
Abstract
Objectives
The aim of this study was to evaluate the safety and efficacy of the artificial urinary sphincter ZSI 375 device in male patients with stress urinary incontinence (SUI) at 10 centres.
Methods
This was a retrospective, nonrandomised, multicentre study. From January 2012 to December 2014, and follow-up to February 2016, men with SUI were treated with the ZSI 375 device. The primary outcome was continence. The secondary outcome was complications rate.
Results
A total of 147 patients with moderate-to-severe stress incontinence and mean age of 70.67 (26-85) years underwent implantation of the ZSI 375 device at 10 centres.
The most common indication for placement was incontinence after radical prostatectomy (121 patients: 82.31%). The ZSI 375 device was considered successful in 86.40% of cases after 12 months follow-up, 83.52% after 24 months follow-up and 78.26% after 36 months follow-up. The infection rate was 6.12%, urethral erosion was 12.92% and mechanical failure was limited to 3.40% leading to ZSI 375 improvement.
Conclusions
This study confirmed safety and efficacy of ZSI 375 device to treat moderate-to-severe SUI in men.
Introduction
The Bradley-Scott artificial urinary sphincters (AUS) is the standard treatment for persistent moderate-to-severe stress urinary incontinence (SUI) since 1973 (1-3). Its first version has evolved into the current AMS 800 (Boston Scientific, USA), but the device has never been modified since 1983. The AMS 800 is still provided in several boxes and separated components to assemble during the procedure with a constraining preparation; the cuff is moulded flat with a potential for creasing and fracture as fitted around the urethra. There is an inability to readjust the cuff in case of postoperative urethral atrophy (4, 5) and no option to adjust the issued pressure of the device after activation. Although many studies have reported a good, long-term clinical outcome (6-8), the procedure can be complex. The double cuff did not show any evidence of improvement on continence but increased complications rate (9). Adopted by many surgeons, peno-scrotal approach does not show any superiority on perineal approach (10). The AMS 800 stays the Gold Standard but presents relatively high surgical revision rates up to 30% (11) with urethral erosion or atrophy, infection and mechanical failures such as leaking connectors and porosity of the Pressure-Regulating Balloon (12, 13).
ZSI 375 (Zephyr Surgical Implants, Geneva, Switzerland) is a one-piece AUS including a number of innovative features to answer AMS 800 lacks. This paper describes safety and efficacy of ZSI 375 implanted at 10 centres, in a group of 147 male patients with SUI.
Patients and Methods
This was a retrospective, nonrandomised, multicentre study open to patients over the age of 18 years with urodynamically proven stress incontinence. The pre-implantation evaluation comprised a patient's history, analysis of voiding diaries [time and voided volumes, number of pads used, urinary incontinence (UI) episodes], a clinical examination, cystoscopy and an urodynamic assessment. The main exclusion criteria for the investigation were detrusor overactivity, urinary tract infection and urethral stricture. Only patients with moderate incontinence (three pads per day) or severe incontinence (four pads or more per day) were included in the study. The Device ZSI 375 AUS is manufactured as a single unit from medical-grade silicone rubber to facilitate implantation and minimise mechanical failures that range from 8 to 45% with AMS 800 (14, 30) (Fig. 1).

Photograph of the ZSI 375 AUS.
One-piece AUS reduce failure of leaking connectors and decrease preparation time. Cuff is adjustable from 3.75 to 6 cm. It is moulded and curved to reduce potential for creasing and fracture (15) (Fig. 2).

Photograph of the ZSI 375 Cuff with a curve design.
Cuff and Pump-Unit are connected via kink-resistant tubing. Pump-Unit (Pressure-Regulating Tank + Pump) is placed in the scrotum. The size of this Pump-Unit is equivalent to the size of a penile implant pump: length 40 mm, diameter 24 mm. The AUS must be filled with saline solution prior to implantation. As there is no abdominal reservoir, the risk of damage to either the bladder or to the intestine is minimised and hence the operating time is reduced.
After activation, the issued pressure can be increased or decreased to improve patient continence via a trans-scrotal approach under local anaesthesia. One millilitre of saline is injected via increased pressure by approximately 10 cmH2O.
Surgical Technique
Implantation of the device was performed as described by Staerman et al (16). The surgical procedure was performed under general anaesthesia, and patients were placed in the lithotomy position with a 16 F Foley catheter in the urethra for guidance. The urethra was exposed through a perineal incision for adjustable cuff placement and an inguinal incision for Pump-Unit scrotal placement. A 12F Foley catheter was inserted at the end of the procedure and removed 24 hours after the procedure. Patients were discharged as soon as they could empty their bladder. The device was activated 8 weeks later in an outpatient setting. During the procedure, the sphincter closure pressure set ranged from 60 to 70, from 70 to 80 or from 90 to 100 cmH2O.
Assessment of Postoperative Continence
The patients were assessed at AUS activation, and at 3, 6 and 12 months and annually. The assessment included scrotal comfort evaluation, clinical examination, urinalysis and bladder ultrasonography to evaluate residual urine volume. Patient incontinence was evaluated with number of pads used per day during a period of 7 days before their follow-up visits. Trans-scrotal adjustment of AUS-issued pressure was done to reach an improvement or a social continence. Social continence was defined as zero pad to one pad per day (with total continence: 0 pad per day) and incontinence as the use of more than one pad per day. Patients were considered as improved if they used both less than two pads per day and 50% fewer pads than at baseline. Success was defined as patient with social continence or improved.
Results
One hundred forty-seven male patients were implanted with the ZSI 375 AUS at 10 centres in Germany, Poland, Italy, Spain, England, Colombia, from January 2012 to December 2014, and follow-up till February 2016. All patients had sterile urine at the time of surgery. Mean age was 70.67 (26-85) years. All patients were incontinent more than 1 year before implantation. Seventeen patients (11.56%) had moderate incontinence and 130 patients (88.44%) suffered from severe incontinence. None of the patients included in the study had detrusor overactivity or urethral or vesico-urethral anastomotic stricture. The most common indication for placement of the AUS was incontinence after radical prostatectomy (121 patients: 82.31%), radiotherapy (nine patients: 6.12%), radical prostatectomy with adjuvant radiotherapy (five patients: 3.40%) and transurethral resection of the prostate (TURP) (six patients: 4.08%). The other causes of incontinence included radical cystectomy with neo-bladder (two patients: 1.36%), Arnold-Chiari syndrome (one patient: 0.68%), Rectal surgery: (one patient: 0.68%), high-intensity focused ultrasound (HIFU) (one patient: 0.68%) and a patient after pelvic traumatism (0.68%). All patients had tried conservative treatment methods unsuccessfully. A total of 11 patients (7.48%) had experienced failure of previous continence procedures or devices, including one patient with Pro-ACT, three patients with AMS 800 (double cuff erosion), two patients with Flow-Secure mechanical failure, two bulking agent injections, three male TOT and two patients following male TOT with bulking agent injection. All previous devices such as Pro-ACT, AMS 800 and Flow-Secure were explanted at least 6 months before implantation of the ZSI 375 AUS.
There were no intraoperative complications. Mean stay was 3 days and patients were discharged after the ability to empty the bladder. No patient experienced bladder overactivity, chronic urinary retention or any other adverse effect following the device activation. ZSI 375 pump is bigger than AMS 800 pump, but no patient complained about scrotal discomfort because of Pump-Unit size.
One year after activation, 115 out of 147 patients (78.23%) presented social continence. Twelve out of 147 patients (8.17%) presented an improvement with two pads per day. The success rate (social continence + improvement) reached 86.40%. After 2 years, 65 out of 91 patients (71.43%) had social continence when 11 out of 91 patients (12.09%) showed improvement. The success rate was 83.52%. Three years after activation, 18 out of 23 patients (78.26%) had social continence without any patient in the improved group, so success rate was 78.26%. Continence rates before and after device implantation are presented in Table I.
Continence rates before and after device implantation
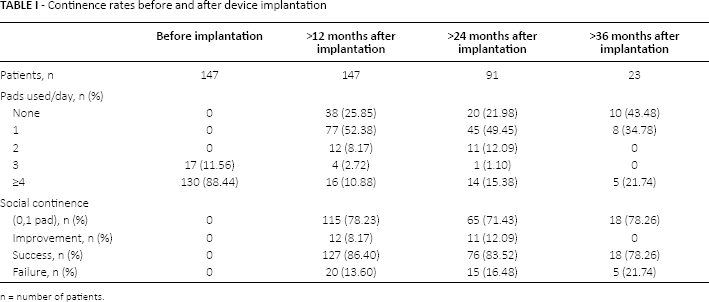
n = number of patients.
Postoperative complications occurred in 33 patients (22.44%). There were nine cases (6.12%) of infection leading to a total device removal. Two out of nine patients had a scrotal infection only without any associated urethral infection or urethral erosion.
Postoperative erosion of the urethra occurred in 19 cases (12.92%). Mechanical failure (saline leakage) with resultant device reimplantation occurred in five cases (3.40%). The cause for saline leakage was kink-resistant tubing breakage, leakage of the pump and intraoperative injury of the silicone kink-resistant tubing connecting the cuff with the Pump-Unit. The ZSI 375 implantation-related complications by aetiology of UI are presented in Table II. Patients who underwent pelvic irradiation were more prevalent in the failure group than in the success group.
ZSI 375 implantation-related complications by aetiology of urinary incontinence
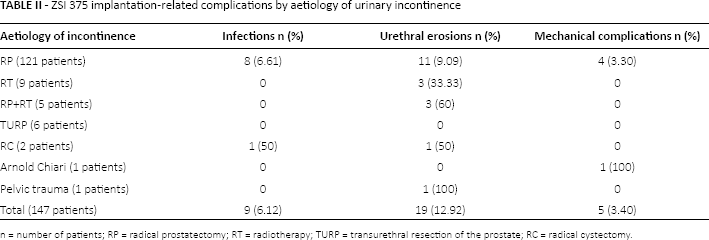
n = number of patients; RP = radical prostatectomy; RT = radiotherapy; TURP = transurethral resection of the prostate; RC = radical cystectomy.
Discussion
AMS 800 AUS is currently considered the gold standard treatment for male severe SUI, but it has several drawbacks such as complexity of preparation and of procedure. Last version from 1983 did not improve the design of the cuff to reduce the potential for creasing and fracture leading to leakage and there is no possibility to readjust the cuff in case of urethral atrophy (4). In case of poor result on continence, issued pressure cannot be adjusted, the AMS Pressure-Regulating Balloon has to be changed and the patient has to undergo a new procedure. ZSI 375 has been developed to overcome the lacks of AMS 800. Although long-term follow-up and large population of patients are necessary to evaluate an AUS, a follow-up of 12, 24 and 36 months with 147, 91 and 23 patients, respectively, is reliable to evaluate safety and efficiency of a new AUS. In the current study, we report a multicentre experience from Germany, Poland, Italy, Spain, England and Colombia. One hundred forty-seven patients were implanted with this device. The majority of reports that quote high success rates of AMS 800 come from the centres of excellence. Our centres are a mixed of centre of excellence and centres with minor or no experience with AUS implantation. All implanters reported the implantation procedure being very simple and straightforward and our success rate confirms that a short learning curve is required to achieve mastery. The results are in line with those of Staerman et al (16). ZSI 375 previous series outcomes have shown excellent short-term results, which ranged from 87 to 94.2% (15-17). Regarding the AMS 800 numerous studies, disparate continence rate are presented from total continence ≤ 90% (4, 5, 18-20) to 73% of patients dry or substantially dry and 88% showing improvement (21). Our social continence rate and success rate of the 12, 24 and 36 months follow-up period meet AMS 800 performances.
In our study, the short-term complication rate was similar with AMS 800 (4, 11, 22). The infection rate was 6.12% (nine patients) and occurred early in our series. It is equivalent to AMS 800 rates from 1 to 8.5% (4, 18, 22, 23).
Urethral erosion is well-known problem associated with the use of AUS with a rate of 7 to 12% (4, 11, 22). In our study, erosion affected 19 patients (12.92%). Previous treatment for incontinence did not have any influence on erosion rate, nor issued pressure of 70-80 and 90-100 cmH2O. AUS results from the adjustable pressure learning curve were included in the study. The possibility to increase pressure must be done with care, as studies have shown that pressures in excess can compromise the blood perfusion in the urethra and can explain a high rate of erosion. Our rate or erosion could be decrease with a better handling of this adjustable pressure (24-26).
Although no comparable data regarding the outcome of the ZSI 375 device implantation in patients who underwent pelvic irradiation are available, our results are in agreement with studies on AMS 800 that noted erosion rates higher with previous radiation (26-28). However, this issue remains controversial, as a recent literature review has not confirmed such association with regard to the AUS implantation (5). Mechanical failure with device reimplantation occurred in five patients (3.40%). First generation of the sphincter was involved. The device defect leads to the Kink-resistant tubing reinforcement and a pre-filled version of the sphincter in 2015. The rate of mechanical failure in our series is comparable with the 6% rate of AMS 800 failure in contemporary series (4, 18, 29).
The present study reports on a multicentre experience with the ZSI 375 device implantation in a large series of male patients and with an acceptable follow-up duration. However, there were several limitations in the design and outcome analysis of this study that could be improved by future studies. The study was retrospective, and would benefit from a prospective, randomised trial evaluating the same outcomes. Assessment of continence was based on pad number and not on pad weight and did not use self-administered questionnaires.
Follow-up period is long enough to establish the safety and efficacy of the ZSI 375 device. It has been long enough to identify complications, as the mean time for erosion onset is 19.8 months and atrophy is 29.6 months. But mechanical failures need longer follow-up as mean time for onset is 68.9 months (30).
Conclusions
The ZSI 375 AUS is effective in treating severe UI in male, with a good success rate and acceptably low complication rate. Implantation was simple with no serious adverse events associated with the device. The ability to adjust issued pressure of the device by a trans-scrotal injections may reduce the need for surgical revision, but erosion rate shows that this possibility must be done with care.
Footnotes
Financial support: The authors received no financial support for this study.
Conflict of interest: T. Pottek declares consultancy work, lectures for AMS, Zephyr (Geneva, Switzerland) and Teleflex (Limerick, USA). I. Ostrowski has done one surgical support in Serbia for ZSI.