
Abstract
Introduction
The epidemiology of lung cancer is changing worldwide, with smoking being the key driver of lung cancer incidence and mortality. Our aim is to analyze the incidence, survival and mortality trends in Italy in the framework of the 2017 survey on smoking behavior in Italy.
Methods
AIRTUM 2017 reports on cancer survival and incidence; 2017 survey on smoking behavior in Italy.
Results
Men achieved progress in lung cancer control characterized by a decrease in incidence and mortality and an increase in survival. The decreasing use of tobacco in men (from 60% in the 1960s to 24% in 2017) was most likely responsible for the decreasing incidence and mortality. Women showed no progress: although survival improved slightly, the incidence and mortality were both on the rise. This was most likely due to the increasing smoking rates in women in the 1970s and 80s. Of major concern is the accelerated rise in the number of smoking women from 4.6 million in 2016 to 5.7 million in 2017 compared to the decrease observed in men (from 6.9 to 6 million).
Conclusions
The incidence and mortality trends in males clearly demonstrate that primary prevention is the most effective way to reduce lung cancer mortality. By contrast, a 24% increase in the prevalence of smoking among women in just 1 year is extremely worrying for the future, and calls for immediate action by targeted strategies to reduce tobacco consumption in women and avert the dreadful prospect of a lung cancer epidemic in Italy.
Introduction
Lung cancer cases were 1.8 million in 2012 across the globe, corresponding to 13% of all cancers (1). Lung cancer was the most common cancer in men worldwide with 1.2 million new cases per year; meanwhile, nearly 600,000 new cases were diagnosed in women in 2012. Differences were also observed between regions, with 758,000 cases occurring in the more developed areas and more than 1 million of cases diagnosed in the less developed areas. Lung cancer remains lethal everywhere in the world, with a 5-year survival rate below 20% (2). Because of the high incidence rates and low survival, lung cancer is the most common cause of death from cancer worldwide with 1.59 million deaths, more than 1 million in men and 491,000 in women (1). In Europe, it is the third most common cause of cancer, after breast and prostate cancer (1).
The epidemiology of lung cancer is changing in many areas of the world in terms of incidence by gender, age class and histological type (3, 4). Different histological subtypes are linked to different risk factors; for example, outdoor particulate matter has been recognized as a stronger risk factor for adenocarcinoma of the lung than for other histologies, while smoking has been associated in the past mainly with squamous cell carcinoma. However, because of the dissemination of low-tar filter cigarettes, smoking has been hypothesized to be linked also with adenocarcinoma (3). Lung cancer appears to have biologically different characteristics in men and women. The histological distribution of lung cancer subtypes is distinctly different and female smokers are more likely to develop adenocarcinoma of the lung than squamous cell carcinoma, which is more common in men (4). However, the differences in incidence rates between men and women are mainly attributable to the different exposure to tobacco smoking (3).
The aim of this paper is to analyze the lung cancer incidence, survival and mortality trends in Italy in the last available 15 years by using the data of the Italian Association of Cancer Registries (AIRTUM; http://registri-tumori.it/cms/).
While assessing the progress in lung cancer control in Italy, we will speculate about possible reasons for the observed changes over time and we will outline opportunities to reduce the burden of lung cancer in the discussion section of this article.
Materials and Methods
Data
Formally established in 1997, AIRTUM promotes and supports activities and research programs for both general and specialized population-based Italian cancer registries (CRs). AIRTUM has developed a central database to collect and store CR data and make them available for collaborative studies and research activities after an official quality check in terms of data accuracy and completeness. Currently the AIRTUM CRs cover more than 35 million people, corresponding to 60% of the Italian population. AIRTUM has had a central database since 2005, which stores data from all accredited CRs. All CRs transfer data to the AIRTUM database in accordance with a standard protocol, performing regular updates over time. Each registry can send new data or update old records with new variables, including follow-up for vital status. The network standard protocol describes the inclusion criteria, data format, and checks. (For detailed information see http://www.registri-tumori.it/cms/files/2010.pdf).
Data published in the most recent AIRTUM reports on survival (5) and incidence (6) were selected for this paper.
Statistical analyses
For the joint analyses of incidence, mortality and survival (5), 23 CRs covering the period 1999-2010 and representing the population of 4 Italian macro-areas: Northwest Italy (Biella, Genoa, Mantua, Milan, Sondrio, Turin, Varese), Northeast Italy (Alto Adige, Ferrara, Friuli Venezia Giulia, Modena, Parma, Reggio Emilia, Romagna, Trento, Veneto), Central Italy (Umbria, Latina), and South Italy (Naples, Ragusa, Salerno, Sassari, Siracusa) were included. The study period was stratified in triennia.
Incidence and mortality rates were standardized by age with the direct method using the old (1960) European standard population. The average annual percent change of incidence and mortality rates was expressed by an indicator called annual percent change (APC), which explains synthetically the trend and the intensity of the variation in time. This model is based on linear segments connected at join points that represent the best fit of the observed data, that is, the segments that minimize the sum of the square of the differences between the estimated and observed data. APC was estimated with JoinPoint regression models available in the software distributed by the NCI (https://surveillance.cancer.gov/joinpoint/download).
Five-year net survival was estimated with the Pohar-Perme method (7). Survival changes were measured in terms of absolute percentage difference (APD) between the 5-year age-adjusted net survival estimates in 2008-2010 and 1999-2001. We combined statistically significant changes of the 3 indicators to identify patterns discriminating optimal/inadequate progress in cancer control. Incidence and mortality rates were standardized by age with the direct method using the old (1960) European standard population.
Analysis by tumor histology was performed considering among adenocarcinoma the ICDO-3 codes 8050, 8140-8149, 8160-8162, 8190-8221, 8250-8263, 8270-8280, 8290-8337, 8350-8390, 8400-8560, 8570-8576 and 8940-8941 and among squamous cell carcinomas the ICD-O3 codes 8051-8052, 8070-8084 and 8120-8131 (8).
For the joint analyses of incidence and mortality trends and projection to 2016 (6), 10 CRs covering the period 1999-2011 were included (Varese, Parma, Reggio Emilia, Modena, Romagna, Umbria, Naples, Turin, Ragusa and Siracusa).
Results and Discussion
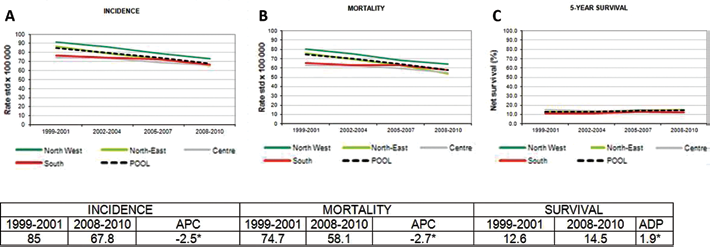
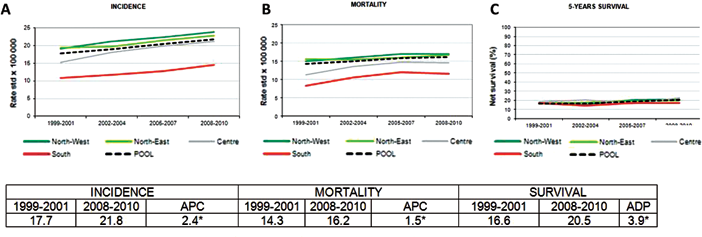
Figures 1 and 2 present changes in incidence, mortality and 5-year net survival between 1999-2001 and 2008-2010 for lung cancer in males and females, respectively.
POOL AIRTUM 1990-2010, males. Age-standardized incidence (
POOL AIRTUM 1990-2010, females. Age-standardized incidence (
Incidence
In the period 2008-2010 the lung cancer incidence in Italy was 67.8/100,000 in men and 21.8/100,000 in women (Figs. 1A and 2A). This translated into more than 41,000 new lung cancer cases, 28,000 in men and 13,500 in women (6). The number of new lung cancer cases must be interpreted with caution because it reflects both the distribution of risk factors (including smoking prevalence over time in the 2 sexes) and population aging.
A big difference between the incidence rates for men and women was still observed in 2008-2010 (68 and 22, respectively), even though the rates were gradually converging over time (Figs. 1A and 2A). This was due to the downward trend among men and the sustained increase in incidence in women. These trends may be largely attributable to previous smoking rates. Cigarette smoking or tobacco use is the most important causal risk factor for lung cancer development, with a long latency of 30 years between exposure to tobacco smoke and lung cancer development. Thus, the incidence trends and figures reported in this paper reflect the smoking prevalence of the late 1970s and 80s. In Italy, the smoking prevalence steadily declined until 2008 overall (from 35.4% to 21.7%) and in men (from 65.0% to 23.9%), while in women it increased from 6.2% in 1957 to 25.9% in 1990, and declined thereafter to 17.9% in 2008 (9). According to the recent survey on smoking habits in Italy (10), the smoking prevalence reached 24% in men and 21% in women in 2017. The latter percentage needs to be interpreted with caution since the variability for this estimate in a subgroup could be very large. Decreasing male tobacco use was most likely responsible for the decreasing incidence trends observed in men in this paper. By contrast, the increasing incidence trend in women was most likely due to the increasing smoking rates in women until the 1990s. A point of concern is that in just 1 year (from 2016 to 2017) the number of smoking women increased from 4.6 million to 5.7 million whereas the number of smoking men decreased from 6.9 to 6 million. This trend in women is extremely worrying because, if no changes occur, it will most likely lead to an increase in lung cancer incidence in women in the future.
Considering the carcinogenic role of secondhand smoke, also the data on the exposure to secondhand smoke in homes and cars are of note. Out of 688 smokers, 34% reported they could smoke everywhere in the home while 29% reported they could smoke only in selected rooms such as the bathroom or kitchen (10). In cars, 10% of nonsmokers reported having traveled with people who smoked and 61% of smokers reported they smoked in the car (10).
Figures 3 and 4 report the incidence trends (POOL AIRTUM CRs, period 2003-2012) for adenocarcinoma and squamous cell carcinoma in men and women, respectively. Data for other histological types are not available. The incidence of squamous cell carcinomas decreased in men while no major changes were observed in women; the incidence of adenocarcinomas increased in both men and women. A factor that may have contributed to the decreased incidence of squamous cell carcinomas of the central airways and the increased incidence of peripheral adenocarcinomas is the changed composition of cigarettes, which has resulted in deeper inhalation (11). Furthermore, with smoking cessation the risk declines more rapidly for squamous cell carcinoma than adenocarcinoma, which partly explains the increasing incidence trends of adenocarcinoma observed in men and women (11, 12). However, in this context it is important to take into account the recent findings of Gharibvand et al (13), who assessed the association between ambient fine particulate matter (PM2.5) and lung cancer among never smokers. Most of the lung cancers in this study (66.4%) were adenocarcinomas and an increase of 22% in the lung cancer risk was observed for each 10-μg/m3 increase in ambient PM2.5 concentration. In another study the increase in risk was found to be 55% for adenocarcinomas (14). Future studies that evaluate trends in adenocarcinomas and other histological subtypes should consider specific airborne environmental exposures in addition to socioeconomic factors and tobacco exposure (11). Finally, studies in Southeast Asia, where the prevalence of smoking among women is low, have suggested that the rise of adenocarcinomas in women can be attributed to secondhand smoke and cooking fumes (15).
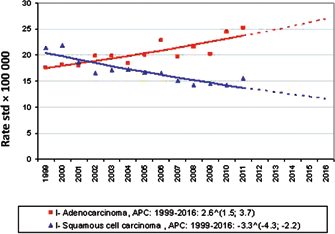
AIRTUM estimates of incidence time trends for 1999-2016 by histology in males. Age-standardized incidence (direct method, standard population: European population). APC = annual percent change. Reproduced with permission from AIOM & AIRTUM. I numeri del cancro in Italia 2016. Rome: Il Pensiero Scientifico Editore 2016.
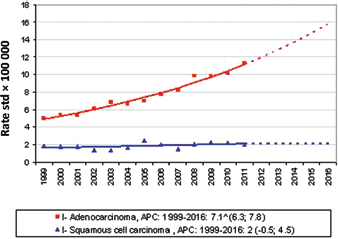
AIRTUM estimates of incidence time trends for 1999-2016 by histology in females. Age-standardized incidence (direct method, standard population: European population). APC = annual percent change. Reproduced with permission from AIOM & AIRTUM. I numeri del cancro in Italia 2016. Rome: Il Pensiero Scientifico Editore 2016.
The Italian incidence rates were high but comparable to those reported internationally in similar countries in 2012. The highest incidence rates for men were reported in Central and Eastern Europe (53.5/100,000) and East Asia (50.4/100,000) and for women in the United States (33.8/100,000) and Northern Europe (23.7/100,000) (15). For these estimates the world standard population was used whereas for the Italian data the European standard population was chosen. The European population was used for Italy because it was closer to the distribution of the resident population. The world population is slightly younger than the European population and the rates therefore tend to be lower.
Interestingly, the incidence pattern reported in Italy was observed in many countries with a high or very high human development index (HDI), namely Australia, Canada, Russia, the United States and Europe (Denmark, Germany, Netherlands, Sweden and United Kingdom), although in the United States the incidence has begun to show signs of a decreasing trend among females since 2010 (16). Also in these countries, the epidemic of lung cancer aligns with historical patterns of tobacco use. From 1980 to 2012, for men, annualized rates of decline of 2% or more occurred in 17 countries: Canada, Mexico, United States, Australia, South Africa, Venezuela, Nigeria, Antigua and Barbuda, New Zealand and Japan, and in Europe in Iceland, Norway, Sweden, Denmark, Italy, United Kingdom and Poland (16). For women, annualized rates of decline greater than 2% were achieved in 22 countries, while 12 countries exhibited statistically significant increases in prevalence since 1980. Bolivia, Canada, Denmark, Iceland, Israel, Norway, Sweden and the United States all had prevalence rates higher than 20% in 1980 but achieved annualized rates of decline of greater than 2%, whereas Austria, Bulgaria and Greece, which also had prevalence rates greater than 20% in 1980, showed statistically significant increases since then (16).
Mortality
In Italy, in the period 2008-2010 the mortality rate of lung cancer was 58 in 100,000 men and 16 in 100,000 women (Figs. 1B and 2B). The lung cancer mortality rates have changed substantially over time (Figs. 1 and 2), mirroring the incidence rates, with reductions in mortality among men and increasing trends among women, and with male-to-female mortality rates converging over time.
If we look at the geographic regions of the world, the highest mortality rates for men were observed in Central and Eastern Europe (47.6 in 100,000) and East Asia (44.8 in 100,000) (14). The highest mortality rates among women were in North America (23.5 in 100,000) and Northern Europe (19.1 in 100,000) (15). For many EU and non-EU countries (e.g., Australia, Denmark, France, Germany, Sweden and the United States), the trends in lung cancer mortality closely mirrored those for incidence (15). Parallel and increasing sex-specific mortality trends were observed in Romania; mortality rates were stable for both sexes in Japan; and parallel decreasing trends by sex were reported in Hong Kong and the Russian Federation. Also the mortality trends align with the historical patterns of tobacco use previously reported (16). These results are not surprising considering that, because of the high fatality associated with lung cancer, the geographical patterns in mortality closely follow those of incidence. As noted for the incidence comparison, also for the mortality rates these international data should be compared with the Italian ones considering the different standardization used.
Survival
In Italy, the 5-year lung cancer survival was 14.3% (12.6% for men and 16.6% for women) (Figs. 1C and 2C), which was higher than the EU average (13%) and that of the Northern European countries (12.2%) (17).
The low survival rate of patients with lung cancer is related to the stage of lung cancer at diagnosis. This determines the treatment options and has a strong influence on the length of survival. The earlier lung cancer is caught, the better chance a person has of surviving 5 years after being diagnosed. A population-based study performed in Northern Italy showed that, overall, 10% of new lung cancer cases were stage I, 50% stage IV, and 12% stage unknown. Three-year survival was 14% overall: 69% for stage I and 3% for stage IV (18). In the United States, in the period 2007-2013, 16% of lung and bronchus cancers were diagnosed at localized stage, 22% at regional stage, and 57% with distant metastases. The 5-year survival was 55.6%, 28.9% and 4.5% for localized, regional and distant lung cancer, respectively (19).
In addition to stage at diagnosis, variation in the treatment of lung cancer (e.g., time to curative treatment and adherence to guidelines) is likely an important determinant of survival and of the differences in survival between countries (20, 21).
Women tended to have higher survival rates than men (5-year net survival 20.5% in women and 14.5% in men) (5). This is a well-known phenomenon attributed to a mix of biological factors and tumor characteristics: hormonal status, comorbidities, histolological case mix (more adenocarcinomas in women than men), and the different natural history of lung cancer for men and women (22).
Despite the poor prognosis, a slight increase in survival was observed for men and women with an absolute percentage difference of 1.9 and 3.9, respectively (Figs. 1 and 2).
Any progress in lung cancer control?
Figures 1 and 2 present the changes in incidence and mortality rates and in 5-year net survival between 1999-2001 and 2008-2010 for lung cancer in men and women. We identified different patterns for men and women according to the progress in lung cancer control.
Men showed progress in lung cancer control, as characterized by a decrease in incidence and mortality and a slight increase in survival. Between 1999-2001 and 2008-2010, the incidence and mortality rates declined significantly by 2.5% and 2.7% per year, respectively. Survival increased significantly from 12.6% to 14.5%.
By contrast, women had no progress because the cancer burden worsened, i.e., the incidence and mortality were both on the rise, even though survival improved slightly. For lung cancer in women, the incidence rates increased annually by 2.4% in 1999-2010 (from 17.7 to 21.8 per 100,000); the mortality increase (APC +1.5%) was possibly mitigated by a small but statistically significant 5-year net survival improvement (from 17% to 20%).
As discussed earlier, the key driver of trends in lung cancer incidence is smoking. Because of the limited efficacy of high-cost screening and treatment measures, smoking is also a key driver of lung cancer mortality (23, 24). Thus, smoking cessation and changes in other risk factors mainly contribute to explaining the decline in incidence and therefore in mortality. The slight increase observed in survival might be due to changes in stage distribution at diagnosis, changes in the histological subtype case mix (more adenocarcinomas, which have higher survival than large cell and small cell lung cancer (15)), a high proportion of EGFR mutation-positive lung cancers for targeted therapies (15), as well as to a real improvement in diagnostic and treatment strategies (17). Further studies focused on histological, clinical and molecular features of lung cancer are needed to properly interpret the survival changes and disentangle the role of the diagnostic pathway and treatment progress.
In Italy, men have benefited from a decreasing smoking prevalence and are likely to experience continued reductions of the lung cancer incidence over the coming years. Conversely, the rates of lung cancer in women are expected to rise, given the new signs of increasing smoking prevalence.
Currently, effective tobacco control programs seem critically important in the battle to reduce the burden of lung cancer. This will be of particular importance for young women. In the young population (25-44 years), female lung cancer mortality is predicted to reach similar rates to those of men if not to surpass those of men by 2017 (1.38 in women vs. 1.21 in men) in the EU (25), and the same pattern was seen in Italy (25).
Italy was the first large country in 2005 to adopt comprehensive tobacco legislation, banning smoking in all indoor workplaces and public places (26). However, from 2006 to 2013 a decrease in the implementation rate of tobacco control measures was observed in Italy compared with other European countries (27, 28). This could explain the trends in smoking prevalence reported in Italy in the recent survey (28). In 2016, new legislation on tobacco, transposing the Directive 2014/40/EU, was introduced in Italy to further decrease the social acceptability of smoking, reduce smoking by the younger generations, and limit secondhand smoking exposure among children.
Conclusion
The availability of population-based cancer data to assess the lung cancer burden and monitor emerging trends is of crucial importance together with the availability of surveys on the prevalence of tobacco smoking. Primary prevention is the most effective way to control the lung cancer epidemic. Tobacco legislation and tax policies still offer a great opportunity to control lung cancer; however, a comprehensive lung cancer control policy including coordinated strategies to reduce exposure to all recognized risk factors including secondhand smoke, air pollution, radon, asbestos, and occupational carcinogens will be essential to tackle the lung cancer epidemic in future.
In Italy, the incidence and mortality trends in males clearly demonstrate that primary prevention is the most effective way to reduce the lung cancer mortality. By contrast, a 24% increase in the prevalence of smoking in women in just 1 year is extremely worrying, and calls for immediate action and targeted strategies to reduce tobacco consumption by women and avert the dreadful prospect of a lung cancer epidemic in Italy.
Footnotes
Financial support: None.
Conflict of interest: The authors declare no conflicts of interest.