
Abstract
Objectives:
The aim of the present study was to perform cost-effectiveness and budget impact analyses comparing endovascular arteriovenous fistula creation to surgical arteriovenous fistula creation in hemodialysis patients from the National Healthcare Service (NHS) perspective in Italy.
Methods:
A systematic literature review has been conducted to retrieve complications’ rates after arteriovenous fistula creation procedures. One study comparing endovascular arteriovenous fistula creation, performed with WavelinQ device, to the surgical approach through propensity score matching was preferred to single-arm investigations to execute the economic evaluations. This study was chosen to populate a Markov model to project, on a time horizon of 1 year, quality adjusted life years and costs associated with endovascular arteriovenous fistula (WavelinQ) and surgical arteriovenous fistula options for both cohorts of incident and prevalent hemodialysis patients.
Results:
For both incident and prevalent hemodialysis patients, endovascular arteriovenous fistula creation, performed with WavelinQ, was the dominant strategy over surgical arteriovenous fistula approach, showing less cost and better patients’ quality of life. Compared to the current scenario, progressively increasing utilization rates of WavelinQ over surgical arteriovenous fistula creation in the next 5 years in incident hemodialysis patients are expected to save globally 30–36 million euros to the NHS.
Conclusion:
Endovascular arteriovenous fistula creation performed with WavelinQ could be a cost-saving strategy in comparison with the surgical approach for patients in hemodialysis. Future studies comparing different devices for endovascular arteriovenous fistula creation versus the surgical option would be needed to confirm or reject the validity of this preliminary evaluation. In the meantime, decision-makers can use these results to take decisions on the diffusion of endovascular procedures in Italy.
Keywords
Introduction
Globally, there are more than two million patients undergoing hemodialysis (HD) treatments. 1 To receive this therapy, many patients depend on a permanent vascular access. 2 Autogenous arteriovenous access, created by anastomosing a native artery and vein to create an arteriovenous fistula (AVF), is the preferred choice for long-term HD since it is associated with lowest incidence of morbidity and mortality, best long-term primary patency rate, and fewest complications, such as infection or clotting, compared to all other access choices like arteriovenous graft (AVG) or central venous catheter (CVC). 3
For HD patients, blockages created by repeated access or narrowing of the blood vessel (restenosis) are a common problem and hinder treatment. Problems with vascular access are an important cause of morbidity and mortality in HD patients. In the United States, it has been estimated that US$1 billion per year is spent on vascular access and its complications. 4 Some patients require up to eight reinterventions per year to maintain AVF function. 5 For patients undergoing HD for kidney failure, who already spend a significant portion of their time undergoing dialysis and other treatments, repeated reinterventions to maintain AV access can be an added burden.
Despite significant developments during the past years, outcomes of surgical arteriovenous fistulas (SAVFs) are still suboptimal. Complications, such as thrombosis, occur in 20% of cases, and 20%–60% of AVFs fail to mature. 6 –8 A successful fistula requires an average of two additional catheter-based procedures to facilitate maturation, leading to delays until usable access is available. 9
At present, two endovascular catheter-based systems, the WavelinQ™ 4F EndoAVF System (DB—Becton, Dickinson and Company, NJ, USA) and Ellipsys® Vascular Access System (Avenu Medical, San Juan Capistrano, CA, USA), have been developed to apply a minimally invasive method to create an AVF as an alternative to the traditional open surgical approach. 10 Ellipsys is a thermal resistance device that enables arteriovenous anastomosis of the proximal radial artery and perforating vein while WavelinQ works slightly differently as it is a dual catheter-based system that creates an AVF between arteries (typically the ulnar artery/radial artery) and veins (ulnar vein/radial vein) of the proximal forearm, offering two anatomic options for AVF creation. Endovascular technology, which allows fistula creation with minimal vessel trauma, showed encouraging outcomes with high technical success rates, low reintervention and failure rates, and good usability for HD. 11
The overall aim of the present study was to measure the added value of endovascular catheter-based approach for the endovascular creation of AVF (endoAVF) with WavelinQ system in HD patients and to compare it to the surgical approach (SAVF), through a health technology assessment, to inform decision-makers in due course on the choices offered to HD patients in the context of access creation. In particular, the aim of the present study was to perform cost-effectiveness and budget impact analyses comparing endoAVF by WavelinQ to SAVF in HD patients from the Italian Healthcare Service perspective.
Methods
Retrieval of clinical efficacy data
With the aim of retrieving data to populate a cost-effectiveness model, a systematic literature review has been conducted for endoAVF and SAVF and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 12 The search considered randomized controlled trials (RCTs), prospective clinical trials, and observational studies. While the latter have some limitations compared with RCTs, such studies can offer valuable real-world evidence on the use of the technology. 13,14
A comprehensive search strategy to scan the four items within the PICO (Population: HD patients needing native AVF creation, Intervention: endoAVF, Comparator: SAVF, and Outcomes) framework has been designed and used in June 2019 to search PubMed and Web of Science scientific databases.
As regards the outcomes, the search focused mainly on complications after clinical interventions since they are directly linked with healthcare resource consumption (and consequently costs) to perform the economic evaluation. Studies reporting data on patients’ quality of life have been searched as well.
Studies were considered if published in English and if they referred to an adult population. No restrictions were imposed on the location of the study, while the year of publication was limited to the last 10 years, considering the relatively recent development of the endoAVF approach. Case reports, letters, comments, editorials, and reviews were excluded. Two investigators (C.R. and M.T.) independently performed the screening on titles and abstracts, first, and full-texts later. Studies were excluded based on titles and abstract screening according to the following exclusion criteria: (a) no abstract available, (b) specific focus on pediatric or adolescent population, and (c) focus on interventions different from vascular access creation. Full-text articles were retrieved and reviewed by the same two investigators. Articles were excluded if they did not provide any data on rates of complications or quality of life. All search results were extracted in MS Excel software. Details on the search strategy are reported in the Appendix, while Table 1 reports the inclusion criteria.
Inclusion criteria for the systematic literature review.
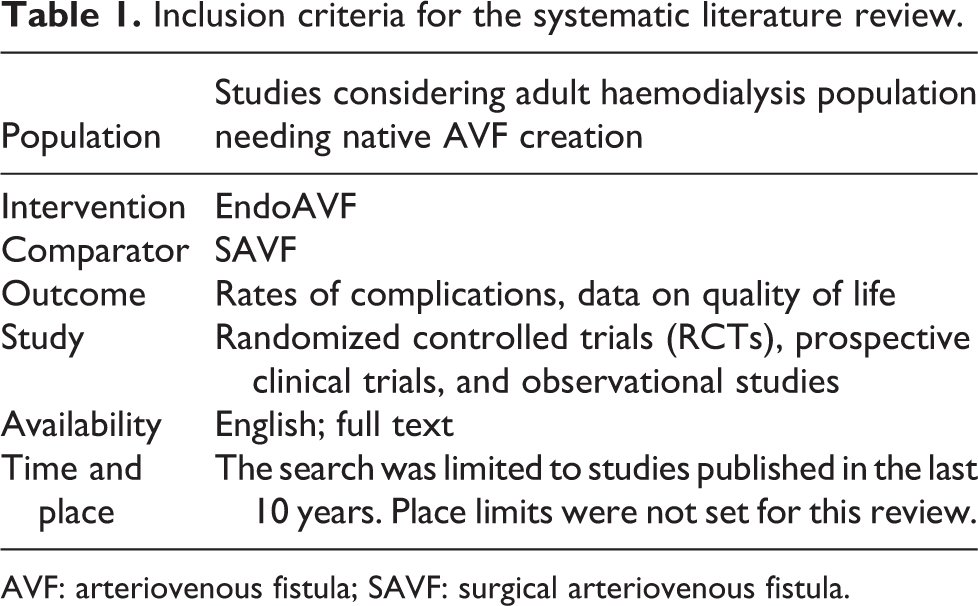
AVF: arteriovenous fistula; SAVF: surgical arteriovenous fistula.
Twenty-six studies have been found reporting data on the number of events following fistula creation. None of these studies reported data on patients’ quality of life useful for cost-effectiveness analysis. A summary of main data is reported in Table 2 (see Supplemental Table 1 for detailed data).
Summary of study characteristics.
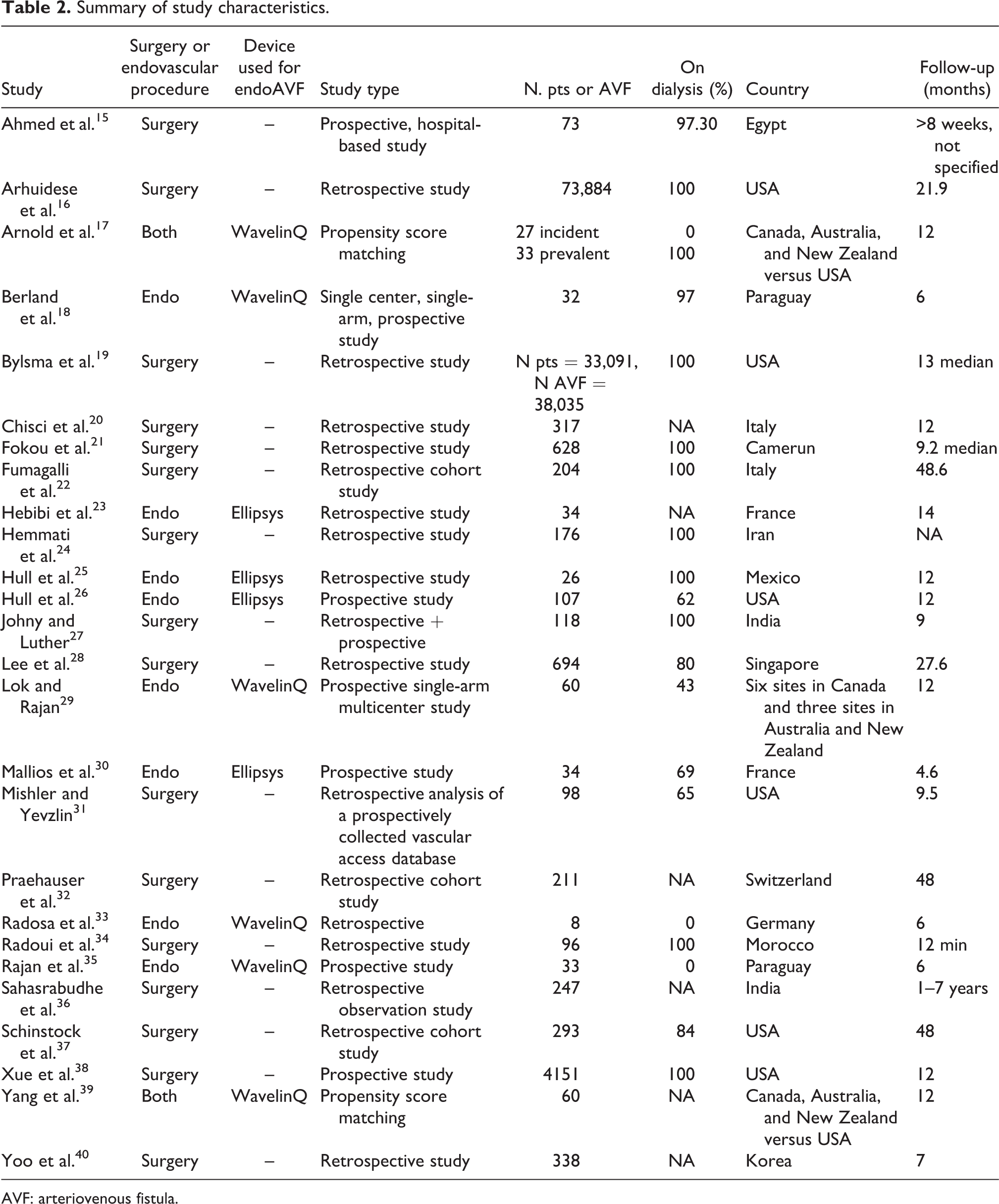
AVF: arteriovenous fistula.
Two studies, 17,39 which considered WavelinQ device, directly compared the two AVF creation procedures through propensity score matching (PSM) technique. On the remaining single-arm studies, sixteen, mainly retrospective, reported data on SAVF, while eight studies focused on endoAVF (four on WavelinQ and four on Ellipsys). The follow-up ranged from 4.6 to 84 months and the number of studied patients ranged from 73 to 33,091 for SAVF and from 8 to 107 for endoAVF.
Because comparative studies based on PSM have been considered the ones with higher data quality compared to single-arm investigations, these studies were evaluated for the model development for the economic evaluations. In particular, the first published study 39 considered a random sample from Medicare to determine post-creation procedures and associated costs for SAVF and compared them with data on endoAVF with WavelinQ from the Novel Endovascular Access Trial (NEAT). 29 However, information on incident and prevalent status could not be evaluated with Medicare. The second study 17 considered endoAVF (WavelinQ) data from the same NEAT trial, while data on SAVF were retrieved from the United States Renal Data System (USRDS). This study has carried out the comparative analysis between WavelinQ and surgical procedure by distinguishing incident and prevalent dialysis patients and it has been chosen as the source for developing the model in our study in order to perform the economic evaluations.
Target population and events for the comparison between endoAVF (WavelinQ) and SAVF
Patients in the USRDS database were 13,265 adults who performed SAVF creation and enrolled in Medicare and followed for 6 months before and for 6 months after the AVF creation date. The endoAVF cohort considered the 60 participants enrolled in the NEAT study. Patients were defined as incident if they were not on dialysis at the time of AVF creation; all USRDS incident patients received dialysis.
A 1-1 PSM has been performed to compare event rates, intervention-free survival, and costs between endoAVF and SAVF cohorts, leading to a comparison of 27 and 33 for incident and prevalent patients, respectively. 17 Table 3 reports the rates of events distinguished by cohort and population.
Event rates per patient year for incident and prevalent patients (time horizon of 1 year).
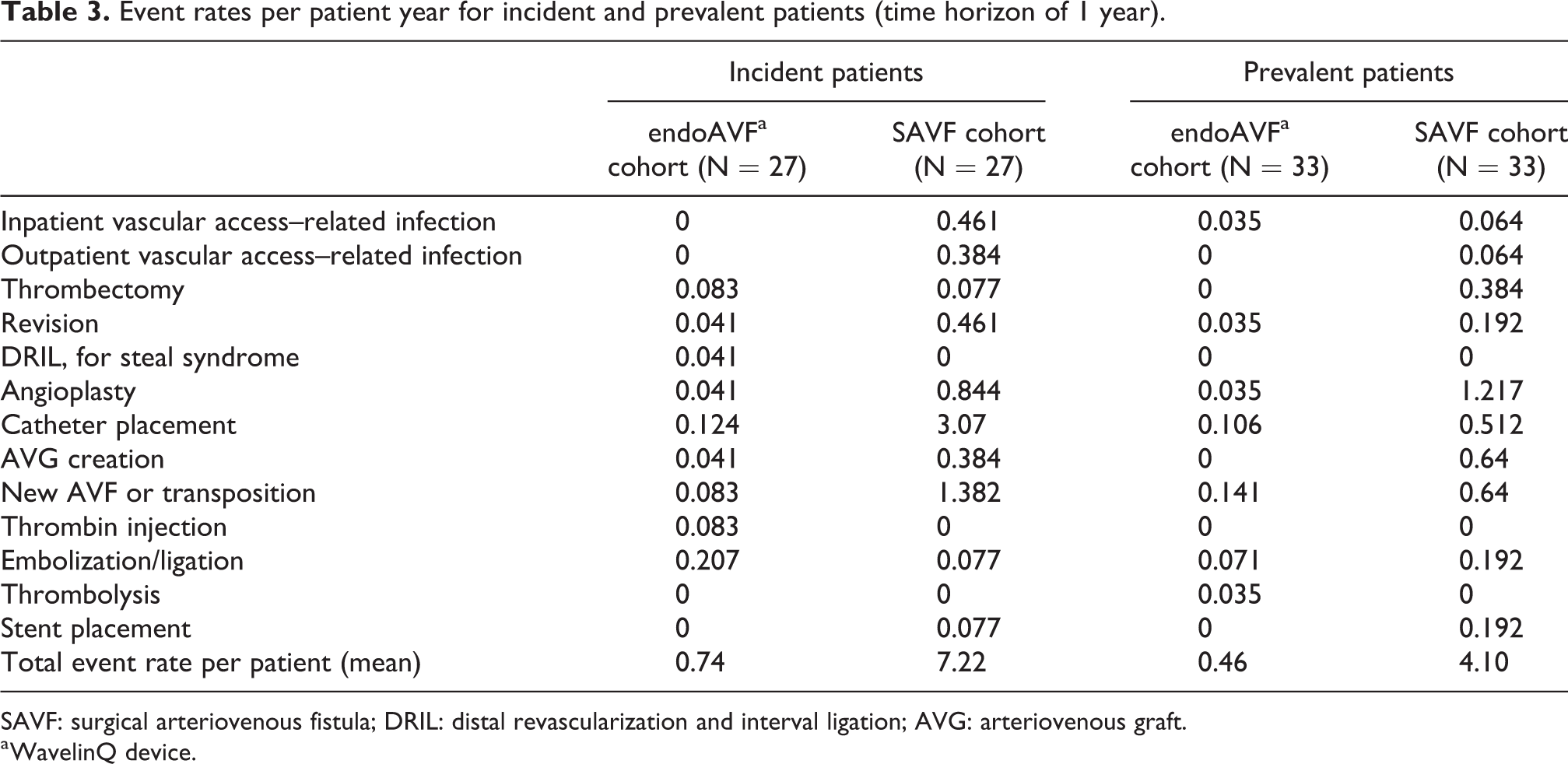
SAVF: surgical arteriovenous fistula; DRIL: distal revascularization and interval ligation; AVG: arteriovenous graft.
a WavelinQ device.
The model
A Markov model has been selected for this economic evaluation. 41 A Markov model comprises a finite set of health states in which an individual can be found. The states are such that in any given time interval, the individual will be in only one health state. In the original graphical representation of Markov models, sometimes referred to as a “bubble diagram”, each state is represented with a circle, while arrows represent transitions from one state to another. Movements among states are defined by transition probabilities. Transitions usually happen at fixed time intervals (Markov cycle). A transition arrow pointing back to the state from which it originates indicates that it is possible for an individual to remain in the same state for more than one cycle. Rewards are assigned to each health state and earned at the end of each cycle; in our case, the model projects quality adjusted life years (QALYs) and costs associated with endoAVF (WavelinQ) and SAVF for both incident and prevalent cohorts.
The health states considered in the implemented model were “native AVF, no events” and “complications” (Figure 1). A hypothetical cohort of patients starts the Markov process in the “native AVF no events” state. Patients may stay in the “native AVF no events” state or, in case of events, may move to the “complications” state. Transition probabilities between health states for incident/prevalent patients undergoing endoAVF or SAVF have been estimated from freedom from intervention curves presented in Arnold et al. 17 (Supplemental Table 2). Exponential functions have been fitted for the event-free curves emerging from the two matched cohorts according to treatment strategy. A Markov cycle length of 1-month and a horizon of 1 year have been chosen for baseline analysis.
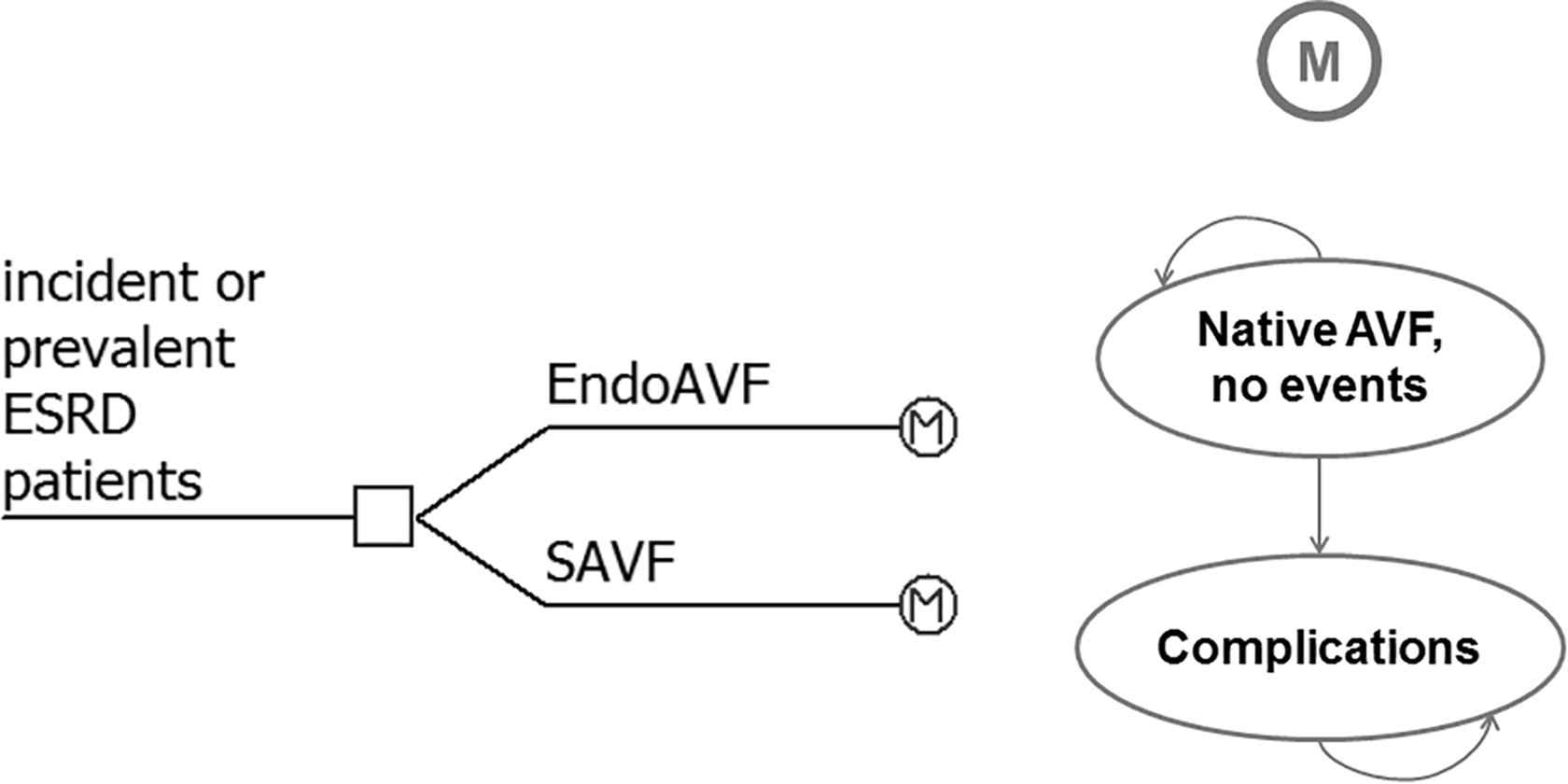
Model representation (M=Markov model).
The model was implemented using TreeAge Software (TreeAge Software, Inc., Williamstown, MA, USA).
Healthcare resource consumption and costs
Direct healthcare resource consumption (direct costs) was considered in the model (Eur, 2019). Data on costs were obtained from national diagnosis-related groups (DRGs) reimbursement rates to reflect the Italian Healthcare System perspective (Table 4). For the endovascular procedure with WavelinQ, we assumed it can be performed in a day-hospital (DH) setting, while for the surgical one, the standard DRG tariff has been applied. Angioplasty has been considered as a DH procedure.
DRGs reimbursement rates for the different procedures.
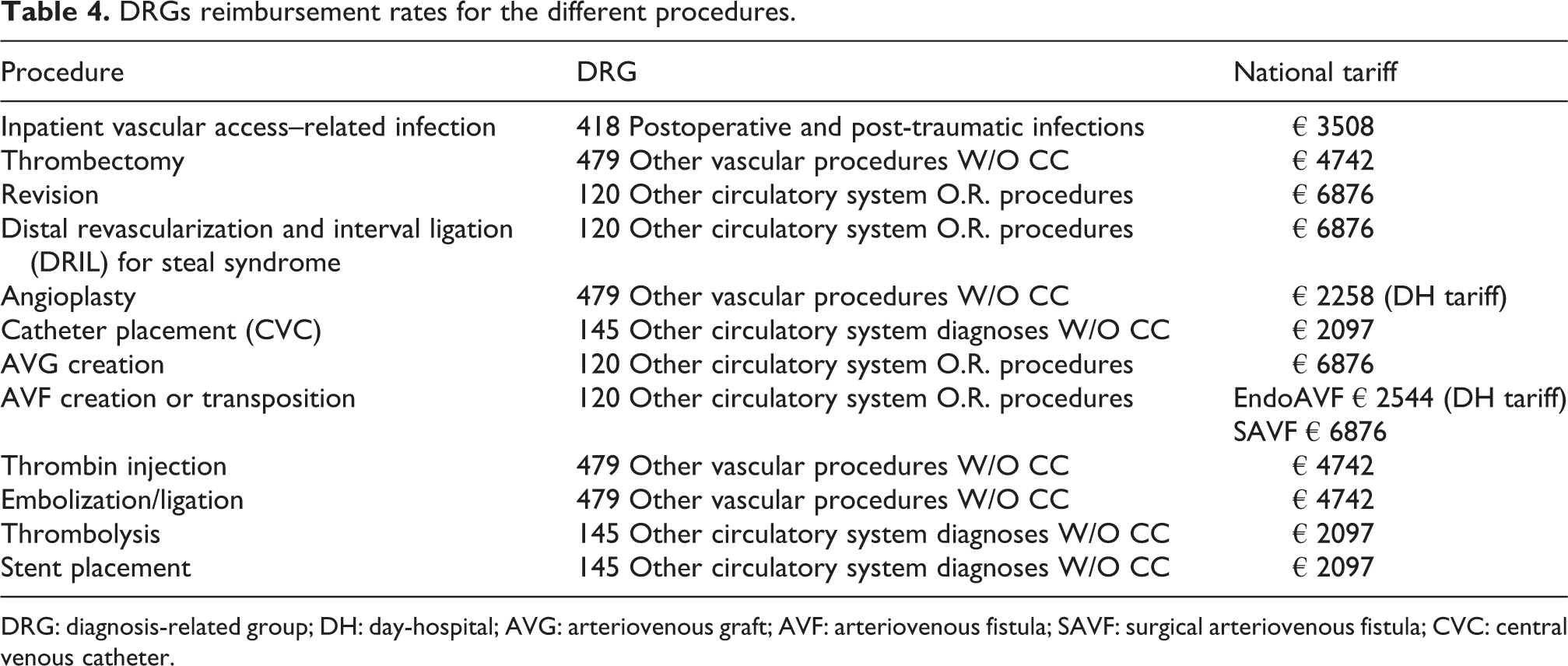
DRG: diagnosis-related group; DH: day-hospital; AVG: arteriovenous graft; AVF: arteriovenous fistula; SAVF: surgical arteriovenous fistula; CVC: central venous catheter.
Quality-of-life estimates
Health-related quality-of-life measures were not available from Arnold et al. 17 The utility coefficients for the main events have been retrieved from another publication, obtained by the systematic literature search, involving the same authors 42 which reported utility values for AVF (0.614), AVG (0.566), and CVC (0.538). Because the reference study did not report the duration of events experienced by the patients, we calculated a mean utility value for the health state “complications” based on the reported frequencies of events. We assumed that events related to the management of the fistula (e.g. thrombolysis, thrombectomy) caused a lowering of the patients’ quality of live for a limited time, and for this reason, these events were not accounted in the model. This approach led to the estimation of a utility coefficient of 0.568 and 0.562 for the “complication” health state for incident patients undergoing endoAVF and SAVF, respectively. The values for prevalent patients’ cohort were 0.581 and 0.575, respectively. A utility coefficient of 0.614 has been applied to the “native AVF, no events” health state.
Cost-effectiveness analysis (CEA)
Costs and QALYs for the considered strategies were estimated to calculate the incremental cost–utility ratio (ICUR) of endoAVF (with WavelinQ device) versus SAVF. Considering the limited time horizon for the analysis (1 year), QALYs and costs were not discounted. Transition probabilities, costs, and utilities were entered into the model along with a distribution: beta for utilities and transition probabilities and gamma for costs (a standard deviation of 10% of the baseline value has been considered for all the distributions). Deterministic and probabilistic sensitivity analyses (PSA) were performed to test the robustness of the model. In the latter case, second-order Monte Carlo simulations (10,000 iterations) were conducted for incident and prevalent cohorts to take into account parameters variability; resulting scatterplots were plotted onto a cost-effectiveness plane.
Budget impact analysis
A budget impact model has been developed based on the cost-effectiveness analysis (CEA) model to evaluate the expected changes in the expenditure for the Italian Healthcare Service in the hypothesis of an increased utilization of endoAVF with WavelinQ in place of SAVF for incident HD patients.
The annual incidence of HD in Italy accounts for about 9500 patients, 43 of which about 68% can be considered for AVF creation (6460). 44
As the use in Italy of WavelinQ is at the beginning, the current scenario of patients’ distribution between the two alternative creation procedures considered 100% of use of SAVF. Future scenarios considered increased proportions of use of WavelinQ over SAVF of 0.5%, 2%, 4%, 6%, and 8% for the following 5 years. The model applies the variations of the market share to the new incident cohorts (naive treatments), without considering the prevalent cohort. Constant incident cohorts were considered in the analysis.
The costs for current and future scenarios were estimated by multiplying yearly costs of each option by the proportion of the eligible population using that option and by the number of patients in the eligible population, taking into account subsequent yearly incident cohorts. As the focus was on the expected budget at each point in time, the financial streams were presented as undiscounted costs. 45
Results
CEA results
Considering a time horizon of 1 year, for WavelinQ, the average QALYs were estimated to be 0.607 for incident patients and 0.608 for prevalent patients; for SAVF, the average QALYs were 0.589 and 0.595 for the two populations considered. The mean costs per patient for WavelinQ were estimated to be 5722€ and 3978€ for incident and prevalent patients, respectively, while for SAVF costs of 33,041€ and 24,178€ were obtained, respectively.
For both incident and prevalent cohorts, endoAVF with WavelinQ was the dominant strategy (i.e. less costly and with higher QALYs) compared with SAVF. The model results for the two scenarios are summarized in Table 5.
Model results for incident and prevalent patients (time horizon 1 year).
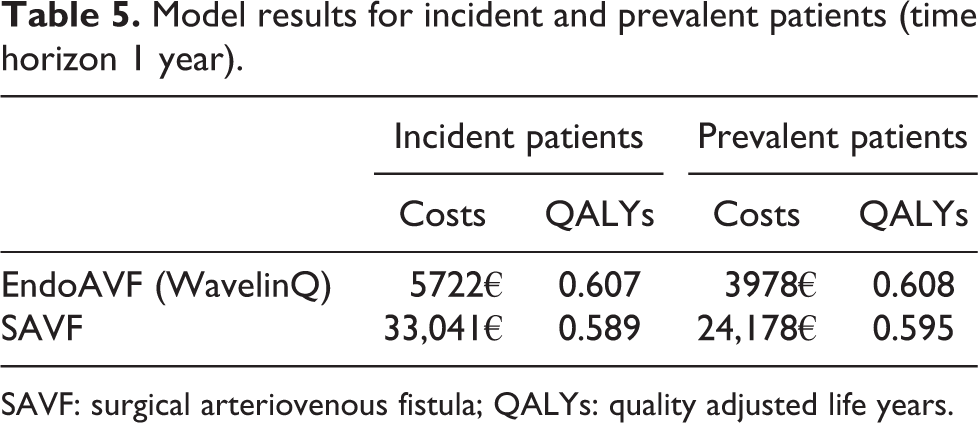
SAVF: surgical arteriovenous fistula; QALYs: quality adjusted life years.
A scenario analysis has been conducted by considering the standard DRG reimbursement for both WavelinQ and SAVF procedures. In this case, the mean costs per patient for WavelinQ were 10,414€ and 8920€ for incident and prevalent patients, respectively. These costs were still lower than the corresponding ones for SAVF and, for both cohorts, endoAVF with WavelinQ was confirmed as the dominant strategy.
The plots of incremental costs versus incremental QALYs obtained from the Monte Carlo simulations are shown in Figure 2 (a: incident patients; b: prevalent patients). Dotted lines represent a theoretical cost-effectiveness threshold of 50,000€/QALY; the totality of points lie below this line for incident and prevalent cohorts, respectively.
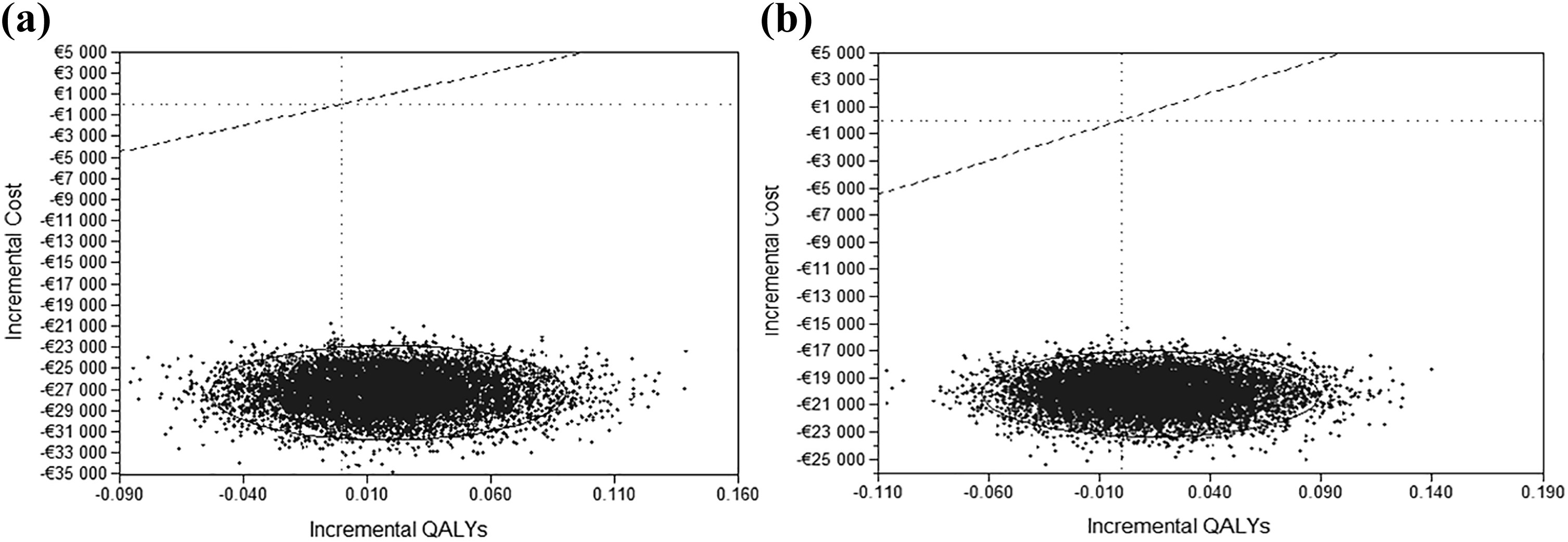
Scatterplot of incremental costs versus incremental QALYs obtained from Monte Carlo simulations for the comparison endoAVF versus SAVF for incident (a) and prevalent (b) cohorts.
Budget impact analysis
In comparison with the current scenario (year 0), by progressively increasing endoAVF (WavelinQ) utilization rates for incident HD patients to 0.5%, 2%, 4%, 6%, and 8%, it would be possible to save 882,404€, 3,529,615€, 7,059,230€, 10,588,844€, and 14,118,459€ for 1-, 2-, 3-, 4-, and 5-year scenarios, respectively, yielding total savings of about 36 million euros over the next 5 years (Table 6). In the scenario that considered the standard DRG tariff for both WavelinQ and SAVF procedures, the total savings on a time horizon of 5 years would be about 30 million euros.
Budget impact analysis for incident HD patients.
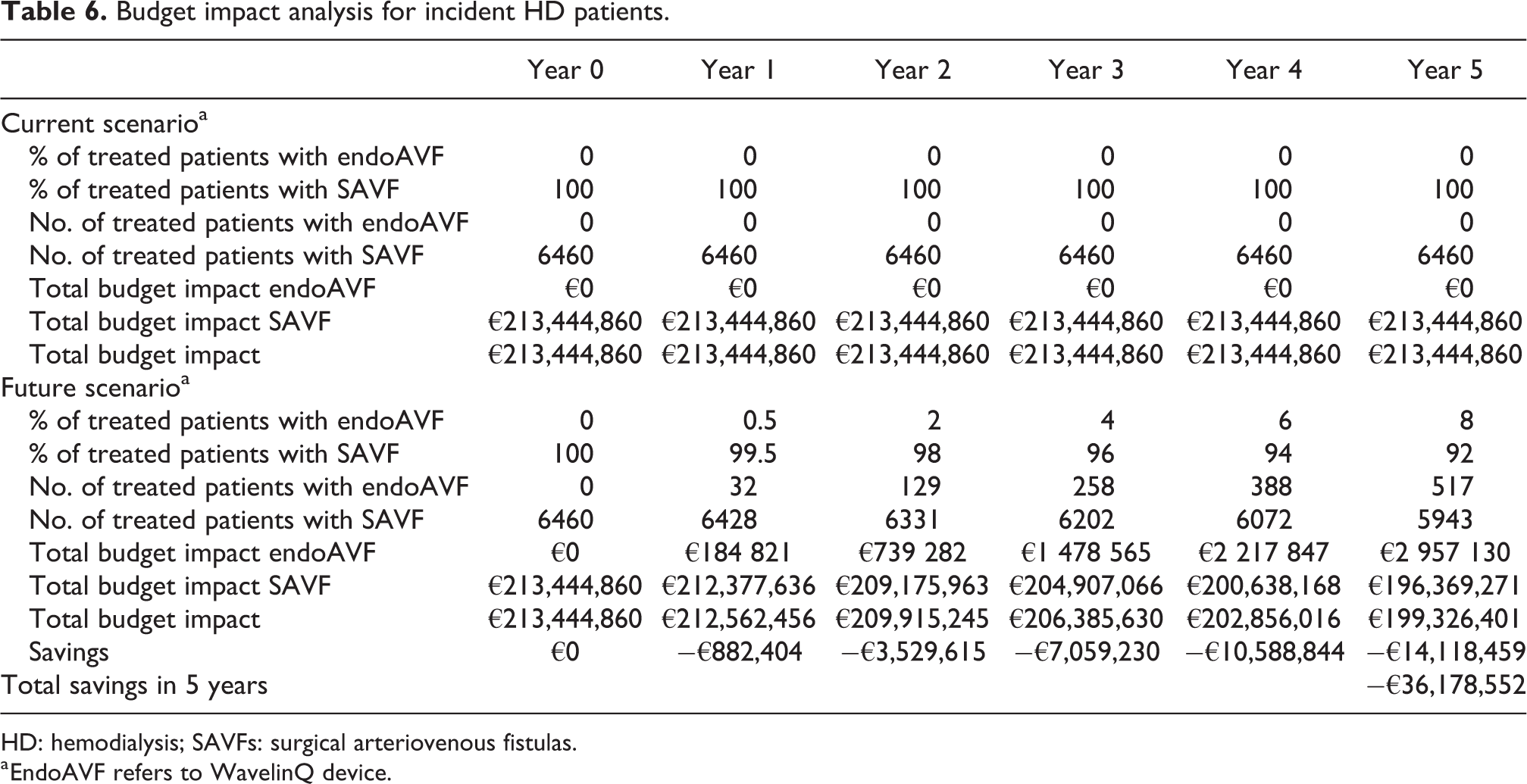
HD: hemodialysis; SAVFs: surgical arteriovenous fistulas.
a EndoAVF refers to WavelinQ device.
Discussion
Patients with progressive renal insufficiency or renal failure have limited possibilities of receiving an organ from a donor, as the number of available kidney donors is significantly lower than the growing incidence of end-stage renal disease. 46 To replace the kidney function by HD, the endovascular creation of AVF has emerged as an option in addition to the surgical procedure. The surgical placement of an arteriovenous access alone is challenging and may be subject to complications. Even with a precise technique, vessel irritation, turn phenomena, or neointimal hyperplasia may occur, leading to early closure or disturbed maturation. 7 Moreover, patients requiring AVF access are usually old, with comorbidities and with poor vessel conditions, resulting in only few treatment options available. All these factors may cause high failure and high reintervention rates. 47
EndoAVF creation is a sophisticated procedure providing a minimally invasive alternative to open surgical creation of AVF. This technique has been developed to address the limitations of surgical fistulas such as skin incision, vessel dissection, and the sutured anastomosis, which may result in prolonged healing, complications, and a low rate of functional fistula creation. 4 Furthermore, endoAVFs can be created in outpatient setting with local or regional anesthesia and sedation, and do not require the use of the operating theater. The proximal radial artery AVF created using an endovascular approach for the anastomosis showed excellent 2-year cumulative patency and a high level of patient satisfaction. 48
Although endoAVF showed promising clinical efficacy with a good safety profile in published studies and registries, 29,33 the use of this option at present is not officially recommended over SAVF creation. Large RCTs comparing endoAVF to SAVF have not been implemented and no comparative results from these studies have been published so far. Since endoAVF uptake in clinical practice is growing in Italy and in other countries, the use of real-world data to support decision-making may be in these cases highly relevant. 49,50
The present study aimed to evaluate the cost–utility of endoAVF versus SAVF and related budget impact at the national level to assess the value of currently available AVF creation procedures in the clinical practice in Italy. The analysis was performed using observational real-world data from a published study which compared WavelinQ versus surgical procedure for AVF creation. 17 Therefore, our findings are not generalizable to the entire class of endoAVF devices but, instead, to WavelinQ only.
The results from this analysis suggest that endoAVF performed with WavelinQ could be a cost-saving strategy in comparison to SAVF for incident and prevalent HD patients, from an Italian Healthcare Service perspective. Furthermore, the probabilistic sensitivity analysis confirmed the results, with the totality of the simulations lying below the commonly accepted ICUR threshold representing value for money. Moreover, the BIA showed that the Italian Healthcare Service could save from 30 to 36 million euros in the hypothesis of an increased utilization of WavelinQ, from 0.5% to 8%, in place of SAVF in the next 5 years.
From our analyses, it emerged a great difference in costs for AVF creation and its management for the two considered procedures. This difference is mainly due to the lower number of complications occurring after the endovascular procedure compared to the surgical one. The reference study 17 used for the CEA model implementation reported for the matched incident HD patients an event rate of 0.74/person-year for endoAVF versus 7.22/person-year for SAVF (p < 0.0001); similarly, in matched prevalent patients, the event rate was 0.46/person-year for endoAVF (WavelinQ) versus 4.10/person-year for SAVF (p < 0.0001).
In literature, there is paucity of studies presenting cost-effectiveness or budget impact analyses comparing endoAVF to SAVF in HD patients. To our knowledge, only Yu et al. 42 performed a cost-effectiveness analysis using retrospective data in the United States comparing endovascular AVF creation with WavelinQ from the Novel Endovascular Access Trial with propensity score–matched SAVF procedures from the US Renal Data System for 1 year after AVF creation. That study showed that, excluding the cost of the device, endovascular AVF creation resulted in a cost-saving option compared with the surgical one for both incident and prevalent HD cohorts. These results are in line with the ones of our study; this means that the savings could be used (at least partially) to cover the costs of the technological innovation, thus leaving the Italian Healthcare Service cost neutral in the worst case, that is, if all savings should be reverted to cover the incremental costs of the innovative procedure.
The present study has a number of limitations. First of all, the clinical effectiveness was derived on the matched databases with a limited number of patients in the US context; therefore, the generalizability of the real-world patient data collected to the broader Italian HD population could not be verified. Moreover, a small sample of patients belonging to a single center (the NEAT study, 60 patients) was matched with a tiny percentage of patients belonging to the Renal Data System in United States (n = 13,265). While the former group is composed by patients selected for endovascular AVF procedure according to best anatomical findings, clinical/physical aspects, and ultrasound examinations, the surgical group, although matched through main variables related to clinical history, may represent a broad set of patients with variations in vessel quality, preoperative evaluation, and surgical expertise; this may have led to underlying differences on other aspects not considered in the matching process, thus possibly limiting the validity of this kind of analysis.
Second, costing for healthcare resource consumption was based on DRG reimbursement rates which, in general, especially in the context of use of medical devices, does not cover the actual cost of the procedure and materials. In Italy, the NHS acts as both third-party payer and provider of healthcare services. This means that—besides DRGs (i.e. tariffs level)—it might be important to estimate the actual production costs from the hospital perspective. This estimation could be important for hospitals, especially when procurement strategies and negotiations with the manufacturers are at stake, especially in times of growing interest in value-based procurement aimed at acquiring technologies whose benefits outweigh the extra costs. Third, since data on patients’ quality of life were not available for the investigated population, assumptions have been made to populate the model health states with utility coefficients retrieved by literature. Moreover, worsening of patients’ quality of life due to fistula management (e.g. thrombolysis, thrombectomy) has not been considered in the model, and this could have led to possible overestimations of patients’ QALYs. Fourth, clinical outcomes and resource consumption related to patients managed with new technologies, such as endoAVF, may be influenced by the underlying learning curve related to the experience of the operators. 51 Continuous monitoring and data collecting could provide more robust data also for the evaluation of this aspect.
Finally, because the model used for the economic evaluations was developed according to published data comparing WavelinQ versus surgical procedure, the results of our analyses are valid only for this comparison, and no conclusions may be made on other endovascular devices. Further studies would be needed before our findings can be extended to other comparisons.
In conclusion, endoAVF with WavelinQ seems to be a valid option for the creation of HD venous access. Medical devices, which are subject to incremental innovation and operators’ learning curve, present challenges with respect to drugs concerning their assessment process; 52 in this case, the production of real-world evidence can sometimes be more meaningful for policy makers in comparison with RCTs. 51 Future real-world studies comparing endoAVF to SAVF will be able to increase the clinical evidence to confirm or reject the validity of this preliminary evaluation, not only for WavelinQ but also for other possible endovascular devices for AVF. In the time being, decision-makers may base on these preliminary results coverage recommendations for approval in defined target patient populations.
Supplemental material
Supplemental Material, Appendix - Endovascular versus surgical creation of arteriovenous fistula in hemodialysis patients: Cost-effectiveness and budget impact analyses
Supplemental Material, Appendix for Endovascular versus surgical creation of arteriovenous fistula in hemodialysis patients: Cost-effectiveness and budget impact analyses by Carla Rognoni, Matteo Tozzi and Rosanna Tarricone in The Journal of Vascular Access
Supplemental material
Supplementary_Table_1 - Endovascular versus surgical creation of arteriovenous fistula in hemodialysis patients: Cost-effectiveness and budget impact analyses
Supplementary_Table_1 for Endovascular versus surgical creation of arteriovenous fistula in hemodialysis patients: Cost-effectiveness and budget impact analyses by Carla Rognoni, Matteo Tozzi and Rosanna Tarricone in The Journal of Vascular Access
Supplemental material
Supplementary_Table_2 - Endovascular versus surgical creation of arteriovenous fistula in hemodialysis patients: Cost-effectiveness and budget impact analyses
Supplementary_Table_2 for Endovascular versus surgical creation of arteriovenous fistula in hemodialysis patients: Cost-effectiveness and budget impact analyses by Carla Rognoni, Matteo Tozzi and Rosanna Tarricone in The Journal of Vascular Access
Footnotes
Authors’ note
No interferences occurred in carrying out the research project and in writing the manuscript for which the authors are the sole responsibility.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics statement
Ethics approval and informed consent was not sought for this study because the data used for the analyses were derived exclusively from studies published in literature.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was funded by Confindustria Dispositivi Medici Servizi Srl through an unrestricted grant to CERGAS, SDA Bocconi School of Management, Via Roentgen 1, 20136 Milan, Italy.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.