
Abstract
Purpose
To provide an overview of the morphologic subtypes of ovarian carcinomas in Bulgaria in relation to current healthcare organization using Bulgarian National Cancer Registry data. Further, we investigated hospital volume as a factor influencing the quality of care for patients with ovarian cancer.
Methods
Bulgarian National Cancer Registry ovarian carcinoma data were retrieved (2009-2011) and distribution of histologic types was analyzed. Cases were divided and compared with respect to main treatment: no surgery, surgery at hospitals dealing with ≥30 ovarian cancer patients/year (high volume), and surgery at hospitals dealing with <30 ovarian cancer patients/year (low volume). We then estimated the odds of being diagnosed with adenocarcinoma and carcinoma not otherwise specified (NOS) vs specified morphologies (serous, endometrioid, clear cell, and mucinous), including age, grade, stage, and hospital volume, in a logistic regression model.
Results
A total of 2,041 ovarian carcinomas were distributed as follows: serous 47.7%, mucinous 11.9%, endometrioid 5.8%, clear cell 1.8%, and adenocarcinoma and carcinoma NOS 32.5%. More than half of cancer patients (n = 1,100, 53.9%) were surgically treated in low-volume hospitals and they had a larger proportion of cases with adenocarcinoma and carcinoma NOS: 33.3%, in comparison with 24.0% in high-volume hospitals (p<0.0001). The odds of being diagnosed with unspecified morphology, assumed as a proxy of suboptimal quality of care, are higher for patients surgically treated in low-volume hospitals (odds ratio 1.50 [95% confidence interval 1.21-1.87]) compared with high-volume hospitals after adjustment for age, stage, and grade.
Conclusions
The results of our study may serve policymakers and healthcare professionals when optimizing diagnosis and treatment of ovarian cancer in Bulgaria.
Introduction
Ovarian cancer is the fifth most commonly diagnosed female cancer in Europe, accounting for about 4% of all incident cancers and almost 5% of all cancer deaths in women (1, 2). The estimated incidence and mortality rates for 2012 are 13.1 and 7.6 per 100,000 women, respectively (1). According to the EUROCARE-5 estimates for Europe (3), 5-year relative survival for ovarian cancer patients, diagnosed in 2000-2007, was 40.8% (95% confidence interval [CI] 40.4% to 41.3%). In Bulgaria, both the incidence of and mortality from the disease are slightly higher than the European average rates, 17.9 and 8.0 per 100,000 women, respectively, while the survival is similar, 40.6% (95% CI 39.2% to 42.1%) (3).
Ovarian cancer comprises a heterogeneous group of tumors with more than 10 histologic subtypes, with ovarian epithelial tumors (carcinomas) being the most common among them, accounting for about 90% of cases. The 5 main subtypes of ovarian epithelial tumors (high-grade serous, low-grade serous, endometrioid, clear cell, and mucinous) are perceived as different diseases, with different risk factors, pathogenesis, and response to treatment (4). Therefore, recent epidemiologic studies report ovarian cancer burden indicators (incidence and/or survival) taking into consideration these morphologic subtypes (2, 5, 6). Cancer registries, which are the main source of data for population-based studies, record topography and morphology of the tumors, using the coding system based on the International Classification of Diseases for Oncology (ICD-O) (7). For the subtypes of ovarian carcinomas, ICD-O provides a specific range of codes for serous, endometrioid, clear cell, and mucinous tumors, but there is a morphology group of ovarian carcinomas in the cancer registries database that is not uniformly classified in the different studies.
The Cancer Incidence in Five Continents (CI5) series (2) defines 3 more subgroups of ovarian carcinomas in addition to serous, mucinous, endometrioid, and clear cell: adenocarcinoma, not otherwise specified (NOS), other specified carcinoma, and unspecified carcinoma, while in the study of Sant et al (6), there are 2 additional subgroups instead: undifferentiated (including carcinomas, NOS; carcinoma, undifferentiated, NOS; carcinoma, anaplastic, NOS; and adenocarcinoma, NOS) and other types (including selected codes from the following morphologic categories in ICD-O-3: epithelial neoplasms, NOS; transitional cell papillomas and carcinomas; adenocarcinomas; cystic, serous, and mucinous neoplasms; and several others) (7).
The RarecareNet study (rarecarenet.eu) has prepared a 3-tier list of rare cancers, specifying a category of epithelial tumors of ovary and fallopian tube, including adenocarcinoma with variants of ovary, mucinous adenocarcinoma, clear cell adenocarcinoma, primary peritoneal serous/papillary carcinoma, Müllerian mixed tumor of ovary, small cell ≠ NET, and adenocarcinoma with variants of fallopian tube.
Other smaller studies (8, 9) used even more different approaches for grouping the ovarian carcinomas, but they also attempted to separate adenocarcinoma, NOS and carcinoma, NOS from the other more specified morphologic subtypes.
Oncologic medical care in Bulgaria is decentralized—surgery is provided in specialized, university, and general hospitals, chemotherapy and radiotherapy in specialized and university hospitals, and emergency surgery in the surgical departments of all hospitals. The hospitals with surgical departments have their own pathologic laboratories, which are staffed and equipped differently according to the size and location of the hospital, and do not follow any hierarchical structure. Thus, the hospital of surgery is usually also the hospital of diagnosis.
Since the comparison between different populations of cancer burden estimates, such as incidence rates and survival by morphologic groups, may be affected by the definitions of these groups and by the coding practices in cancer registries, we aimed to analyze the distribution of morphologic subtypes of malignant epithelial ovarian tumors in Bulgaria in the context of the current organization of the oncologic medical services and cancer registration. On the other hand, the organization of health care, especially centralization of cancer services, has been considered by a number of researchers in recent years as an independent factor influencing survival of patients with ovarian cancer (10-11-12-13-14-15). Therefore, we also wanted to investigate if the low hospital volume is an issue contributing to the number of cases with unspecified morphologic characteristics, the latter assumed as a possible indicator of suboptimal quality of care.
Methods
The Bulgarian National Cancer Registry (BNCR) is population-based and collects information about all cancer cases since 1952. It yields comparable data that are reasonably accurate and close to complete (16). The information on each case is structured in more than 85 variables, concerning patient, cancer, and treatment. Pathologists are one of the main sources of information for the cancer registry, along with clinicians and death certificates.
Data from the BNCR for ovarian cancer cases (ICD-10 code C56) diagnosed in 2009-2011 were analyzed. Morphology is coded according to ICD-O-2 (17) and the subtypes of ovarian carcinoma were defined following the grouping used in CI5 series (18) and the subgroups adenocarcinoma NOS, other specified carcinoma, and unspecified carcinoma were combined into one category: adenocarcinoma and carcinoma NOS. Grade of the tumors and stage of disease follow the TNM6 rules (19). We divided the cases into 3 categories according to information regarding the main treatment (surgery): without surgery, treatment in hospitals with an average annual number of new ovarian cancer patients who underwent surgery ≥30 (high-volume hospitals), and treatment in hospitals with an average annual number of new ovarian cancer patients who underwent surgery <30 (low-volume hospitals). We then compared the characteristics of the patients treated in high-volume or low-volume hospitals using Pearson chi-square test with level of significance at p<0.05. In order to investigate if the treatment in low-volume hospitals is related to unspecified morphologic diagnosis, we first grouped the cases into 2 categories, adenocarcinoma and carcinoma NOS vs specified morphologies (including serous, endometrioid, clear cell, and mucinous tumors), and we estimated the odds of being diagnosed with adenocarcinoma and carcinoma NOS vs specified morphologies, including age, grade, stage, and hospital volume, in a logistic regression model.
Results
There were 2,343 patients with ovarian cancer diagnosed during the 2009-2011 period and registered at the BNCR as of January 1, 2014. Of those, 2,041 (87%) were cases with carcinoma, 124 (5%) other morphologies, and 178 (8%) unspecified malignant neoplasms. The latter 2 groups were considered ineligible for further analysis in this study.
The distribution of morphologic subtypes of ovarian carcinoma (n = 2,041) by selected characteristics is summarized in Table I.
Distribution of ovarian carcinoma cases by clinicomorphologic characteristics
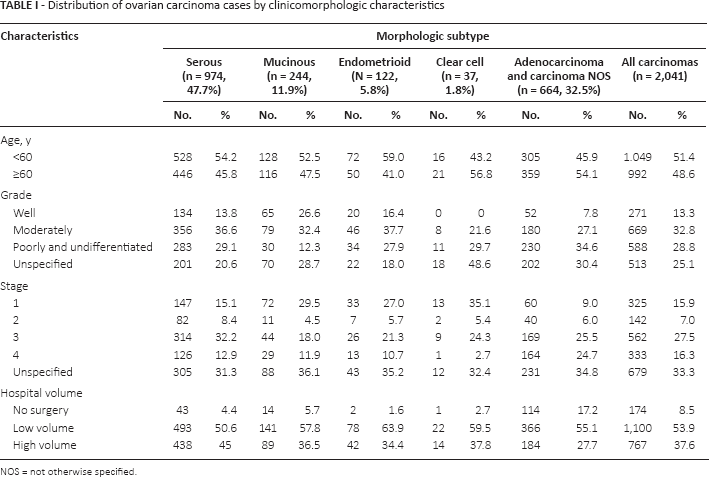
NOS = not otherwise specified.
Serous ovarian carcinoma was diagnosed in 47.7% (n = 974) of the patients. Among them, 54.2% were diagnosed before 60 years of age, with the highest proportions at stage III (32.2%) and moderately differentiated grade (36.6%).
Mucinous carcinoma was diagnosed in 12.0% of the patients and 52.5% out of all diagnosed were younger than 60 years of age, ranked first among unspecified stage (36.1%), and moderately differentiated grade was assigned in 32.4%.
The distribution of the patients with endometrioid carcinoma, which was diagnosed in 6.0% of them, followed a similar pattern as observed for mucinous carcinoma: 59.0% were diagnosed before 60 years of age, with overrepresentation of the unspecified stage (35.2%), and the bulk of tumors were graded as moderately differentiated (37.7%).
Clear cell carcinoma accounted for 1.8% of all ovarian carcinoma cases and distribution of patient characteristics is as follows: 56.8% were diagnosed at over 60 years of age, 35.1% were diagnosed at first stage, and almost half (48.6%) were of unspecified grade.
The distribution of characteristics for adenocarcinoma and carcinoma NOS (32.5% of all carcinomas) were not dissimilar: the majority of them were diagnosed at over 60 years of age (54%) and were poorly and undifferentiated (34.6%) with unspecified stage (34.8%).
More than half of the patients with ovarian carcinoma (n = 1,100, 53.9%) were surgically treated in low-volume hospitals. In high-volume hospitals, 37.6% (n = 767) of patients were treated, while 8.5% (n = 174) did not undergo curative surgery, but diagnostic histology specimen was obtained (Tab. I).
The distribution of characteristics of surgically treated patients with ovarian carcinoma by hospital volume is presented in Table II. The low-volume hospitals have larger proportion of cases with adenocarcinoma and carcinoma NOS: 33.3%, in comparison with 24.0% in high-volume hospitals (p<0.0001). Low-volume hospitals also seem to accumulate cases with unspecified grade (27.7% vs 14.3%, p<0.0001) and unspecified stage (37.9% vs 27.4%, p<0.0001).
Distribution of patients with ovarian carcinoma by biological characteristics and surgical hospital volume
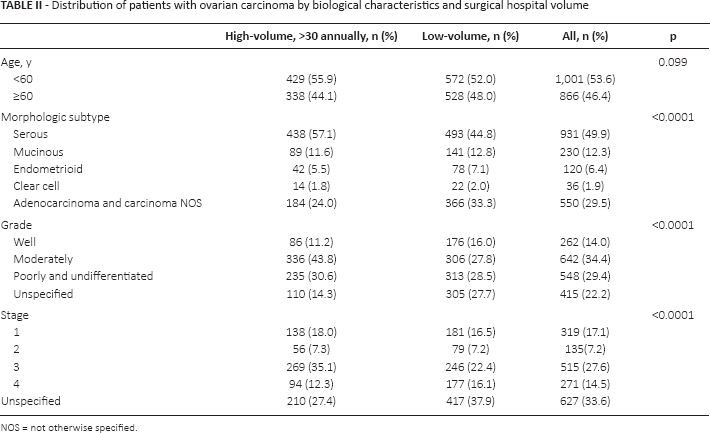
NOS = not otherwise specified.
There were 109 Bulgarian hospitals in the 2009-2011 period that reported surgical intervention in patients with ovarian cancer. Of those, 103 (94.5%) are low-volume hospitals that reportedly treated (diagnosed) about half of all patients. Only 6 hospitals (5.5%) (specialized oncologic and university hospitals) are high-volume and they cover about 40% of patients. The graph (Fig. 1) shows a long tail in the distribution of cases by hospital, representing the decentralization of surgical treatment.
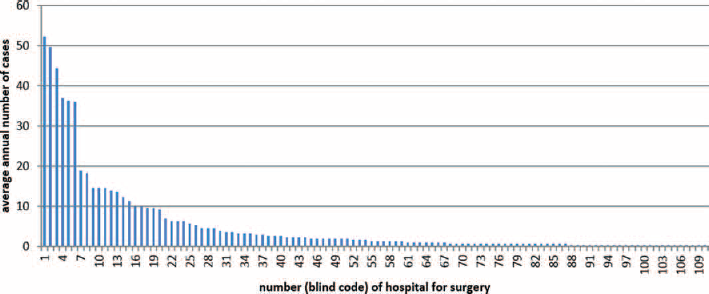
Distribution of surgically treated patients with ovarian cancer (diagnosed 2009-2011) by hospital. Hospitals were ranked by decreasing volume of cases after blind coding.
The odds of being diagnosed with unspecified morphology (adenocarcinoma and carcinoma NOS) are higher for patients surgically treated in low-volume hospitals (odds ratio 1.50, 95% CI 1.21-1.87) compared with high-volume hospitals after adjustment for age, stage, and grade (Tab. III).
Odds ratio (OR) of being diagnosed with adenocarcinoma and carcinoma NOS (vs specified morphologies) in patients with ovarian carcinoma
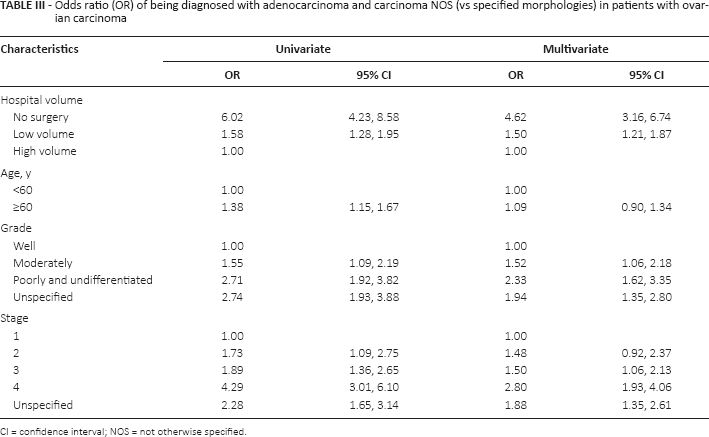
CI = confidence interval; NOS = not otherwise specified.
Discussion
In the present study, we analyzed the distribution of morphologic subtypes of malignant epithelial ovarian tumors in Bulgaria in the context of the current organization of oncologic medical services and cancer registration. In addition, we showed that low hospital volume is important when considering the number of cases with unspecified characteristics as a possible indicator of suboptimal quality of care.
The serous type of ovarian carcinoma is reported to be the most prevalent worldwide, with estimated proportion around 70% (4, 20, 21). In contrast, in Bulgaria, the number is much lower (48%), but still concordant with the reported estimate by authors from a single center in Edinburgh (52%) (22). If we assume that well-differentiated (G1) and low-grade serous cancer are the same, than the latter will comprise 6.6% of all ovarian cancers in our study, a number that seems slightly over the most cited 3%-5% (4, 20), but is close to the 7% cited in a Scottish article (22). The lower proportion of high-grade serous tumors (G2 + G3, 31%) might be explained with erroneous including of some of these cases in the group adenocarcinoma and carcinoma NOS, dominated by G3-4 cancers, and existence of 10% serous carcinoma with unspecified grade.
Recent advances in understanding of mucinous neoplasms with ovarian localizations (most of them have been recognized and reclassified as metastatic from gastrointestinal cancers) have led to a steady decline in the proportion of primary mucinous carcinoma of the ovary, not exceeding 2%-3% (4, 20, 21). In Bulgaria, mucinous carcinoma of the ovary has a fourfold higher proportion (12%), and it is impossible to overlook the advanced clinical stage in 30% of cases, unspecified stage in 36%. Many metastatic cancers were probably originally misdiagnosed as primary, often due to emergency surgery and lack of appropriate preoperative imaging studies, and this is reflected in the high proportion of patients at advanced stage. Some authors elaborated on comparable values, but lower than ours: Swedish Family-Cancer Database (1993-1999) reported that mucinous cystadenocarcinomas were 10.5% of epithelial ovarian cancers (23) and a German group estimated mucinous histology at 8% out of all ovarian carcinomas (8). The Surveillance, Epidemiology, and End Results Program (SEER) for 1988-2001 representing almost a quarter of the US population reported 9.7% of cases with mucinous type of epithelial ovarian carcinomas (24). It seems that the population-based studies reported higher proportions of mucinous histotype than the more detailed studies conducted by experts in gynecologic pathology.
Regarding ovarian endometrioid cancers in Bulgaria (5.8%), they were diagnosed with half the frequency of the same diagnosis from similar studies: 13%-13.5% for the SEER program (24) and Swedish Family-Cancer Database (23), reaching 21.4% reported in a Scottish article (22). The closest, but still higher, is the number cited by a German group (9%) (8), while according to experts in gynecologic pathology, the proportion is 9%-11% (4, 21). We speculate that the low proportion of endometrioid histology is largely due to labeling many endometrioid cancers simply as adenocarcinomas, without further specification.
Most difficult to discuss is clear cell carcinoma (1.8% in our country) owing to the large variability in the numbers often quoted, ranging from 1% to 12% for North America and Europe, whereas in Japan, the estimated proportion reaches 25% (25). In recent years, we witnessed the decline of endometrioid histology cases on the grounds of widespread use of immunohistochemistry, which led to reclassification of a part of G3 endometrioid cancers in the serous group (21). Decreasing proportions of endometrioid along with primary mucinous ovarian carcinoma resulted in the emergence of clear cell cancer histology as the second most common ovarian cancer type after serous (21). For long time now, the relation between clear cell histology and endometriosis has been elucidated, and there is a cause-effect correlation on endometriosis prevalence and distribution of clear cell ovarian cancer, exemplified by the Asian population (26). In Bulgaria, we do not have any data about the prevalence of endometriosis among the female population and thus we cannot explain the low proportion of endometriosis-related ovarian cancers, such as clear cell and endometrioid, observed in our study. Clear cell carcinoma grading is debatable, but the recommendations of the previous WHO edition from 2003 were to abstain from defining grades (27). Despite this recommendation, we observed some cases graded as G2 or G3 in our analysis, which might reflect insufficient adherence to the WHO classification.
The coding in the cancer registry is based mainly on what is written in the pathologic reports, but do all pathologists adhere to up-to-date classifications? At times, diagnosticians use terminology that formally reflects morphologic features of cancer tissue, e.g., cystadenocarcinoma or papillary cancer, but these seem to have no relevant clinical meaning; at other times, simple generic terms like cancer or adenocarcinoma are employed due to lack of auxiliary techniques to detail the cancer histotype, especially when faced with a poorly differentiated tumor. Thus cancer registry entries of choice are codes like carcinoma/adenocarcinoma NOS or undifferentiated cancer. Therefore, when conducting epidemiologic studies, investigators group the codes in a way that can make it harder to compare data from different registries and across individual studies. More importantly, some discrepancies emerge when comparing the relative frequencies of each cancer histotype as defined by epidemiologic registries and when reported by groups with leading experts in gynecologic pathology based on their own diagnostic observations.
Our study is based primarily on data stemming from the BNCR. One potential weakness comes from the lack of expert review of histologic slides by pathologists in this study and it raises concern that the observed relative and absolute numbers of the BNCR-reported morphologic subtypes could be different in reality. Data shown in Table I seem to contain an outstanding feature: nearly one third of all ovarian carcinomas bear the general label “adenocarcinoma or carcinoma NOS” without any further reference to histologic type. The proportion of “adenocarcinoma NOS” reported in the German article is 14% from all carcinomas and the percent for “carcinoma NOS” is 10% (8), although according to the WHO blue book, this diagnosis is considered to be an exception and has to be the final diagnosis only if distinctive features of one of the Müllerian types of adenocarcinoma are missing (27). Moreover, almost every third “adenocarcinoma and carcinoma NOS” in our study is devoid of grading. This disproportional overrepresentation of the group is largely due to lumping of cases from the other 4 major subtypes. The group “adenocarcinoma and carcinoma NOS” boosts with G3-4 cancers (35%), bearing in mind that often these tumors lack obvious histologic features, thus precluding precise assignment to a specific category without auxiliary studies. A reasonable explanation for this could be seen in the fact that the majority of patients with ovarian cancer in Bulgaria underwent surgery in hospitals with <30 hospital volume.
In addition, patients surgically treated in low-volume hospitals have a higher risk of receiving an unspecified diagnosis, which may result in inadequate treatment and poor outcome. Some researchers advocate for centralization of services, based on evidence for meaningful improvement in survival outcomes for women with ovarian cancer treated in high-volume hospitals (10-11-12-13-14). However, other investigators have shown that patients can receive good quality of care in low-volume hospitals if the specialists adhere to clinical guidelines (15). Currently, the organization of health care in Bulgaria is trending toward decentralization of cancer services, in a milieu of constraints in resource allocation, which predisposes to more obstacles to achieve the best outcome. Surgical pathologists are in shortage in low-volume hospitals, lacking subspecialization in the field of gynecologic oncology, rendering them ineffective participants in the continuing medical education paradigm. The small laboratories do not employ auxiliary studies like immunohistochemistry. In addition, central expert review of tumor slides is often inaccessible due to lack of an official and effective system.
Conclusion
The current analysis serves to describe the basic demographic and histologic characteristics of all malignant epithelial ovarian tumors reported for a given timeframe. Despite the concern that the observed relative and absolute numbers of the reported BNCR morphologic subtypes could be different in the reality, the results of our study may serve policymakers when optimization of diagnosis and treatment of ovarian cancer patients is discussed for planning resources and achieving better outcome.
Since the foreseeable future will likely witness the introduction of histology-based treatment options, this will require adequate histology reports, with about 95% of the ovarian carcinoma cases having final diagnosis from one of the following 5 categories: high-grade serous, low-grade serous, endometrioid, clear cell, or mucinous (4). In order to ensure better communication among different experts (pathologists and oncologists), a multidisciplinary guidebook in Bulgarian was introduced (28), aimed at familiarizing the medical community with the latest advances in diagnostics and therapy.
Footnotes
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.