
Abstract
Introduction
Despite the preference of many patients to die at home, high proportions of patients with advanced cancer undergo major procedures, receive intensive care, and die in the hospital. The goal of this study is to examine variation in hospital utilization and site of death for patients dying with poor-prognosis cancer in the Regione Emilia-Romagna (RER), Italy.
Methods
We conducted a retrospective, population-level study using administrative data. Patients were included if they died in 2012 and had at least one hospital admission for metastatic or poor-prognosis cancer within 180 days of death. Variations in the use of the hospital, intensive care, and procedures performed were evaluated.
Results
11,470 patients died with metastatic or poor-prognosis cancer in 2012. Seventy-eight percent of patients were hospitalized in the last month of life while 50.7% of patients died in the hospital. Results varied by local health authority from 38.3% to 69.3%. Of patients who had an ICU stay, 55.1% in the community hospitals and 59.8% in the teaching hospitals were admitted to the ICU on the day of death or the day before death. 7.5% of patients underwent a major procedure in the last 30 days of life.
Conclusions
The overall high rate, and substantial variation, in hospital care at the end of life offers the RER the opportunity to evaluate if increasing availability of palliative care, along with provider and patient education, could reduce utilization of high-cost hospital care and increase patient and family satisfaction.
Introduction
Despite advances in screening, diagnosis, and treatment, cancer remains one of the major causes of death in Europe and in Italy (1, 2). Health care for patients with cancer is a major expense for health-care systems worldwide (3). A systematic review estimated that the total cost incurred by EU health systems for cancer-related health care was €51 billion in 2009; the estimated cost in Italy was €6.9 billion (4).
Acute hospital care is the largest component of healthcare spending for patients with advanced cancer (5). In the EU countries, inpatient care accounted for 56% of cancer-related health-care costs. In Italy, inpatient care accounted for 60% of cancer-care costs (4). A number of studies have documented the high cost of medical care at the end of life (6–10). A study of US Medicare beneficiaries with poor-prognosis cancer found care to be highly intensive at the end of life, including a high volume of inpatient care and wide geographic variation (9).
In this study, we examined variation in hospital utilization and site of death for patients dying with poor-prognosis cancer in the Regione Emilia-Romagna (RER), a large region in northern Italy with a population of approximately 4.5 million. In 2012, the RER health-care system was organized in 11 Local Health Units (LHUs) with the responsibility of managing the care of their residents (11).
The use of the hospital at the end of life is more than a cost concern. Increasing attention to the quality of end-of-life care includes evaluation of the site of death (8, 12). The high proportion of patients with advanced cancer that die in the hospital contrasts with the preference of many patients to die at home with good control of pain and other symptoms or in a hospice setting (9, 13–16). Physicians who care for dying patients can help by working to understand their patients’ preferences and aligning their care accordingly (11). For policy makers, a better understanding of local-level variation in end-of-life care should help in their efforts to provide appropriate facilities and services to improve the quality and efficiency of care for patients dying with cancer.
Methods
This study was conducted under the auspices of regulation of privacy of the Emilia-Romagna region N.3 of 24 April 2006 (title: Processing of sensitive data) of act N.1 of 30 May 2014 still in force. In addition, since data analysis was performed at Thomas Jefferson University (Philadelphia, PA, USA), the Institutional Review Board (IRB) of Thomas Jefferson University evaluated this study and determined it to be exempt from IRB review.
Data
Data for this study were from the population-level, longitudinal, administrative health-care database of the residents served by the RER Health Service. This database includes demographic information for all residents (gender, birth and death dates, LHU of residence and primary care physician); hospital discharge abstract data including diagnosis and procedure codes (17) and admission and discharge dates; emergency room utilization information; outpatient pharmacy data at the individual prescription level; specialty care (laboratory, diagnostics, therapeutic procedures, rehabilitation and specialist visits); integrated home health services data (prescribed by a physician and provided by physicians, nurses, and social workers); and information on each primary-care physician in the region. Each patient has an anonymous identifier assigned by the RER so that an individual's utilization can be tracked over time without jeopardizing patient privacy.
To identify patients whose death was likely a result of cancer, we used the methods described by lezzoni et al (18) and Berke et al (19). Individuals were selected for inclusion if they died in 2012 and had at least 1 hospital admission for metastatic or “poor-prognosis” cancer within 180 days of death. Metastatic cancer was identified by ICD-9-CM codes indicating metastatic cancer, regardless of the initial site. In addition, the following types of cancer were deemed “poor-prognosis”: leukemia, cancer of the esophagus, stomach, liver, pancreas, lungs or pleura, ovary, uterine adnexa, or brain.
Outcomes
Patients were classified in the LHU of residence at the time of death. We identified patients who had spent 1 or more days in an acute-care hospital in the last 30 days of life and patients who died in the hospital. For those patients who were hospitalized in the last 30 days of life, we evaluated if they spent any time in an intensive care unit (ICU) and if they were admitted to the ICU on the day of death or the day before death. Since ICU admission is based more on the treating facility and physicians on staff at the hospital than location of patient residence, analyses of ICU use were performed at the hospital level rather than the LHU. We analyzed surgical treatment in the last 30 days of life. Major diagnostic and therapeutic procedures were classified following the Agency for Healthcare Research and Quality procedure class definitions (20). Major diagnostic procedures are those that are considered valid operating-room procedures by the Diagnosis Related Group (DRG) grouper and that are performed primarily for diagnostic purposes (e.g., 01.14 open brain biopsy), while major therapeutic procedures are performed primarily for therapeutic reasons (e.g., 52.5 partial pancreatectomy). Additionally, we considered any major procedure, that is, procedures falling into either the major therapeutic or major diagnostic class.
Statistical Analyses
Descriptive statistics were computed for all variables of interest. Age-sex-adjusted death rates were computed by direct standardization with RER residents in 2012 as the reference population; that is, the age-sex-specific rate of dying with a poor-prognosis cancer was computed for each LHU and then applied to the age-sex distribution found in the region. Ninety-five percent confidence intervals were computed as ± 1.96 times the standard error. The rates of acute hospital admissions in the last 30 days of life and the location of death were compared between LHUs of patient residence using logistic regression to control for sex and age.
Analyses of the ICU were performed at the hospital level. Hospitals were included in analyses if at least 10 decedents were admitted to the ICU in the last 30 days of life. Separate analyses were performed for community and teaching/research hospitals; variation among the hospitals of each type was tested by chi-square tests. To assess the possible influence of differences in cancer type on ICU use, we repeated the analyses excluding patients identified with leukemia.
Analyses of surgical use at the end of life were compared between patients’ LHUs of residence. Differences were assessed using logistic regression models adjusted for sex and age.
All analyses were performed in SAS version 9.3 (SAS Institute Inc.).
Results
Study Population
There were 11,470 patients in the RER who died with metastatic or poor-prognosis cancer in 2012. There were more men (56.0%) than women in the study population; 18.9% of patients were under 65 years of age at the time of death and 20.7% were over 85 years old at the time of death (Tab. I).
Age at death and sex of study population (2012)
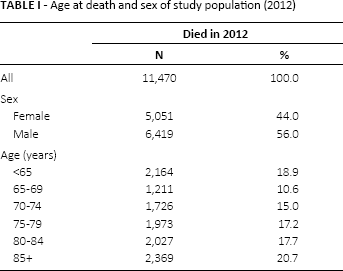
Table II displays the number of residents in each LHU and the number of residents who died of poor-prognosis cancer. Variation was observed among the LHUs in the rate of death in 2012 from poor-prognosis cancers. After adjusting for age and sex, 1 of the 11 LHUs (Modena) had a lower death rate than the region, while 1 LHU (Piacenza) had a higher death rate than the region.
Local health unit of residence and age–sex-adjusted rate of death of study population
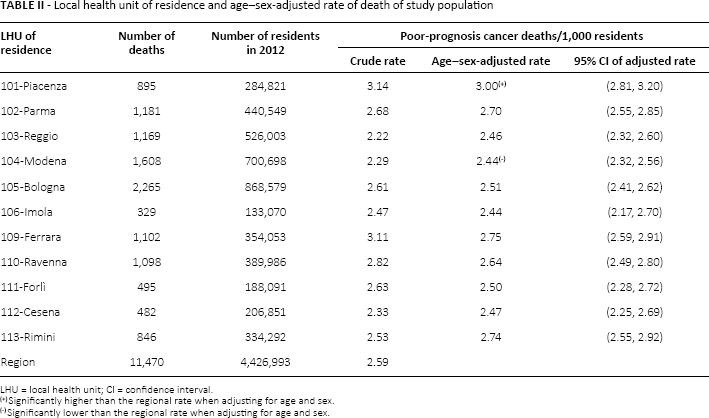
LHU = local health unit; CI = confidence interval.
Significantly higher than the regional rate when adjusting for age and sex.
Significantly lower than the regional rate when adjusting for age and sex.
Hospital Care at the End of Life
More than 3 out of 4 patients dying of cancer (77.8%) spent time as an inpatient in the last month of life, with significant variation in the rate of inpatient hospitalization in the last 30 days of life by LHU of residence (Tab. III). The lowest rates were observed in the LHUs of Fori) (69.5%) and Bologna (70.9%); the highest rates were observed in the LHUs of Cesena (84.2%), Ravenna (84.1%), Rimini (81.3%), and Modena (80.8%). Those patients who were admitted in the last month of life spent an average of 12.8 days of their last 30 in the hospital. About half (50.5%) of the study population died in the hospital. This varied from 38.0% for residents of the Forì) LHU to 69.1% for residents of the Cesena LHU.
Of the patients who were hospitalized in the last 30 days of life, there was substantial variation in the use of the ICU (Tab. IV). Among the community hospitals managed by the LHUs, 3.6% of patients who were hospitalized in the last 30 days of life spent time in ICU. In the teaching hospitals reporting directly to the region, the proportion was 5.5%. Among the teaching hospitals the rate of ICU use varied from a low of 4.6% in S. Maria Nuova (Reggio Emilia) to a high of 8.4% in Policlinico (Modena). Among the community hospitals, ICU use ranged from 3.0% among patients hospitalized at the Ospedale Ravenna to 16.8% among those hospitalized in Ospedale Civile S. Agostino Estense (Modena).
Of patients who had an ICU stay during the last 30 days of life, 55.1% in the community hospitals and 59.8% in the teaching hospitals were admitted to the ICU on the day of death or the day before death. The results were similar excluding patients with leukemia; of patients with solid tumors who had an ICU stay during the last 30 days of life, 52.9% in the community hospitals and 55.3% in the teaching hospitals were admitted to the ICU on the day of death or the day before.
Overall, 7.4% of RER residents dying with poor-prognosis cancer underwent a major procedure in the last month of life: 6.3% underwent a major therapeutic procedure while 1.8% underwent a major diagnostic procedure (Tab. V). No significant variation was observed between the LHUs with respect to major diagnostic procedures; however, the proportion of Ferrara (10.3%), Cesena (8.3%) and Parma (7.9%) residents undergoing a major therapeutic procedure or any major procedure in the last month of life was significantly higher than the regional average when adjusting for age and sex differences. Conversely, 3.9% of Rimini residents dying with poor-prognosis cancer underwent a major therapeutic procedure in the last month of life.
Hospitalization in the last month of life and site of death by local health unit of residence
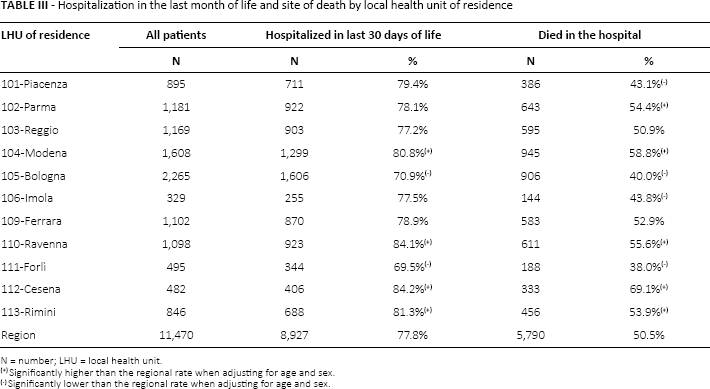
N = number; LHU = local health unit.
Significantly higher than the regional rate when adjusting for age and sex.
Significantly lower than the regional rate when adjusting for age and sex.
Intensive care unit stays in the last 30 days of life
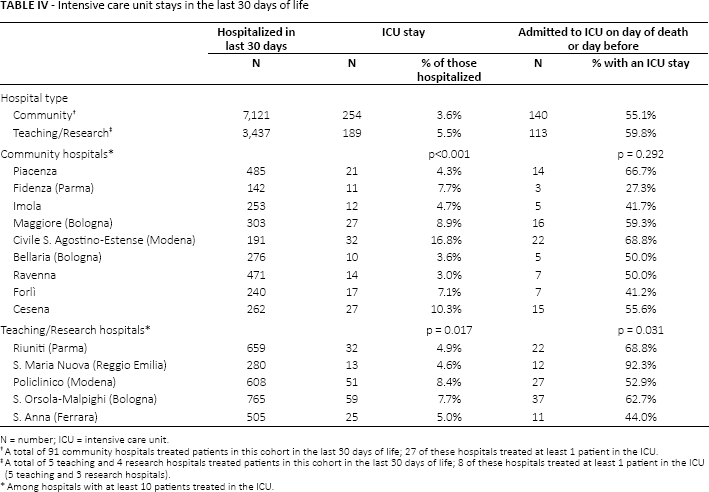
N = number; ICU = intensive care unit.
A total of 91 community hospitals treated patients in this cohort in the last 30 days of life; 27 of these hospitals treated at least 1 patient in the ICU.
A total of 5 teaching and 4 research hospitals treated patients in this cohort in the last 30 days of life; 8 of these hospitals treated at least 1 patient in the ICU (5 teaching and 3 research hospitals).
Among hospitals with at least 10 patients treated in the ICU.
Surgical treatment in the last 30 days of life
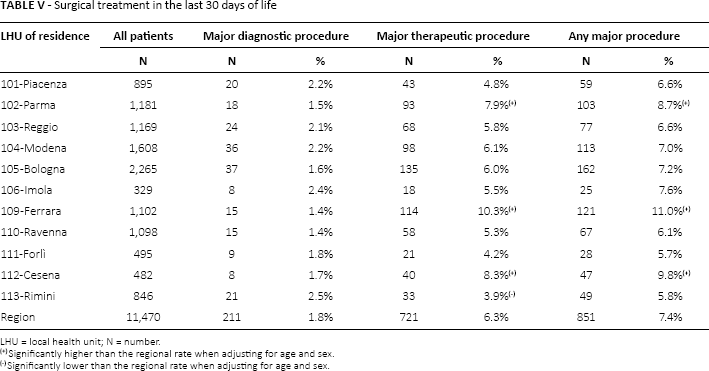
LHU = local health unit; N = number.
Significantly higher than the regional rate when adjusting for age and sex.
Significantly lower than the regional rate when adjusting for age and sex.
Discussion
In the RER, more than 3 out of 4 patients identified using administrative data as having died with poor-prognosis or metastatic cancer spent at least some time in an inpatient setting in the last month of life. Approximately half of the patients died in an acute hospital setting. While the sample selections differed, a study in Canada reported 34% of cancer patients dying in the hospital (21). A study of US Medicare beneficiaries age 65 or older reported a reduction in the proportion of cancer patients dying in an acute care hospital from 30% in 2000 to 22% in 2009 (22). While not limited to poor-prognosis cancers, a recent multinational study of site of death found 47.3% of cancer-related deaths in Italy to occur in the hospital (23). Another study in 7 developed nations reported rates of dying in an acute care facility ranging from 22.2% to 52.1% (24).
In addition to an overall high rate of hospital use at the end of life, substantial intraregional variation was observed in the rates of hospitalization and death in the hospital depending on the LHU of residence of the patient. This variation might be explained by variation in the availability of alternative palliative care services. In 2012, there were 273 hospice beds in RER, ranging from 10 in the Modena LHU to 58 in the Bologna LHU (25). In addition, home care is available in all of the LHUs of the region. RER is reviewing the relationship between the use of hospice and home health services for patients dying with cancer and admission to the hospital and location of death.
Despite the high cost of hospital care at the end of life, such care might be justified if it were beneficial or desired by patients and their families. However, a number of studies have found that more patients and their families would prefer to die at home or in a less intensive setting than an acute hospital or an ICU as long as pain and symptom control and support services are available (9). A study in Italy of primary caregivers estimated that 93.5% of those who died of cancer preferred to die at home yet found that only 57.9% did so (26).
We also observed substantial variation among hospitals in the use of the ICU among patients who were admitted to an acute-care hospital. Rates of ICU use varied from less than 4% of hospitalized patients to almost 17%. Earle et al (27) proposed a benchmark of ICU admission, multiple hospital admissions or emergency room visits in the last 30 days of life exceeding 4% as an indicator of potentially overly aggressive care at the end of life. While that study was based on a population of US Medicare patients, the Emilia-Romagna region and other Italian regions could consider the development of similar benchmarks using Italian data and experiences. In addition, over 50% of patients who had an ICU stay were admitted on the day of death or the day before death. While unmeasured differences in cancer types may affect these findings, they are unlikely to explain the large observed variation in ICU use. The ICU is a very expensive and invasive resource. High ICU utilization at the end of life may reflect an unwillingness of the medical and nursing staff to confront the death of a patient or potential pressure from patients or their families. We believe that the hospitals and the region may want to review guidelines for ICU admission for patients with cancer in the final days of life.
Variation in surgical treatment at the end of life was also observed, with more than 7% of patients undergoing a “major” operating-room procedure in the last 30 days of life. It is not clear from the data we have available if the intent of these procedures was exploratory, palliative, or curative. Review of a sample of the medical records of patients who had undergone these types of procedures at the end of life might help to assess their appropriateness.
Our study has a number of limitations. First of all, it was retrospective, starting with patients who had died and evaluating the care provided in the period before death. Some have argued in favor of prospective cohort studies which are more similar to the dilemmas faced by physicians and patients with severe diseases but unknown outcomes (28). However, Setoguchi et al (29) compared retrospective and prospective measures and concluded that they identify similar patterns of end-of-life care. We did not have access to death certificate data that could be linked to the administrative data files used in our study. With diagnostic data from outpatient encounters unavailable, we relied on hospital admissions to identify cancer cases. Our dependence on hospital discharge data may have underestimated the number of patients dying with poor-prognosis or metastatic cancer. Furthermore, differences in case mix may explain some of the observed variation between the LHUs and treating facilities. In addition, we had no ability to assess patient and family preferences.
Despite these limitations, we believe that the overall high rate and substantial variation in high-cost hospital care at the end of life for patients dying with cancer that we observed in this study offers the RER the opportunity to evaluate methods for both reducing the cost and increasing the quality of care at the end of life for patients with cancer (30). Of course, changing patterns of care at the end of life depends on the availability of alternatives to hospital care, such as hospice and home health care, as well as the preferences of patients and their families and the attitudes and practices of the oncologists and other physicians providing care to these patients.
Footnotes
Abbreviations
Financial support: This project was funded by the Agenzia Sanitaria e Sociale Regionale Regione Emilia-Romagna and Progetto PRIN “L'erogazione della prestazione medica tra diritto alia salute, principio di autodeterminazione e gestione ottimale delle risorse.”
Conflict of interest: Daniel Z. Louis is a consultant for Truven Health Analytics, Ann Arbor, MI, USA. Rita Melotti is a consultant for KCI Medical Srl, Milan, Italy, and for Covidien AG, Neuhausen am Rheinfall, Switzerland.