
Abstract
Robotics not only contributes to the invention of rehabilitation devices, it can also enhance the quality of medical education. In recent years, the use of patient simulators and part-task trainers in the medical education field has brought meaningful improvements in the training of medical practitioners. Nevertheless, in the context of therapy training for upper limb disorders, trainee therapists still have to engage directly with the patients to gain experience of the rehabilitation of physical diseases. In this work, a high-fidelity part-task trainer that is able to reproduce the stiffness of spasticity and rigidity symptoms of the upper limb, such as those observed in post-stroke patients and Parkinson's disease patients, has been developed. Based on the evaluation carried out by two experienced therapists, the developed part-task trainer is able to simulate different patient cases and help trainee therapists gain pre-clinical experience in a safe and intuitive learning environment.
Introduction
Simulation in Medical Education
A simulator in medical education is a computer-controlled human mannequin or set of parts of the human body that is able to function as the human anatomy and react to clinical procedures used during the training of doctors, surgeons, nurses and therapists. A part-task trainer simulates different situations and helps the trainees learn from new experiences and acquire new clinical skills. Simulators of segments of the human body are called part-task trainers, while a simulator that can provide complete human physiological responses is called a patient simulator [1].
Although simulators have only recently been applied in the education of medical practitioners [2][3], the simulator approach has been applied in educating trainee pilots to fly airplanes safely for decades [4] and has helped in veterinary clinical training as well [5]. Teaching and learning in the clinical field might involve many challenges when it deals with real human or animal patients, and a simulator can be used until the students master the clinical training, thus avoiding the occurrences of clinical mistakes.
There are patient simulators that have been used in clinical training to improve performances and skills in surgery [6] and anaesthetics, and some have been proven to develop good team performance even in complex fields such as trauma resuscitation [7]. The use of advanced human patient simulators encourages the team to practice high-risk skills in a risk-free environment. There are other haptic simulators for surgery under development, such as for angioplasty intervention [8] and for virtual material [9].
However, in therapy training, trainees still engage directly with patients to gain experiences. A high-fidelity human patient simulator that is capable of helping them improve their skills and performance such as in [10] and [11] is lacking. In order to be an expert in physical therapy and occupational therapy, therapists need to have a multidimensional knowledge base, in which one of the concepts of therapy skills is the use of touch [12].
In this paper, the focus is on developing an artificial human upper limb for the purpose of pre-clinical therapy education similar to the added value in the application of the infant respiratory physiotherapy described in [13].
Motivation
The need for a high-fidelity part-task trainer that can provide different patient cases and the opportunity to have physical contact with ‘patients’ in a safe and encouraging environment is described as follows:
Patient safety – Physical and occupational therapists play an important role in resuming the normal daily life of patients with regard to their physical impairments. It is understood that clinicians in training will treat patients; however, from an ethical perspective, harm to patients as a by-product of the training or of lack of experience is justified only after maximizing approaches that do not put patients at risk [14]. In the rehabilitation field, patients are indirectly becoming part of the learning process of gaining experience, as distinct from role-play training. This is no longer acceptable, as it will risk the patient's safety. The deployment of simulators is a suitable method to provide a patient-free environment for therapy students.
Patient availability – The burgeoning number of physiotherapy schools has reduced the opportunities for trainee therapists to find training subjects. This has raised concerns in the profession that the constrained health care sector cannot continue to deliver an appropriate level of experience to graduates [15]. A high-fidelity simulator plays an important role in reproducing these conditions and providing clinical experience in a patient-free environment.
Standardization in evaluation – Providing a consistent replication of symptoms will help to create a standardized evaluation method, thus improving the trainee's skills. Currently, therapists evaluate the severity level of spasticity using the Tardieu, Ashworth and Modified Ashworth Scales, which can vary depending on their experience. Variability in the rater scores that currently happens between raters and within raters suggests that training can be improved.
Paradigm shift in medical education – Current medical education demands better measurement of outcomes and accountability of the diagnosis from the medical and nursing team, and from other healthcare practitioners. This will lead to improvements in the educational practices and curricula, providing new challenges to the curriculum planners. Those who responsible for health professional education finds that traditional educational models, involving extensive clinical time, are not sustainable. Also, health organizations, health managers and clinicians reportedly view students on clinical placement as a burden [16]. With an increasing number of students requiring training, the physical therapy profession is not immune to these challenges and has stated widely that there is a ‘clinical education crisis'. Therefore, curriculum planners need to suggest new education methods. For instance, the Health Workforce Australia National Simulated Learning Project reported that 15 of the 16 universities frequently use a Simulated Learning Programme (SLP) during their pre-clinical programmes. This emphasizes the importance of using simulation to help trainee therapists gain experience.
The Upper Limb and Upper Limb Disorder
The upper limb is made up of three parts that define its structure. These parts are the upper arm, the forearm and the wrist or hand. The muscles of the upper arm can be split into anterior and posterior compartments. The anterior compartment muscles are responsible for the flexion of the forearm. Likewise, the posterior compartment extends the forearm. The upper arm and the forearm are connected at the elbow, where the mechanism is similar to a hinge joint. The radius bone that connects the elbow and the wrist creates the wrist extension effect. Wrist extension occurs when nerve impulses are sent from the brain to the radial nerve, which innervates a group of extensor muscles. The muscles then contract to pull tendons and produce joint movement.
There are various upper limb disorders that require rehabilitation, such as spasticity, rigidity and contracture. Upper limb disorder is a condition that affects the shoulder, upper arm, elbow, forearm and hand. It is not a specific disease but varies with different symptoms such as post-stroke and Parkinson's disease symptoms. It might also occur due to work-related movements. In this paper, work was conducted on emulating two symptoms by means of a high-fidelity part-task trainer.
Spasticity commonly occurs in patients with spinal cord injury, multiple sclerosis, cerebral palsy or stroke. Spasticity will affect daily activities, causing pain and discomfort and might lead to sleep disturbance which will eventually burden the caregivers. Spasticity is a unidirectional, velocity-dependent symptom and varies with the muscle tone amplitude [17]. Muscle resistance increases with passive movement and can be assessed by fast flexion or extension of the forearm.
On the other hand, rigidity is a bi-directional symptom which is not affected by velocity. Rigidity or stiffness of the muscle can be seen in Parkinson's disease, where the patient's muscles are always tensed and are not able to loosen up. A relatively uniform rigidity is called lead-pipe rigidity, whilst trembling, ratchet-like movements are called cogwheel rigidity. Patients with rigidity exhibit shaking and have slow movement feedback. Rigidity also shares the same effect as spasticity, that is, sooner or later it will develop into emotional and cognitive problems.
Development of Part-task Trainer
Measurement of Wrist Extension Effect
Prior to prototype development, a measurement was conducted to prove the effects of wrist extension caused by the extensor muscles. The objective of the measurement is to provide evidence that the length of the forearm changes in a full flexion position and a full extension position.
One healthy subject was used in the measurement. The length of the subject's forearm during full flexion was measured, and the measurement of the length was recorded for different angles of the elbow joint towards the full extension position. Three trials were conducted. The result of the wrist extension tracking experiment is shown in Figure 1, where the forearm moves in an elliptic trajectory instead of a circular trajectory. The length of

Ellipse orbit of wrist extension effect
This section focuses on the development of the core structure of the human arm for the second prototype. In comparison with the first prototype, the current prototype is able to produce the movement of the elbow joint with pronation and supination movements [21]. These movements are important in rehabilitation and therapy education.
As shown in Figure 2, the artificial human arm is built from the shoulder area with a range of motion of −45 degrees to +45 degrees from a horizontal plane. By providing a range of angles, trainee therapists may take various positions depending on the different positions of the patient. The forearm is built with a 140-degree range of motion, imitating the human forearm's movement.

Range of motion for artificial human arm simulator
The fabricated part-task trainer is supported with two shafts, the shoulder shaft and the elbow joint shaft. The details of each segment are described below.
The elbow joint is supported by the humerus. The humerus is built with two plates, both on the sides, to support the elbow joint, which is the most important structure in reproducing the disorder symptoms.
In order to produce the ellipse movement shown in Figure 1, the elbow is built with a cam-shaped mechanical structure and the ulna bone attached to the cam follower will move following the cam's ellipse orbit. Figure 3 shows the details of the cam and the position of the ulna bone attached to the cam follower.
The stiffness of the symptoms is reproduced at the elbow joint by providing resistance when therapists apply extension movements to the part-task trainer. Referring to Figure 2, the shaft of the elbow joint is connected to the shoulder shaft using a cantilever mechanism of a belt and pulley. The actuators that transfer the force to the shoulder shaft and the belt that transfers the force to the elbow joint shaft are placed between the two humerus plates.

Cam follower at the elbow joint
The forearm is built with separate ulna and radius bones attached to the elbow joint shaft. Figure 4 illustrates the cross-sectional drawing of the ulna bone and the radius bone. Each bone performs a different function.
The radius bone is built with the ability to perform pronation and supination movements. With the aim of providing these movements, a ball joint spherical bearing is used. The ball joint spherical bearing is able to create 30 degrees of angular displacement. A healthy human requires 50 degrees of pronation and 50 degrees of supination movements to accomplish daily activities [22]. In rehabilitation, the imitation of 30 degrees of pronation and supination movements has already met the requirements of therapists.
On the other hand, the ulna bone is built with a mechanical spring structure to allow for movement following the ellipse cam, as explained in the ‘Elbow Joint’ section. The ulna bone is separated into two parts; the fixed and moveable ulna. The spring attaches the fixed ulna bone on the inside with the moveable ulna bone on the outside, giving the outside ulna bone the ability to move freely following the cam shape in one degree of freedom. This is to enable the mechanism of a cam follower to facilitate the ellipse movement of the forearm, generating the effect of a wrist extension.

Moveable ulna structure and radius angle movement
The part-task trainer system is built with a set of DC servo motor manufactured by SANYO Corp. (L404-011NE) and a Magneto-Rheological (MR) brake by LORD Corp. (RD-2087-01) to reproduce the stiffness as in the elbow of a patient suffering from an upper limb disorder. An MR brake is an electronic brake control system that employs the brake-by-wire system which is currently endorsed by the automotive industry [23]. The MR brake has a faster response compared to other hydraulic brake systems. In this system, it is used to produce resistance, imitating the stiffness of a patient for the trainee therapist.
In the current stage, the part-task trainer is built to reproduce the symptoms of spasticity and rigidity. For constant stiffness, the MR brake is used to reproduce the resistance and the DC servo motor is used to support the stiffness provided by the MR brake, depending on the symptom's characteristics. Details of the symptoms are described in section 3: ‘Symptoms Reproduction'.
The passive force produced by the MR brake and the DC servo motor is transmitted to the elbow joint using a belt and pulley as a cantilever mechanism to provide resistance following the symptoms of the upper limb disorder. The passive force is activated based on the elbow rotation angle, which is measured by a rotary encoder. A strain gauge is placed at the shoulder shaft to detect the force exerted by the simulator for the purposes of analysis. The configuration of the system is illustrated in Figure 5.

Actuator and sensor configuration for part-task trainer
The radius and ulna bones, as well as the upper arm part are rolled with urethane foam that replicates the human arm's softness. Then, both the forearm and upper arm are covered with a thin simulated skin made from silicone material. The simulated skin is used to reduce the incongruity when interacting with the part-task trainer. The simulated skin cover is presented in Figure 5.
Symptoms Reproduction
Symptoms Quantification
In order to reproduce the symptoms of an upper limb disorder in the part-task trainer, a database set for each symptom has to be developed. With the help of two experienced therapists, the characteristics of the symptoms were measured, with one of the therapists as a simulated patient and another therapist giving rehabilitation treatment. A muscle tester (μTAS MT-1) with a load cell range of 0-100 [kg] produced by ANIMA Corp. was attached to the therapist to measure the force exerted by the patient.
Three markers were attached to the patient's shoulder, elbow joint and wrist to measure the elbow joint angle. One marker was attached to the back hand of the therapist, holding the muscle tester to measure the distance of the force from the patient's elbow joint to produce the moment around the elbow joint later. The positions of the markers are shown in Figure 6. All rehabilitation sequences were recorded and analysed with Frame-DIAS. Frame-DIAS is an image processing LED marker detection device developed previously in our laboratory.

Markers showing key points of forearm movement
The three symptoms measured were spasticity, lead-pipe rigidity and cogwheel rigidity. The characteristics of spasticity, lead-pipe rigidity and cogwheel rigidity are shown in Figures 8(a), 8(b) and 8(c), respectively. The graphs show one cycle from a full flexion to a full extension movement of the simulated patient. Apart from the explained method, there are several methods under study of how to quantify the characteristics of upper limb diseases [24], other than the Ashworth Scale [25].
Spasticity is a velocity-dependent symptom with an increase in muscle tone in response to stretching relaxed muscles [17], and can usually be seen in post-stroke patients. It must be assessed with a quick flexion or extension of the elbow, or with a quick pronation and supination of the forearm. Therefore, spasticity symptoms show the characteristics of a high magnitude of moment called muscle tone around the elbow axis during sudden extension movements, as in Figure 7a. The simulated patient shows resistance from a fully flexion condition (140 degrees) until 100 degrees and reduces its resistance depending on the degree of the elbow joint.
Meanwhile, rigidity symptoms are not velocity dependent, and can be seen in Parkinson's patients. Lead-pipe rigidity is a continuous resistance during passive movements from full flexion up to full extension (140 degrees - 0 degree), and ends with a sudden release of the muscle stretch [26]. The characteristics show a sudden decrease in the moment around the elbow axis, as in Figure 7b. Cogwheel rigidity shows the same characteristic patterns as spasticity symptoms, with a high magnitude of moment during full flexion (140 degrees) and reduces its resistance depending on the elbow joint degree along with ratchet-like resistance during the whole cycle of extension movement, giving symptoms of trembling as seen in Parkinson's disease patients [26]. Characteristics of the symptoms can be seen in Figure 7c.
The database is made up of simulated patient data, thus it shows the general characteristics of each symptom without focusing on the symptom level based on the Modified Ashworth Scale or Tardieu Scale.

Spasticity characteristics

Lead-pipe rigidity characteristics

Cogwheel rigidity characteristics
Unlike the other upper limb disorder simulators [27][28], the stiffness of each spasticity and rigidity symptom in this work is reproduced using two different types of actuators, the MR brake and the DC motor. Each symptom is built with a different programming, as described in Figures 9, 10 and 11.
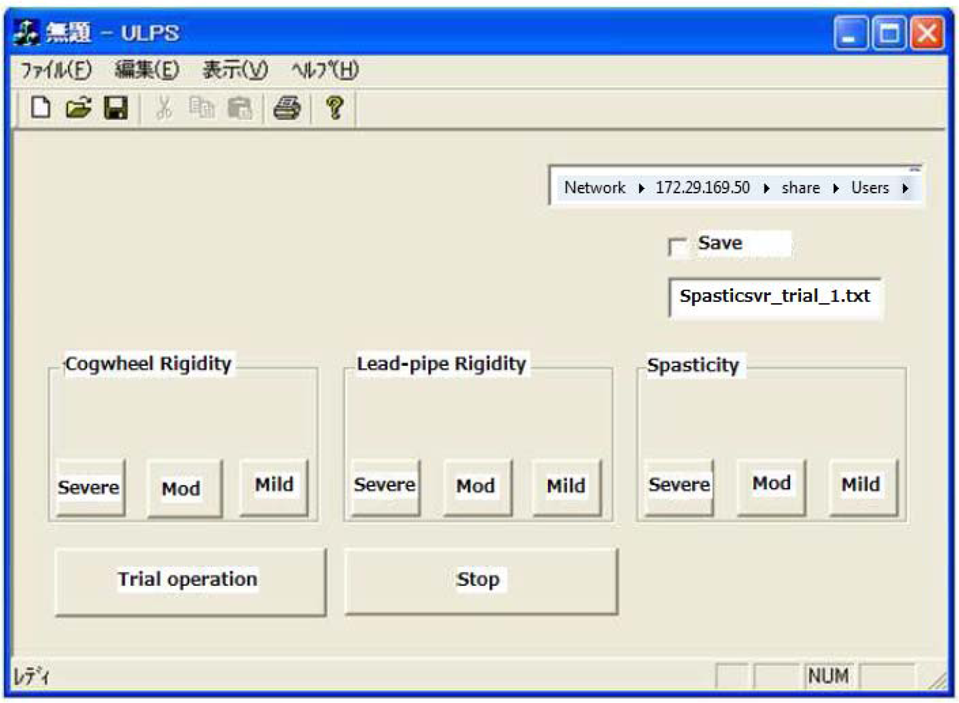
Part-task trainer graphical user interface
The system starts with the part-task trainer being in full flex position, thus showing 140 degrees of the elbow joint angle. The therapist needs to select a symptom from a graphical user interface, as illustrated in Figure 8. There are three choices: spasticity, lead-pipe rigidity or cogwheel rigidity. Each symptom provides a different stiffness following their respective characteristics, as described in Section 3.1. Therefore, a different actuator is activated at a different elbow joint angle. Each symptom is divided into three levels: severe, moderate and mild. Each level is still under development, thus the results shown in this paper are the emulation characteristics of each symptom in general.
Figure 9 shows a flowchart for programming the part-task trainer for the emulation of spasticity symptoms. The elbow joint angle is divided into three phases, from full flexion to full extension positions. In the range of 140–101 degrees of the elbow joint angle, the system provides maximum resistance using only the MR brake. This range of the elbow joint angle shows the muscle tone phenomenon. After entering the range of 100–41 degrees of the elbow joint angle, the resistance from the MR brake and the DC motor is reduced depending on each angle. Finally, when the elbow joint angle is almost in the full extension position, a constant resistance is imposed by the MR brake and the DC motor. In order to repeat the training, the part-task trainer needs to be returned to the fully flexed position.

Flowchart for emulation of spasticity
Figure 10 shows a flowchart for programming the part-task trainer for the emulation of lead-pipe rigidity symptoms. The elbow joint angle is expressed in only one phase. Unlike the spasticity symptom, lead-pipe rigidity shows a uniformly constant resistance characteristic. Therefore, the system only provides a constant MR brake output voltage to recreate uniform resistance regardless of the detected elbow joint angle.

Flowchart for emulation of lead-pipe rigidity
Figure 11 shows a flowchart for programming the part-task trainer for the emulation of cogwheel rigidity symptoms. Cogwheel rigidity is one of the rigidity symptoms that can be seen in Parkinsonism. This symptom has three phases of elbow joint angles, similar to the spasticity symptom, except that it has an additional ratchet-like movement imitating the trembling and shaking symptoms. As shown in Figure 11, the muscle tone of the cogwheel rigidity is reproduced at 140–102 degrees of the elbow joint angle. The computer sends an output voltage to the MR brake and this output voltage is reduced during the range of 101–48 degrees of the elbow joint angle, depending on each angle detected. The most important part in imitating this symptom is producing the ratchet-like movement. The DC motor supports this movement by inserting a torque at two degrees intermittently. In the first phase, the inserted torque is larger in comparison to the second phase of the elbow joint angle. During the final phase before reaching the full extension position, 0.2 [V] output of the DC motor is inserted with zero voltage of the MR brake output.

Flowchart for emulation of cogwheel rigidity
Using the developed upper limb part-task trainer, an evaluation is conducted on the reproduced symptoms of the upper limb disorder. Two experienced therapists evaluated the system. The evaluation session is shown in Figure 12. The force given to the part-task trainer is detected by a strain gauge positioned at the shoulder shaft of the part-task trainer, while the rotation of the elbow joint angle is recorded by the encoder.

System evaluation
The objective of this evaluation is to be able to recognize each symptom's stiffness characteristics emulated by the part-task trainer and compare it with the simulated patient data. Apart from analysing the quantification data of the symptoms, the advice from therapists regarding the differences between the patients’ symptoms was recorded for future development. The therapists were not restricted to any specific positions during evaluation, thus they were not able to exert identical forces and velocities during a trial, which naturally led to different results during each trial.
Figure 13a shows the characteristics of spasticity symptoms showing an increased moment around the elbow joint, especially during 120 degrees of the elbow joint angle. Although a time delay can be observed in the elbow extension movement before reaching the peak magnitude expressing the muscle tone phenomenon, the therapist feels that it does not affect the training, since the important point here is the way the simulator loosens its stiffness after the muscle tone phenomenon.
Figure 13b shows the characteristics of lead-pipe rigidity with continuous resistance following passive movements from the therapist and a sudden release of muscle. Compared to the characteristics shown in Figure 7b, the lead-pipe rigidity symptoms reproduced by the part-task trainer showed similar symptoms with almost the same magnitude of moment.
The cogwheel rigidity symptoms reproduced by the part-task trainer are shown in Figure 13c, where ratchet-like movements can be observed during the extension of the forearm. The symptoms are quite similar to spasticity symptoms, where the patients show the effects of muscle tone along with trembling or shaking movements. Compared to the result in Figure 7c, the part-task trainer reproduces an extreme trembling symptom. For actual patients, the trembling is much more moderate in comparison to the part-task trainer. The trembling movement is the result of motor input assistance to the MR brake at two degrees intermittently. However, the torque given was too large, at 2 [N] on average, while in the simulated patient the trembling torque was recorded at 0.5 [N], causing the forearm of the part-task trainer to vibrate intensely. Thus, an improvement in the algorithm is needed for the cogwheel rigidity symptoms.

Reproduced spasticity

Reproduced lead-pipe rigidity

Reproduced cogwheel rigidity
Furthermore, several comments regarding the simulated skin cover were obtained from the therapists. The use of urethane foam to simulate human arm softness has to be improved, as the stiffness of human skin is higher than that of urethane foam. In contrast, the simulated skin cover was highly evaluated by the therapists as it is able to provide the feel of interacting with a human arm instead of interacting with a robotic arm. Nevertheless, the training is not affected by the softness and stiffness of the part-task trainer's skin.
The deployment of a high-fidelity part-task trainer for therapy education on upper limb disorders enables students to conduct repeated practices, gain experience and build up their confidence before engaging with real patients. The standardization of the symptoms’ evaluation helps in building better clinical judgment, particularly concerning spasticity, lead-pipe rigidity and cogwheel rigidity. Further, it ensures patient safety during training. With the increasing number of medical schools and therapy training centres, it solves the problem of patient unavailability and the difficulty in obtaining patient cooperation for the training of students.
Footnotes
6.
The authors thank the Research Organization for Advanced Engineering at Shibaura Institute of Technology, Japan, the Ministry of Science, Technology and Innovation Malaysia [100-RMI/SF 16/6/2 (3/2014)] and the Ministry of Education Malaysia [600-RMI/FRGS 5/3 (77/2014)] for funding the research work.