
Abstract
One of the priorities of personalized medicine regards the role of early integration of palliative care with cancer-directed treatments, called simultaneous care. This article, written by the Italian Association of Medical Oncology (AIOM) Simultaneous and Continuous Care Task Force, represents the position of Italian medical oncologists about simultaneous care, and is the result of a 2-step project: a Web-based survey among medical oncologists and a consensus conference. We present the opinion of more than 600 oncologists who helped formulate these recommendations. This document covers 4 main aspects of simultaneous care: 1) ethical, cultural, and relational aspects of cancer and implications for patient communication; 2) training of medical oncologists in palliative medicine; 3) research on the integration between cancer treatments and palliative care; and 4) organizational and management models for the realization of simultaneous care. The resulting recommendations highlight the role of skills and competence in palliative care along with implementation of adequate organizational models to accomplish simultaneous care, which is considered a high priority of AIOM in order to grant the best quality of life for cancer patients and their families.
Introduction
Every year in Italy, about 364,000 people are newly diagnosed with cancer, and about 30%-35% present with advanced disease at diagnosis (1). Cancer-related physical symptoms, together with psychological distress and social and spiritual needs arising in the course of the disease severely affect the quality of life of the patient and family (2). There is evidence that early integration of palliative care in clinical practice significantly improves quality of life and potentially even survival in patients with advanced cancer (3, 4) and provides an appropriate care setting along with a reduction of costs by reducing the inappropriate use of chemotherapy in the last months of life (5, 6). It is the responsibility of the oncologist who is in charge of the patient to guarantee early palliative care activation (2, 7, 8). Such a simultaneous approach requires a cultural change in oncologists, and several organizational barriers can hinder the efforts of individual operators (9-11). A global consensus on the best organizational model for providing early access to palliative care for cancer patients is currently lacking (12-14), and recent international surveys show that referral to palliative care occurs late in the course of cancer (15, 16).
The European Society for Medical Oncology (ESMO) has been leading the way since 2003 by formally accrediting Designated Centers of Integrated Oncology and Palliative Care (ESMO-DCs) (7). In 2006, the Italian Association of Medical Oncology (AIOM), according to the ESMO program, set up the simultaneous and continuous care (SCC) task force, with the main goals of training oncologists in palliative medicine and spreading the culture of integration between oncologists and palliative care teams in every oncology unit in Italy (8).
From 2003 to 2015, 42 Italian oncology units were appointed ESMO-DCs, ranking first among European countries. The limited availability of palliative care services in Italian hospitals makes it difficult to guarantee an integrated approach, a situation that is similar in other countries (4). Moreover, in Italy, early introduction of palliative care in clinical practice is still a work in progress, with different models applied according to local and regional organization, with the common aim being to ensure a careful assessment and management of symptoms as well as cancer-directed therapy in metastatic cancer patients (10).
Methods
A Web-based questionnaire covering the main aspects of simultaneous care (SC) was developed within a focus group by members of the AIOM SCC task force. The questionnaire was accompanied by 4-5 selected articles for each of the 4 main covered areas: (1) ethical, cultural, and relational aspects and implication for patient communication (17-22); (2) medical oncologist training in palliative medicine (23-26); (3) the most relevant objectives for clinical trials in advanced cancer patients (27-29); and (4) the best organizational and management models for palliative care in conjunction with cancer treatment (12, 30-34).
The tool was reviewed by oncologists within the task force and AIOM board members for content validity. The final version of the 37-item questionnaire was sent by e-mail to all 1,119 AIOM members.
A total of 449 medical oncologists, which account for 40.1% of AIOM members, completed and returned the questionnaires. These were analyzed and the answers were used to set up the bases for the consensus conference. The results of the survey were recently published (35).
The national AIOM conference on SC was held in Rome in September 2013 and was attended by over 200 oncologists, with the main aims being (1) to report and discuss the results of the national survey; (2) to acknowledge the attitudes and oncologist-related barriers or organizational obstacles to the provision of optimal SC in clinical practice; and (3) to produce a final consensus document on SC, since AIOM has identified early palliative care as an important goal.
The Web-based questionnaire results represented the basis for the panel discussion and recommendations.
During the conference, participants were divided into 4 working groups focusing on the 4 areas proposed in the questionnaire, which are the 4 main areas of evidence and controversy present in the literature and previously specified.
Each group was coordinated by a member of the AIOM SCC task force, who supported the group by means of the selected literature described above and the results of the survey.
In each group, the results of the survey were reviewed, and a final agreement was defined.
Discussion also took into account the Italian background and previous assessments about these topics (36-40).
Eventually, the results of the discussion of each group were presented in a plenary session in order to make eventual additional comments and share agreement among all participants.
The final document that we propose here thus includes the opinion of more than 600 Italian oncologists who have found agreement on SC recommendations.
Results
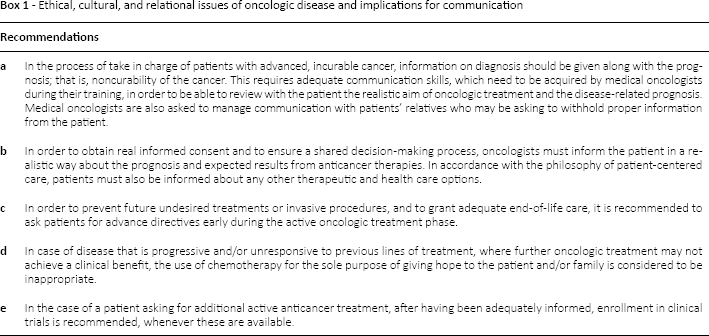
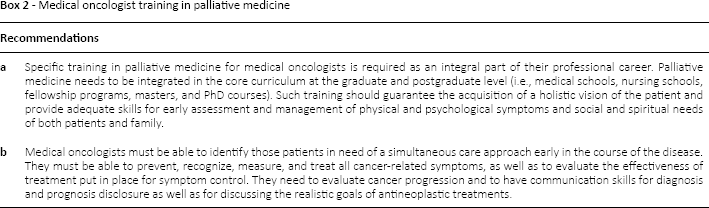
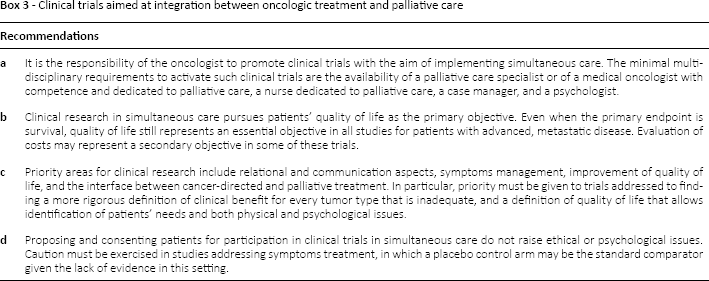
The final document was approved by AIOM board members in 2014 and has been published on the AIOM Web site (41). The AIOM recommendations and statements for each section of the document are provided in Boxes 1-4.
Ethical, cultural, and relational issues of oncologic disease and implications for communication
Medical oncologist training in palliative medicine
Clinical trials aimed at integration between oncologic treatment and palliative care
The organizational and management models for simultaneous care (SC)
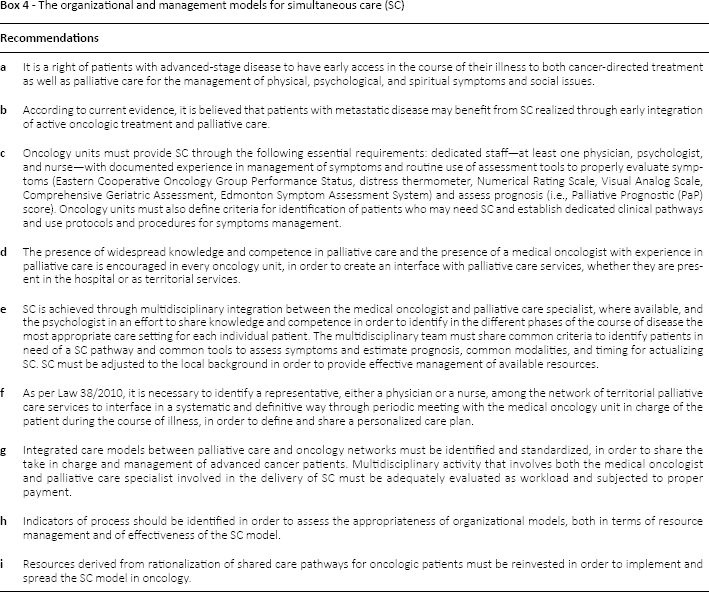
As highlighted in the document-derived recommendations, early activation of palliative care concomitant to cancer-directed treatment in the setting of advanced/metastatic disease is considered one of the top priorities by the community of Italian medical oncologists.
Discussion
The urge for early integration of palliative care is evident as data on prevalence of severe symptoms in patients admitted to oncology units in Italy show more than 60% of patients presenting more than 3 severe symptoms (39).
There were no particular barriers highlighted by oncologists for the spread of early palliative care. Most oncologists in Italy have developed expertise in palliative care and can also provide symptom control.
One possible drawback is related to the fact that SC require a revision of the current organizational models of health care, along with a close collaboration between community-based and hospital services dedicated to cancer patients, and this is considered a compelling need.
Palliative care should also require specific skills for the conduction of clinical trials as well as for correct translation of results in clinical practice. The application of a rigorous methodology for clinical trials, which is part of the cultural background of medical oncologists, could help promote the rapid growth of scientific evidence in various aspects of SC that have been poorly studied. Given the large variety in settings and competence of oncologists across Italy, different models of early integration of palliative care can be suggested by sharing assessment tools and with low, intermediate, or high level of integration, according to available resources and personal competences (12, 35, 36).
Individual groups and practices will need to structure their models to guarantee early palliative care application, based on their specific framework.
AIOM indicates that palliative care services should be present within oncology departments, to allow a close integration through regular multidisciplinary meeting and patient discussion. This model requires specific skills and the ability to share the care pathway as overall value to offer to the patient (42).
The diffusion of integrated care models of early palliative care could also provide a useful way to reduce the high rate of mortality of cancer patients in acute hospital wards in Italy (43). Overall, the AIOM priorities that emerged from the consensus conference were as follows: (1) promotion of education of medical oncologists in palliative care, considering it an integral part of their core curriculum; (2) increase the number of oncology units obtaining ESMO-DC certification; (3) activation of a task force with the Italian Society of Palliative Care to share the language and organizational models for patients’ clinical pathways; (4) promotion of prospective clinical trials on SC; (5) implementation of the culture of value and personalized medicine in oncology; and (6) involvement of patient associations in order to share the objectives of care.
On the basis of these priorities, in 2015 a shared AIOM-SICP document was produced and published on the AIOM Web site (44). In this document, the different models of early palliative care proposed by ESMO, American Society of Clinical Oncology, National Comprehensive Center Network, and European Association for Palliative Care are compared, and strengths and weaknesses analyzed. The working group then suggests criteria for access to SC and decision-making steps, and provides multidimensional instruments for symptom relief (44).
Furthermore, a prospective multicentric randomized trial to assess the impact of SC in 207 metastatic pancreatic cancer patients has been activated and completed. This study confirms that systematic early palliative care significantly improves quality of life compared to on-demand palliative care (45). The same study also has shown a significant impact of SC on some indicators of end-of-life treatment aggressiveness, among which are the use of chemotherapy in the last days of life and hospital admission (46).
The AIOM commitment is now to implement, through guidelines (47-49) and consensus conferences for specific tumors (50), the approach of SC in a systematic way.
Recently, a Delphi international consensus identified 13 major and 30 minor indicators of integration of oncology and palliative care, through consensus among international experts (51). At an institutional level, these indicators represent milestones toward the vision of integration.
As discussed in this article, implementation of the process to achieve these milestones is likely going to be a stepwise process, requiring longitudinal commitment from oncologists, palliative care specialists, educators, and hospital administrators (51).
We are confident that the efforts of AIOM with regard to education, research, organization, and consensus about SC may help to place Italy among the worldwide leading countries able to provide global care of cancer patients through the illness trajectory.
AIOM is also committed to acting on institutions to allocate resources for early palliative care activation throughout the country, in order for SC to become a routine part of comprehensive cancer care for all cancer patients in Italy, a goal to be achieved before 2020, the deadline proposed by ASCO (52).
Footnotes
Acknowledgment
The authors thank Kathleen Marie Hughes for English review.
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.