29
My son lives some distance away and he can’t come visit me all the time. […] It would be very reassuring for him if he knew it [my health situation] was under control [via the use of these assistive technologies as in the scenario]. So, if he asked me if I wanted it, I would say no at first. Until maybe I do see the point of it, or perhaps he, let's say, forces me for my own good [to accept] that it's better after all. (Interview 2, Anonymous)
28
When it comes to it, I would rather die than be constantly monitored. That's what I’m saying now. It doesn’t mean I’m tired of living, but one could end up [feeling like this]. In a situation like that. […] (Interview 1, Anonymous)
28
And finally, a more concise sentiment was given by the same care recipient about their autonomy. I would like to make my own decisions, no matter how good or bad they are. (Interview 1, Anonymous)
28
In the gray literature, designers and deployers of AAL devices are encouraged to respect the autonomy of the care recipients and not, for example, limit care recipients’ movement due to a decline in mental and physical abilities. 23 Likewise, surveillance systems discourage behaviors even if the users may enjoy them to avoid triggering safety concerns. 34 This may remove decision-making about risk or perceived risk-taking behaviors from users since technology is being utilized to risk-manage users’ action and alert caregivers when needed. 34 Also, whenever possible, AAL technology users or the substitute decision makers should be allowed to make decisions on who controls and has oversight their personal health information. 23 Data from AAL technologies should not be used in isolation and independent of the end users. 23 Human dignity should also always be maintained, and the care recipients’ perceptions of being controlled by an AAL system should be addressed expediently. 23
Accessibility
The design process needs to consider accessibility features such as font size, color contrast or voice control options so that older adults with different abilities can actively engage in co-design activities. In addition, care recipients have noted issues with physical constraints and visual impairments. …make it user friendly, make it a bit larger so they can get hold of it, because they’ve got problems or issues with their fingers and thumbs…make sure that it's functioning… (Molly, 66 years old)
29
Also for a lot of people, including myself, I have actually had to, um, change what the clock looks like on, um, the Fitbit because the writing was too small and because I couldn’t read it and I, it, it, um, because my vision is bad, I actually have to keep the brightness on the highest about 90 some odd percent of the time. Because I can’t read it when it's darker. (Anonymous)
28
Additionally, the gray literature posits among other things that the lack of inclusion and inequalities in accessing AAL technologies due to economic and social disparities as strong ethical concerns. 23 They should also be able to consistently serve diverse users fairly and without discrimination despite declining cognitive abilities of users. 30
Diversity and social inclusion
A care recipient shared that having functions that could be displayed on a television or engaging with technology would be proxies for conversations with another person acting as their caregiver or friend. Like tell me how much I’ve moved all day and like how far I’ve walked or something…It is like if something had come on the telly every day and said, “Now Bethan, we’re going to do our exercises. Sit in the chair,” and I would have felt like I’d seen somebody and talked to somebody…You don’t think you’ve slept very much…. (Bethan)
29
So, you could have maybe set up a group online of people in their 70s who live in this neighbourhood who have similar interests and you could maybe have a conference call or a virtual meeting for people who can’t get out, that would be very good. (Kelly)
29
Maybe you’ve had the experience of having elderly relations that can only talk about their illness…but so I think is really important that we’re still able to maintain a relationship with the world […]. (Alice, 67 years)
29
Beneficence
Co-designed solutions need to prioritize participant well-being by addressing specific needs identified during engagement sessions. The perceived benefits to be accrued for their health and well-being would encourage the adoption of AAL technologies. I’m very worried that I might get dementia. FutureLearn [web-based education classes], they’re usually three-week, four weeks, six-week, eight-week courses. So, for instance, I’ve done one about dementia […] and they’re free! (Bethan)
29
Blood, cholesterol level and blood sugar level, […] I could actually read about results for things and work out what a good blood sugar level is or not and I can perhaps do something about my lifestyle…the results of my pulse's activity through the course of a day or through the course of a week or through the course. (Henry, 68 years)
29
…When I run out of the drugs I’m using the health portal, that goes straight to the surgery. (Daniel)
29
Other care recipients expressed the need for consultation and engagement in the design of AAL technologies because they had (more) knowledge and lived experience as older adults. … ethics and morality and seeing further from having lived longer that I think collective wisdom of the elderly might be extremely important in the checks and balances put in place. (Anonymous)
27
I think it's a deal of bioethics. Sometimes the 85 and above have more human knowledge than the people working in the industry. (Anonymous)
27
Participants suggested design aspects that would be beneficial for them. “Why can’t there be a feature on the TV that I can get the sound to come straight to my hearing aid electronically?” (Anonymous)
27
A care recipient also expressed the need for meaningful data production. I would adopt this technology if I could get a meaningful series of data, then I’d consider it probably being worthwhile. (Liam)
29
Bin Noon and colleagues identified the need for improved role definition regarding data control and privacy while recognizing the “privacy-utility –trade-off” that is inherent in AAL technology use in the context of care recipients’ continuum of care. 23 AAL technology used should prioritize direct benefits of the devices for care recipients over commercialization, and that AAL technology users should also be given full disclosure about the benefits of AAL devices as well as their rights to accept or refuse them. 23
Transparency and accountability
Researchers must maintain transparency about project goals, progress updates, etc. They also need a system of accountability where they address any concerns raised by participants. The results from the scoping review show that some care recipients were afraid of being deceived or of their data being mishandled. If they’re [the technology] so sensitive, they know three weeks before we know what's going wrong with our bodies. It seems to me that that kind of information could really be compromised, and seniors could, uh, who are very vulnerable, could really be hoodwinked more easily. (Wang)
25
The CJHT report also emphasizes a clear “opt-in” instead of an “opt-out” approach for users’ data be adopted to ensure the prioritization of data ownership and privacy over utilizing recipients’ information to enhance AAL technology. 32 Moreover, AAL technology users should be given the option to grant permission for their personal data to be collected and stored, rather than being asked after the fact if their personal data should be removed. 32
Other themes from the gray literature review
As a counterpoint, the gray literature noted that it was important to consider whether the AAL devices overcomplicate rather than simplify tasks for the users, or risk possibly reducing social interactions that they enjoy. 31 For example, adopting an automated pill dispenser when pills were dispensed by a caregiver in the past may result in less contact with that caregiver. 31
Finally, all our gray literature regarded the concepts of safety of users and data security as necessary for effective aging in place.25,35–33
Synthesis of scoping review findings
The scoping review aimed to synthesize our present knowledge of the ethical use of AAL technologies from the perspective of older adults. The studies systematically selected for this scoping review 29 and the gray literature 33 provided a substantive list of themes regarding the ethics of AAL technologies used for the older adult population. These are privacy and data protection, respect for autonomy, privacy and data protection, respect for autonomy, accessibility, diversity and inclusion, beneficence, and transparency and accountability which are also discussed in the White paper “Ethics by Design: An organizational approach to responsible use of technology.” 36 There are six key areas one can consider when discussing AAL technologies for older adults: (1) “challenges of independent living; (2) availability of behavioral options to cope with challenges; (3) (their) personal thoughts on technology use; (4) influence of their social network; (5) influence of organizations; and (6) the role of the physical environment.” 23 These key areas are summarized are linked to seven ethical principles including informed consent, respect for autonomy, accessibility, privacy and data protection, diversity and social inclusion, beneficence, and transparency and data accountability. To support the ethical use of technology, we link the highlighted six key areas and seven ethical principles in a proposed conceptual framework (Figure 7).

The conceptual framework aligns well with the use cases provided in the IEC TS 63134:2020, which posits that the goal of utilizing AAL is to enable older adults to remain active and thrive at home for as long as possible. 37 IEC TS 63134:2020 identifies AAL scenarios and use cases based on real-world applications and requirements. 37 The use cases provide a practical context for considerations of interoperability and standards based on user experience. Use cases provide a context for utilizing existing standards and identifying further standardization work. User requirements have also been identified. This document also highlights potential areas for standardization in the AAL ecosystem to ensure safety, security, privacy, ease of operation, performance and interoperability. The case categories include: (1) prevention and management of chronic long-term conditions; (2) social interaction; (3) mobility; (4) health and wellness; and (5) self-management of daily life activities at home. 37
Discussion
To inform the ethical considerations in the context of AAL technologies for older adults, we discuss the perspectives of the care recipients familiar with AAL technologies gleaned from the academic literature and how their perspectives intersect with the perspectives in the gray literature review and specifically in the CSA Group technical report. 23 Their interaction is illustrated in a flow chart of a proposed conceptual framework in the Synthesis section. One change we will make to the list of categories is replacing Personal thoughts of care recipients on technology use with a governing theme since the genesis of all the themes are the personal thoughts, that is, the perspectives of older adults.
Challenges of independent living
Privacy
The privacy theme is divided into two key subthemes. The first subtheme under privavcy addresses Monitoring Leading to Privacy Intrusion, highlighting how surveillance or monitoring practices can encroach upon personal privacy for example being observed watching TV all day according to one participant from the literature review 25 or being observed returning home at midnight shared another participant from the literature review. 29 The second subtheme explores the Trade-offs Between Privacy and Staying at home, emphasizing the compromises individuals might make when balancing their need for privacy with the conveniences or requirements of remaining in a domestic setting, such as receiving reminders to listen to a good radio program as narrated by a participant from the literature review. 25 Both subthemes illustrate the broader challenges surrounding privacy in monitored environments. A “value trade-off” for an AAL system being acceptable to its users where the benefits must justify any encroachment (real or perceived) on the care recipients’ privacy and AAL technologies use should be completely voluntary and not elicit feelings of being spied on. 23
Availability of behavioral options to cope with challenges
Co-design
The theme of co-design focuses on collaborative processes where multiple stakeholders work together to create solutions. A key subtheme in this context is Involving Elderly in Technology Design. This subtheme highlights the importance of engaging older adults in the design and development of technology, ensuring that their needs, preferences, and challenges are considered. 27 It emphasizes the value of participatory design approaches, where elderly users are active contributors rather than passive care recipients. This leads to more accessible, user-friendly, and meaningful technological solutions that cater specifically to their requirements. 27 Co-design also avoids a One-Size-Fits-All Solution, recognizing and accommodating diverse physical, cognitive, and social needs when promoting technology use thus fostering an Equity in Design ecosystem.
Autonomy
The central theme of Autonomy is broken down into three related subthemes. The first subtheme is Reluctance to Accept Assistive Technologies, highlighting individuals’ hesitation toward adopting technologies designed to help them. 28 The second subtheme addresses External Pressure to Use Technology, which focuses on external influences or coercion to integrate technology into daily life. 28 The third subtheme is Concerns About Intrusiveness, emphasizing worries about how these technologies may invade personal space or limit independence. 26
According to the standard reference document IEC SRD 63416:2023, designers and deployers of AAL devices should respect the autonomy of the care recipients and not, for example, limit care recipients’ movement due to a decline in mental and physical abilities. 34 Likewise, surveillance systems discourage behaviors even if the users may enjoy them to avoid triggering safety concerns. 34 This may remove decision-making about risk or perceived risk-taking behaviors from users since technology is being utilized to risk-manage users’ action and alert caregivers when needed. 34 Also, whenever possible, AAL technology users or the substitute decision makers should be allowed to make decisions on who controls and has oversight their personal health information. 23 Data from AAL technologies should not be used in isolation and independent of the end users. 1 Human dignity should also always be maintained, and the care recipients’ perceptions of being controlled by an AAL system should be addressed expediently. 23
Together, these subthemes illustrate the challenges to autonomy in the context of technology adoption.
Influence of organizations
Stigmatization/Alienation
The theme of Stigmatization/Alienation centers around the feelings of exclusion or marginalization individuals experience, often due to societal biases or differences. The subthemes of Avoiding Unwanted Attention and Not Wanting To Be Different delve into how people navigate this stigma. 25 Avoiding Unwanted Attention reflects the desire to stay unnoticed to prevent judgment or scrutiny, while Not Wanting To Be Different underscores the fear of standing out in ways that might lead to social rejection or being labelled as “other.” In fact, one participant from the literature review contended that if AAL technologies are available, they should be installed in all the apartments of the facility. 25 Additionally, the care recipients felt that the use of assistive technology would portray them as being dependent and in need of monitoring, which they perceived as a weakness. 26
Influence of social networks
Diversity and social inclusion
Under the broad theme of social inclusion are subthemes that focus on fostering connections and belonging in the digital world. It highlights the importance of AAL technologies in Creating Online Social Groups as a key aspect of enabling social inclusion, allowing individuals isolated at home to form communities and support networks virtually as notes by a participant from the literature review through a conference call for neighbors over the age of 70. 29 Additionally, it emphasizes the importance of maintaining connections with the world, according to a care recipient, ensuring that individuals can stay engaged and participate in society, regardless of physical barriers or social isolation. 32
As a counterpoint, it is also important to consider whether the AAL devices overcomplicate rather than simplify tasks for the users, or risk possibly reducing social interactions that they enjoy. 31 For example, adopting an automated pill dispenser when pills were dispensed by a caregiver in the past may result in less contact with that caregiver. 31
The role of the physical environment
Accessibility
The subthemes address Device Usability Issues Due to Physical Limitations as illustrated by a participant from the literature review who had hand tremors which made it difficult to operate a device. 29 Other challenges faced by users with Visual Impairments Impacting Device Use described the writing being too small and having to rely on the screen brightness at the highest setting. 29 Additionally, the care recipients emphasize the importance of Making Technology User-Friendly by making it larger 29 and providing Customizable Features for Accessibility as noted by a participant from the literature review who desired the sound to be captured directly into their hearing aids from the TV. 29 The concept of Unified Device Controls is also highlighted by participants from the literature reviews, pointing to the need for cohesive and standardized controls across devices to improve the overall user experience for individuals with accessibility concerns. 27
Additionally, the lack of inclusion and inequalities in accessing AAL technologies due to economic and social disparities as strong ethical concerns. 23 They should also be able to consistently serve diverse users fairly and without discrimination despite declining cognitive abilities of users. 30
Strengths of the review
First, the review systematically selected studies, ensuring a comprehensive and structured approach that could be replicated by other researchers. This methodology enhances the reliability and thoroughness of the review. The researchers consulted an expert librarian on the best approach to the search strategy, which resulted in the review using three major databases: Scopus, IEEE Xplorer, and PubMed. This comprehensive database search ensured a wide and inclusive capture of relevant studies, enhancing the robustness of the review. The use of the PRISMA-ScR reporting method added credibility to the review process and demonstrated a rigorous and transparent approach to the scoping review process.
Second, this coping review identifies and discusses a broad range of ethical themes pertinent to Active Assisted Living (AAL) technologies for older adults, including informed consent, privacy and data protection, respect for autonomy, accessibility, diversity and inclusion, beneficence, and transparency and accountability. This comprehensive thematic coverage provides a well-rounded understanding of the ethical considerations involved. Also, the review effectively uses findings from a previous study on AAL in the continuum of care for older adults and builds on a recent systematic review, providing a solid foundation and context for the current discussion. Moreover, by integrating the findings of another study on the role of active assisted living in the continuum of care for older adults, 30 this review complements the study by enriching the discussion that did not focus on but alluded to the ethical use of AAL technologies for older adults. Thus, uniquely, the review highlights six key areas related to the ethical use of AAL technologies, including the challenges of independent living, the availability of “behavioral” options to cope with challenges, personal thoughts on technology use, the influence of social networks, the influence of organizations, and the role of the physical environment. This detailed breakdown provides a nuanced understanding of the various factors influencing the ethical use of AAL technologies.
Finally, the review incorporates care recipients’ perspectives, often missing from the systematic reviews, by emphasizing the perspectives of diverse stakeholders, including those working in care delivery, tech developers, tech integrators, and caregivers or their advocates. This important inclusion, coupled with care recipients’ quotes on the ethics of AAL technologies, ensures an authentic voice is disseminated from the care recipients embedded within the ecosystem of AAL technologies.
Limitations of the review
First, the review identified only five relevant articles, a relatively small sample size. Although this limitation may reduce the robustness and generalizability of the conclusions drawn, the five publications used in this review produced a wealth of information, that is, care recipients’ perspectives. Second, three out of the five studies were conducted in the Canada and USA, indicating a slight geographic concentration that might limit the applicability of the findings to other regions. Only two studies were from Europe, and none from the other continents or regions other than Europe and North America. Unfortunately, this geographic skew may not represent global perspectives or outcomes. Second, although there were studies from the 2000s, 2010s, and 2020s, the small number of included studies indicates an incomplete distribution, which could introduce a temporal bias. Third, although the journals’ overarching themes include health, science, and technology, only a few focused, specifically on aging. This thematic diversity might dilute the specificity and depth of insights related to aging since older adults are the primary target population of the review. Fourth, some of our discussions were not as in-depth since the evidence was sparse on the for some of the themes, for example, on transparency and accountability. In the literature, topics under diversity and inclusion are explored in the context of older adults and AAL technology 38 and transparency and accountability within power dynamics with regards to technology and IoT use. 39 Fifth, the identified studies were published in journals with varying impact factors, ranging from 1.9 to 4.8. This range suggests a potential for publication bias, as higher impact factor journals anecdotally tend to publish studies with more significant or positive findings. However, since we implemented the best practices of conducting a scoping review, that is, we adhered to the review protocol, we could not include all qualitative studies in the period (2000–2023) without breaking the bounds of the inclusion and exclusion criteria cited in the text.
Conclusion
This scoping review aimed to synthesize current knowledge of the ethical use of AAL technologies in aging in place contexts. The scoping review collated existing knowledge and integrated a conceptual framework by using the case categories from the gray literature and emerging themes from our scoping review.
According to the perspectives generated in this scoping review, our findings suggest that:
Co-design is the main motivator for early adoption of AAL smart technologies; The less intrusive the technology is to the care recipients, the more tolerable/acceptable it becomes. The less cumbersome the technologies are to use, that is, the more user-friendly and accessible and inclusive they are in design, the less inhibited the care recipients are from trying these AAL smart technologies. Finally, for care recipients who struggle with behavioral changes as part of their treatment plan and may not be as responsive to an in-person caregiving ecosystem that encourages them to reach their health goals, automated tracking appears to be a motivating factor to succeed.
There is some willingness for older adults to include wearables and IoTs in their AAL smart technologies ecosystem, but it is contingent on a safe, secure, and private (unintrusive) monitoring system. This scoping review has the potential to offer valuable insights to various stakeholders, including developers, designers, health policymakers, providers, patients, researchers, and health insurance companies. However, further research is needed to close the gap in regulatory instruments and to include propose best practices in upholding the respect for older adults’ voices in the use of technology. 25 Also, a bioethical approach to assessing AAL technologies would help underpin any historical and future analysis.
Recommendations for guidelines and standards are as follows:
How can society best to protect the human rights of users? How can society best structure data governance? How can society ensure equity of access and accuracy of data? How can society enforce ethical policies in the use of AI? How can society ensure older adults receive informed consent on the use of personal data?
Governance requirements by policymakers and regulators should ensure that the data collected by AAL technologies are kept safe, secure, and confidential, while providing the intended benefits to seniors should be a priority. Care recipients and their caregivers should be fully informed of how AAL technologies work, the benefits for them, as well as of their own rights to choose and refuse the technology as desired.
Ensuring that the developers provide informed consent and are comfortable with digital monitoring and activity surveillance. Ensuring that the developers of devices do not overcomplicate tasks or reduce social contact that is enjoyed. The basic ethical principles that should guide designers and developers when the use of audio- and video-based technologies for AAL and its incorporation into a wide range of applications, most notably healthcare-related ones, include:
Beneficence: the doing of charitable deeds with no specified limitation. Non-maleficence: the avoidance of harm and requiring a risk/benefit analysis. Respect for autonomy: the recognition that an individual can make their own choices and understand the consequences of these choices. Confidentiality: the maintenance and protection of personal details and information that may reveal personal details.
Footnotes
Acknowledgments
The authors thank the CSA Group for providing pertinent insights.
ORCID iDs
Author contributions/CRediT
THP led the project and drafted the first manuscript, THP and GM conducted the abstract screening, GBN resolved any conflicts emerging in the abstract screening, THP, GBN, and SA conducted the full text screening, IM and DC co-drafted sections of the first manuscript, PPM conceptualized the project and THP, IM, SA, GBN, DC, and PPM reviewed the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Mitacs and the CSA Group [IT24763].
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Other statements
The grant number might compromise online anonymity.
Appendix
Gray literature review results.

| Authors (Year) | Title | Aims | Document type | Ethical considerations | Guidelines/Standards |
|---|---|---|---|---|---|
| IEC SRD 63416:2023 33 | Ethical considerations of artificial intelligence (AI) when applied in the active assisted living (AAL) context. | This document describes ethical considerations relevant when developing AAL systems and services and analyses whether existing frameworks for the governance of AI sufficiently meet the needs of AAL care recipients. | Systems Development Reference | Ethical considerations for AAL technologies include: Respect for autonomy: potential movement or other actions of the AAL care recipient should not be limited due to a decline in abilities. Diversity, non-discrimination, and fairness: decisions and actions should be consistent for all users. Languages used in cueing shall be culturally sensitive. Data privacy: Who should have access to care recipient's data and to what extent this data should be utilized should be considered. Safety: When and under what conditions should the AI system act to minimize danger/increase safety of the care recipients. Human dignity, oversight, and control: individual user, if capable, or the monitoring clinician, should decide who can access recipient's personal health information. AI system should not take actions without the approval of the person overseeing the system and the user should not perceive themselves as being “under the control of” the AI system at any point. |
Standards for AAL implementation should focus on answering these questions for the user.
- How to protect the human rights of users - How to structure data governance - How to ensure equity and accuracy - How to enforce ethical policies in the use of AI - How to ensure informed consent on the use of personal data |
| Alzheimer's society (2015) 30 | Assistive technology devices to help with everyday living - Factsheet | This factsheet looks at some of the devices and technologies that can make getting on with life easier for people living with dementia and their carers. It also suggests ethical considerations pertaining to the use of these devices. | Alzheimer's Society Factsheet | Assistive devices should be primarily for the benefit of the person with dementia—to enhance their independence, safety, and daily living. They should not pose a threat to privacy. Consent should always be obtained before use of AAL technology. |
When choosing to use assistive technology and selecting the systems or devices to use, the person with dementia must be involved in any decisions, and their consent must be sought and gained wherever possible. If the person lacks the ability to make decisions for themselves (‘capacity’), decisions need to be made in the person's best interests and must also be the least restrictive option. |
| Age Space (2024) 31 | Assistive technology for the elderly: A guide to getting started. | The guide discusses the distinct types of assistive technology available for the elderly and the ethical considerations with assistive technology for the elderly. | Age Space Guide | Some people will be worried about their privacy or feel uncomfortable with the idea of digital monitoring and activity surveillance. Other important questions to ask when it comes to assistive devices are whether they overcomplicate the task they are trying to simplify for the elderly individual and whether they reduce enjoyable social contact. |
Best practices for AAL use in recipients include: - ensuring that the users provide informed consent and are comfortable with digital monitoring and activity surveillance. -ensuring that the devices do not overcomplicate tasks or reduce social contact that is enjoyed. |
| Sixsmith et al. (2023) 34 | AgeTech, ethics and equity; Toward a cultural shift in AgeTech ethical responsibility | The project aims to investigate ethical concerns in AgeTech design, research, and development, as well as the larger cultural shift required for ethical and equitable AgeTech services for older persons and their caregivers. | AGE-WELL project report | Ethical issues to be considered in AgeTech include autonomy, informed consent, data protection and data privacy issues to ensure trust by users. | AgeTech users should receive adequate information and understanding of AAL technology development process while making certain that the needs of diverse users are considered in the setup of these systems. It is also important to address how users consent to and understand these devices, as well as how their’ data is utilized. |
| Bin Noon et al. (2022)23 | Data governance for active assisted living | This research report explores the integration of AAL technologies and data into the continuum of care. In addition, it maps data access and governance for AAL technologies, providing guidance on how to implement these solutions in the Canadian context, while protecting the privacy and well-being of seniors using AAL technologies. | CSA Group Technical Report | AAL technology use should consider how the data is used to ensure direct benefit to the care recipient without monetization of users’ data. There should be a “value trade-off” where, for an AAL system to be acceptable to its users, the benefits must justify any encroachment (real or perceived) on the care recipients’ privacy. AAL use should be completely voluntary and not elicit feelings of being spied on. |
There is need for greater consistency in language and technology requirements across Canada. There should be better role definition regarding who may have access to the data, who is responsible for acting based on the gathered data, and the recognition of the privacy– utility trade-off inherent in using AAL technologies in care settings. Governance requirements for ensuring the data collected by AAL technologies are kept safe, secure, and confidential, while providing the intended benefits to seniors should be a priority. Care recipients should be fully informed of how AAL technologies work, the benefits for them, as well as of their own rights to choose and refuse the technology as desired. |
| Clark et al. (2023) 32 | Technologies to increase freedom for people living with Dementia. | This report focuses on assistive technologies that encourage people with dementia to live in their homes and communities for longer. | Canadian Journal of Health Technology Report | Ethical considerations to be considered when using AAL technologies include equitable access, privacy, and data ownership standards. | Data ownership and privacy should be prioritized by using an opt-in approach to data sharing rather than opt-out. Ensure the information collected does not contain any overly personal details. |
| Ake-Kob et al. (2021) 35 | State of the art on ethical, legal, and social issues linked to audio-and video- based AAL solutions [CA 19121 WG 1] | The report aims to define and examine relevant ethical issues associated with audio- and video-based monitoring and to propose privacy-aware working solutions for assisted living. | European Cooperation in Science & Technology white paper | AAL technology may create opportunities for violating informational privacy. Older users may experience feelings of frailty when devices and sensors are publicly visible as they indicate illness or a need for monitoring. There are inadequate inclusion and inequalities in access to AAL technologies. |
The basic ethical principles that should guide the use of audio- and video-based technologies for AAL and its incorporation into a wide range of applications, most notably healthcare-related ones, include: Beneficence: the doing of charitable deeds with no specified limitation. Non-maleficence: the avoidance of harm and requiring a risk/benefit analysis. Respect for autonomy: the recognition that an individual can make their own choices and understand the consequences of these choices. Confidentiality: the maintenance and protection of personal details and information that may reveal personal details. In addition, AAL devices should consider the concepts of justice and equitable resource allocation, protection of vulnerable users, and provision of comprehensive, accurate, and sufficient information for informed consent. |