
Abstract
Introduction
Due to early and late failures that may occur with surgically created hemodialysis arteriovenous fistulas (SAVF), post-creation procedures are commonly required to facilitate AVF maturation and maintain patency. This study compared AVF post-creation procedures and their associated costs in patients with SAVF to patients with a new endovascularly created AVF (endoAVF).
Methods
A 5% random sample from Medicare Standard Analytical Files was abstracted to determine post- creation procedures and associated costs for SAVF created from 2011 to 2013. Medicare enrollment during the 6 months prior to and after the AVF creation was required. Patients’ follow-up inpatient, outpatient, and physician claims were used to identify post-creation procedures and to estimate average procedure costs. Comparative procedural information on endoAVF was obtained from the Novel Endovascular Access Trial (NEAT).
Results
Of 3764 Medicare SAVF patients, 60 successfully matched to endoAVF patients using 1:1 propensity score matching of baseline demographic and clinical characteristics. The total post-creation procedural event rate within 1 year was lower for endoAVF patients (0.59 per patient-year) compared to the matched SAVF cohort (3.43 per patient-year; p<0.05). In the endoAVF cohort, event rates of angioplasty, thrombectomy, revision, catheter placement, subsequent arteriovenous graft (AVG), new SAVF, and vascular access-related infection were all significantly lower than in the SAVF cohort. The average first year cost per patient-year associated with post-creation procedures was estimated at US$11,240 USD lower for endoAVF than for SAVF.
Conclusions
Compared to patients with SAVF, patients with endoAVF required fewer post-creation procedures and had lower associated mean costs within the first year.
Introduction
Among all hemodialysis access types, the arteriovenous fistula (AVF) offers longer access survival, lower mortality risk, reduced infection rate and requires fewer interventions following its successful maturation and use (1, 2). Recent literature suggests that it is common to require two or more additional procedures to facilitate maturation and maintain function after the initial AVF creation (3, 4). Despite these procedures, a substantial proportion of AVFs never become usable for hemodialysis, leaving the patient dependent on temporary central venous catheters (CVCs) for an extended time before another arteriovenous access (prosthetic arteriovenous graft [AVG]) or a new surgical AVF [SAVF]) can be created and used (5, 6). Such catheter dependence can lead to complications, such as infection. Importantly, AVFs that require facilitative procedures for maturation have poorer durability than those that do not (7, 8).
A new endovascular catheter-based system the everlinQ endoAVF System, has been developed that uses a minimally invasive method to create an AVF (endoAVF) as an alternative to the traditional open surgical approach (9, 10). The everlinQ endoAVF system creates a side-to-side anastomosis without open surgery or vessel dissection, minimizing trauma to the vessels. A prospective clinical study, the Novel Endovascular Access Trial (NEAT), has been conducted to determine the efficacy and safety of endoAVF creation in patients with stage V chronic kidney disease (CKD) who require vascular access for hemodialysis (11).
To better understand the potential economic impact of endoAVF creation, we conducted a retrospective observational study to compare the rates and associated costs of procedures performed after the initial AVF creation to facilitate or maintain AVF use between patients with the new endovascular approach (endoAVF cohort) and a propensity score- matched Medicare cohort with traditional surgical AVF (SAVF cohort).
Methods
Study design and data sources
This retrospective observational study used data combined from two sources: (i) the Centers for Medicare and Medicaid Services (CMS) 5% Medicare Standard Analytical Files (SAFs) from 2010 to 2014 and (ii) clinical trial data from NEAT, a prospective, multicenter, single arm study of 60 evaluable patients who had an endoAVF created and followed for one year (11). The CMS SAF sample contains 5% of the Medicare fee-for-service population, which were randomly selected and had every Medicare claim filed fully adjudicated. Medicare Limited Data Set SAFs Parts A and B claims use fee-for-service claims completion or final action, indicated by claim maturity, reconciliation, and validation to produce the extracts that are released and used for analysis through June 30 of the following year (12). This Medicare-derived sample comprised the traditional surgical AVF cohort (SAVF cohort).
For the endoAVF cohort (n = 60), de-identified demographic and clinical data from participants in NEAT were used. All 60 NEAT participants were included and rates were annualized per their individual follow-up times, with a mean follow-up time of 10.9 months.
The SAVF cohort was compared to the endoAVF cohort, using propensity score matching (1:1 ratio), a method successfully used in previous research with small study populations (13). Event rates of post-creation facilitative and maintenance procedures and their associated costs were then compared between the SAVF and endoAVF cohorts.
Patient inclusion and exclusion criteria
The following inclusion and exclusion criteria were applied to eligible Medicare patients for comparison to the endoAVF cohort: (i) received traditional SAVF creation procedures during 2011-2013 (Current Procedural Terminology [CPT] codes 36818, 36819, 36820, and 36821); (ii) ≥18 years of age at the time of AVF creation (index date); and, (iii) continuous enrollment in Medicare Parts A and B during the 6-month base- line period prior to the index date and the 6-month follow-up period after the index date. Patients who were enrolled in a health maintenance organization (HMO) plan at any time during the study period were excluded since the Medicare SAFs do not contain complete claims histories for HMO-type plan beneficiaries.
Baseline patient demographics and clinical characteristics
For the SAVF cohort, baseline demographic and clinical information were extracted from the Medicare SAF denominator file. Corresponding International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes were also used to extract baseline clinical information from the Medicare inpatient, outpatient, and physician Part B files except for baseline information on prior use of CVC and previously failed AVF, for which the CPT codes were used.
For the endoAVF cohort, baseline demographic and clinical information was provided by NEAT (11). Variables included age, sex, race/ethnicity, history of diabetes, hypertension, congestive heart failure (CHF), peripheral vascular disease (PVD), coronary artery disease (CAD), cerebrovascular disease (CVD), known malignancy, prior use of CVCs, and previously failed AVF.
Post-creation procedures and associated costs
For the SAVF cohort, procedural events including angioplasty, stent placement, embolization/ligation, thrombolysis, thrombectomy, pseudoaneurysm treatment, revision, distal revascularization and interval ligation (DRIL), CVC placement, AVG creation, and new surgical AVF creation were identified from Medicare outpatient and Part B claims using corresponding CPT codes (Supplementary Table I - Coding used to identify post-creation procedures from Medicare claims data - available online as Supplementary material at www.vascular-access.info). Vascular access-related infections were also examined for all patients in Medicare inpatient, outpatient, and part B files by using ICD-9-CM codes (996.62, 999.31, 999.32, 999.33).
Comparison of baseline demographic and clinical characteristics between all Medicare SAVF cohort and endoAVF cohort (pre-match)
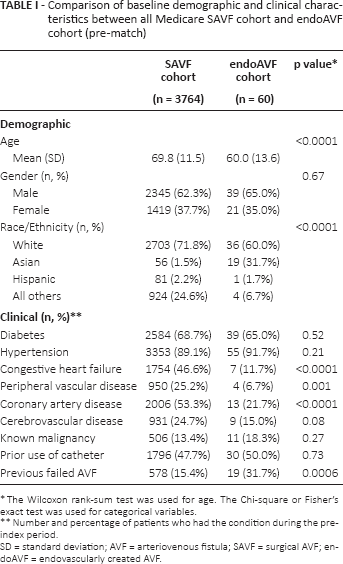
The Wilcoxon rank-sum test was used for age, The Chi-square or Fisher's exact test was used for categorical variables.
Number and percentage of patients who had the condition during the pre- index period.
SD = standard deviation; AVF = arteriovenous fistula; SAVF = surgical AVF; endoAVF = endovascularly created AVF.
For the endoAVF cohort, the information regarding post- creation procedures was extracted from the NEAT data. Costs associated with post-creation procedures were estimated using the total payment amount from payers and patients (copayment or coinsurance) for the service and adjusted to 2014 US dollars (US$) using the Medical Care component of the Consumer Price Index. The average cost for each post- creation procedure, except treatment for vascular access- related infection, was estimated based on the patient's outpatient and Part B claims. For vascular access-related infection, cost was estimated separately for inpatient and out- patient settings, according to place of treatment as recorded in the claims, since severe infection (e.g., sepsis) is typically treated in-hospital and the cost of care is higher than in out- patient settings. Costs for the endoAVF cohort were similarly estimated using Medicare payment rates to make a direct comparison of costs between the treatment cohorts.
Statistical analysis
Descriptive analyses, including means and frequencies for baseline continuous and categorical variables, respectively, were conducted for both the SAVF and endoAVF cohorts prior to propensity score matching (Tab. I). Cohort comparisons were made using Wilcoxon rank-sum tests for continuous variables and chi-square tests (or Fisher's exact tests) for categorical variables, as appropriate. Propensity score matching was used to form the standard of care comparison cohort (matched-SAVF cohort) for the endoAVF patients (14, 15). Propensity scores were estimated by logistic regression incorporating patient baseline demographic and clinical characteristics in a 1-to-1 ratio using a local optimal algorithm for the base case. Patients’ baseline characteristics were again compared between the matched-SAVF cohort and the endoAVF cohort using Wilcoxon rank-sum tests and chi-square/Fisher's exact tests to ensure the balance of matching was achieved (Tab. II). The rates of post-creation procedures for the follow-up period were estimated per patient-year (PY). The event rates were compared between the propensity score matched-SAVF cohort and endoAVF cohort. The average cost for each type of procedure was associated with the event rates and formed the basis for differences in costs associated with post-creation procedures between the matched-SAVF and endoAVF cohorts. Several sensitivity analyses were also conducted to assess the impact of follow-up length and matching ratio on study results as follows: (i) 6-month comparison of matched-SAVF data with endoAVF data censored at 6 months post endoAVF creation; (ii) restricting the analysis to Medicare patients who received only direct arteriovenous anastomosis (CPT 36821), as that is the code for a direct arteriovenous anastomosis as opposed to patients who received an arteriovenous anastomosis using a transposed vein (CPT codes 36818, 36819, and 36820); (iii) varying propensity score matching ratios for the SAVF cohort (1 endoAVF:2 SAVF; 1 endoAVF:3 SAVF; 1 endoAVF:5 SAVF). P values <0.05 were considered statistically significant. All statistical analyses were performed using SAS 9.3 (Cary, NC, USA).
Comparison of baseline demographic and clinical characteristics between 1:1 matched Medicare SAVF cohort and endoAVF cohort (post-propensity score matching)
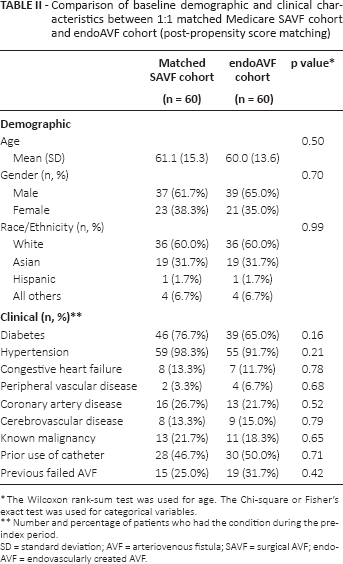
The Wilcoxon rank-sum test was used for age, The Chi-square or Fisher's exact test was used for categorical variables.
Number and percentage of patients who had the condition during the pre- index period.
SD = standard deviation; AVF = arteriovenous fistula; SAVF = surgical AVF; endoAVF = endovascularly created AVF.
Results
A total of 3764 adult Medicare patients with SAVF met the inclusion criteria for propensity score matching and were matched to 60 patients with endoAVF from NEAT (Tab. I). Post-matching, baseline demographic and clinical characteristics were balanced between the matched-SAVF and endoAVF cohorts (Tab. II).
The total procedure rate for the matched-SAVF cohort was 3.43/PY and for the endoAVF cohort was 0.59/PY (p<0.05, Tab. III). Compared with SAVF, event rates (per PY) for endoAVF were lower (all p<0.05) for angioplasty (0.93 vs. 0.04), thrombectomy (0.20 vs. 0.04), catheter placement (0.43 vs. 0.11), AVG creation (0.07 vs. 0.02), new surgical AVF creation (0.30 vs. 0.11), and vascular access-related infections (1.23 vs. 0.02) (Fig. 1). Post-creation procedures demonstrated an average cost of US$13,033 for SAVF and US$1794 for endoAVF (Tab. III). The endoAVF cohort had an average post-creation procedure- related cost that was US$11,240 per PY lower than the SAVF cohort. When the analysis was performed using only Medicare patients whose index event was direct arteriovenous anastomosis (CPT 36821) versus the endoAVF cohort, results did not differ statistically from the primary analysis (data not shown).
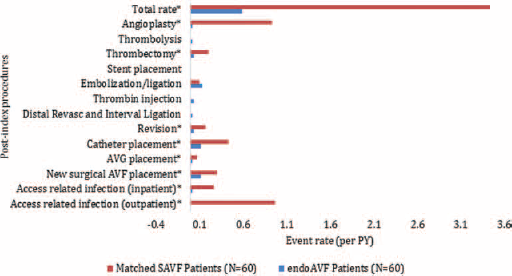
Post-matching comparison of post-creation procedure rates (per PY) for SAVF cohort and endoAVF cohort.
Average cost for each type of post-creation intervention and estimated cost savings per patient-year (PY) for endoAVF cohort when compared to matched SAVF cohort
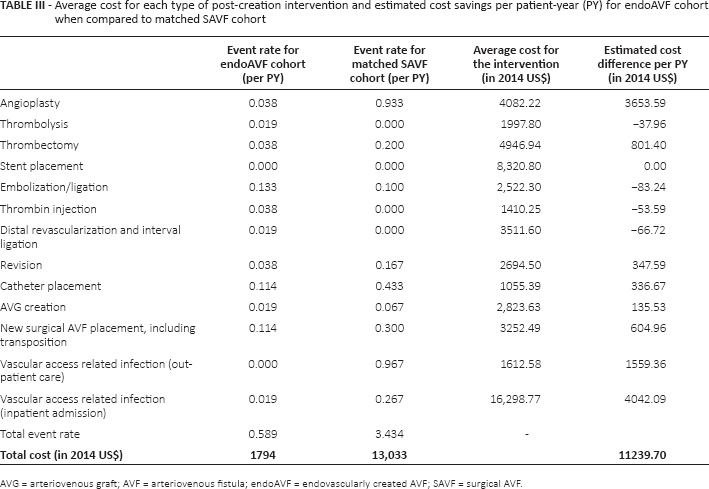
AVG = arteriovenous graft; AVF = arteriovenous fistula; endoAVF = endovascularly created AVF; SAVF = surgical AVF.
A sensitivity analysis with endoAVF patients’ data censored at 6 months was conducted to assess the influence of follow-up length on the study results since the endoAVF cohort had a longer mean follow-up time (10.9 months) compared with the SAVF cohort (6 months). Results from this sensitivity analysis demonstrated a total event rate of 3.43/PY for the matched-SAVF cohort, in comparison with 0.78/PY in the endoAVF cohort (p<0.05). Compared with the matched SAVF cohort, the estimated average procedure- related cost was US$10,533 per PY less for the endoAVF cohort (Tab. IV).
Event rates comparison and estimated cost savings per patient-year (PY) with 6-month censored endoAVF follow-up
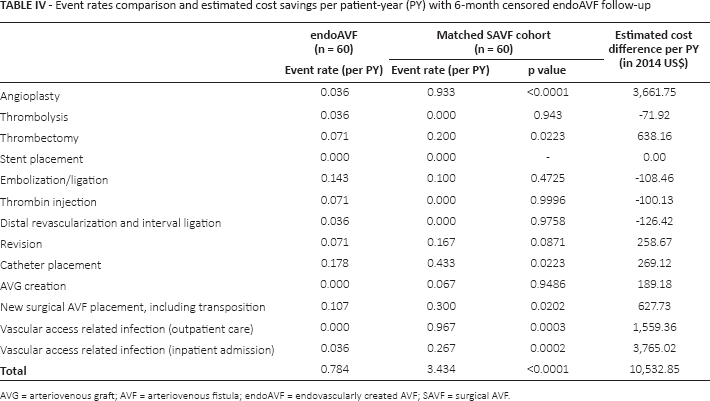
AVG = arteriovenous graft; AVF = arteriovenous fistula; endoAVF = endovascularly created AVF; SAVF = surgical AVF.
The additional sensitivity analyses that varied the base case analysis from 1:1 matching to 2:1, 3:1, and 5:1 matchings indicated that balance was achieved in all baseline characteristics post-matching, except for race/ethnicity in the 5 to 1 matching scenario. All matchings demonstrated similar results for procedural event rates for the matched-SAVF cohorts and consistently lower costs for the endoAVF cohort (data shown in Supplementary Table II - Event rates and estimated cost savings per patient-year (PY) for NEAT cohort when compared to different matched Medicare cohorts - available online as Supplementary material at www.vascular-access.info).
Discussion
When compared with traditional SAVF, patients who had an endoAVF created had significantly lower rates of post- creation procedures to facilitate maturation and/or maintain patency. This overall reduction in post-creation procedures in the first year was associated with lower total procedural costs per PY. Due to the recent innovation of endoAVF, no prior endoAVF costing studies exist for comparison. Within the surgical AVF literature, there is also a paucity of economic studies evaluating different AVF anastomotic techniques that may have shown reduced costs associated with AVF creation and maintenance (16).
The reduced post-creation procedure rate observed in the endoAVF cohort may be related to the lack of surgical trauma to the vessels, i.e., maintenance of the vasa vasorum of the vessels, and improved hemodynamics with a consistent side- to-side anastomosis (17–19). This may potentially result in improved physiologic maturation of the endoAVF and fewer subsequent required procedures. Over 90% of the endoAVFs in NEAT reached physiologic maturation and 67% of endoAVFs were routinely used for dialysis with 2-needle cannulation. The endoAVF usability of 67% compares with the 40%-70% rates reported in the surgical AVF literature (9, 20). The lower rate of procedures to facilitate maturation, such as the use of angioplasty, stenting, and thrombectomy, reflected the low complication and early thrombosis rate seen in NEAT and the high physiologic endoAVF maturation observed (11).
There are several strengths of this study, including the use of multiple sensitivity analysis in propensity score matching, which showed consistent results to select a comparator SAVF cohort for patients with endoAVF. Propensity score matching reduces confounding by including only patients who were comparable in demographic and clinical characteristics that are associated with AVF outcomes and the need for post-creation procedures (6, 21). Age, sex, and race/ethnicity have been routinely used in adjusting heterogeneity in patient populations for AVF outcomes studies (22, 23). Prevalence of diabetes and other patient comorbidities, including hypertension, CHF, PVD, CAD, CVD, and known malignancy, have also been associated with vascular access outcomes (24–31). The patients’ prior catheter use and previously failed AVF may contribute to AVF clinical outcomes as well (26). Our study included these factors in matching the SAVF and endoAVF cohorts. A range of relevant procedures was compared and multiple sensitivity analyses were conducted, which consistently demonstrated fewer post-creation AVF procedures and lower estimated costs with endoAVF (base case and sensitivity analyses ranged from US$10,533 to US$11,501 per PY (Supplementary Table II - Event rates and estimated cost savings per patient-year (PY) for NEAT cohort when compared to different matched Medicare cohorts - available online as Supplementary material at www.vascular-access.info).
There are also several limitations to this study. First, for Medicare patients with SAVF, post-creation procedures were identified and rates were calculated based on patients’ Medicare claims. However, the presence of a procedure or diagnostic code on a medical claim does not guarantee the presence of a procedure or medical condition unless they are validated against medical charts; this validation was not conducted for this study. Similarly, the absence of a code from a patient's claims does not necessarily indicate that the procedure or condition did not occur. Since the primary purpose of a procedure or diagnostic code in a claims database is for billing purposes rather than for clinical research, it is possible that codes may have been incorrectly assigned. However, recent studies have demonstrated accuracy in using key elements from administrative claims data for vascular access research (32). Additionally, the 5% random sampling of the Medicare population would largely eliminate any bias resulting from systematic coding errors.
Second, post-creation procedure-related costs were estimated based on Medicare inpatient, outpatient, and Part B claims and did not include any pharmacy costs or costs associated with diagnostic procedures. However, these were also excluded in NEAT. Third, the analysis examined only the most common procedures after the initial AVF creation; thus, a patient could have experienced less common interventions. However, we believe this would have been infrequent and that the items included in the current analysis are comprehensive and representative for the purposes of the study.
Despite the use of propensity score matching, residual confounding is possible. For example, the NEAT population is comprised of individuals from Canada, Australia, and New Zealand. These populations may differ from the US comparison cohort in unmeasured ways that propensity score matching does not address (e.g., process issues, such as use of multidisciplinary care).
Last, the pre-dialysis status could not be determined in the Medicare SAVF cohort. In NEAT, approximately half of the participants were pre-dialysis and therefore may have required fewer post-creation AVF procedures. While we cannot properly account for this, we methodologically tried to “even the field” by simulating a pre-dialysis-like state in the SAVF dialysis cohort. The propensity score matching specifically matched those SAVF patients without a prior CVC or AVF in the 6 months prior to AVF creation to NEAT pre-dialysis endoAVF patients. However, we recognize this may not directly capture whether a patient was pre-dialysis or dialysis at the time of the SAVF creation in the SAVF cohort.
Conclusions
The rates of post-creation procedures were found to be significantly lower in patients who had AVF created by an endovascular approach (endoAVF) compared with the traditional surgical approach. The associated average cost of procedures to attain and maintain the AVF in the first year following AVF creation was lower in the endoAVF cohort compared with the SAVF cohort. Longer follow-up of endoAVF clinical outcomes and their economic impact will be insightful and important for its wider adoption.
Footnotes
Financial support: Funding for this study was provided by TVA Medical Inc.
Conflict of interest: SY is a former employee of Quorum Consulting, Inc. RJA is an employee of Quorum Consulting, Inc. DR and MG have equity and are consultants for TVA Medical Inc. CL was a consultant for TVA for this economic study.