
Abstract
Introduction
The relationship between intradialytic ultrafiltration volume and vascular access (VA) patency remains unclear. Using data from the Japan Dialysis Outcomes and Practice Patterns Study, we analyzed whether large-volume ultrafiltration was associated with VA failure in hemodialysis patients.
Methods
We included 2736 patients for whom it was possible to evaluate VA patency and bodyweight change during dialysis. Patients were divided into three groups according to the tertile of intradialytic ultrafiltration by bodyweight: low, -9.5%-3.8%; middle, 3.8%-5.1%; and high, 5.1%-13.7%. Primary VA patency was defined as the time to first VA intervention, and secondary patency as the time to creation of a new VA. Hazard ratios for VA failure were compared across groups by using Cox regression models adjusted for age, sex, body mass index, diabetes, hemoglobin and phosphorus levels, Kt/V, and erythropoiesis-stimulating agent and antiplatelet use.
Results
For the low, middle, and high groups, the incidences of primary and secondary VA patency were 4.7, 5.6, and 6.7 events/100 person-years and 1.3, 1.6, and 1.7 events/100 person-years, respectively. Adjusted hazard ratios for primary VA patency in the middle and high groups versus the low group were 1.16 (95% confidence interval [CI], 0.88-1.52) and 1.41 (95% CI, 1.07-1.87), respectively; those for secondary VA patency were 1.29 (95% CI, 0.78-2.13) and 1.45 (95% CI, 0.86-2.45), respectively.
Discussion
Large-volume ultrafiltration during dialysis tended to increase VA failure in hemodialysis patients. We thus recommend smaller ultrafiltration volumes during hemodialysis to secure VA safely.
Keywords
Introduction
Vascular access (VA) failure has been a major concern for hemodialysis patients, staff, and physicians, because VA dysfunction is recognized as a major cause of morbidity and hospitalization among hemodialysis patients (1). With respect to the factors associated with VA patency, reported factors include VA surgery, blood vessel pathogenesis, therapeutic interventions, handling, and factors involved in the self-management of hemodialysis patients (2468101214). Importantly, the previous literature has revealed that a considerable number of VA thromboses could occur in the absence of an anatomic stenotic lesion (15). Some non-stenotic VA thromboses might occur due to such VA surveillance factors as VA cannulation and compression, post-dialysis dehydration with increased blood viscosity, low-flow states, and venous pressure. It has also been hypothesized that decreased VA blood flow in non-stenotic VA dysfunction could occur from such factors as dialysis hypotension, hypovolemia, and decreased cardiac output (16).
Large-volume ultrafiltration might be an important risk factor for VA complications, including failure, in hemodialysis patients. However, the relationships between intradialytic ultrafiltration volume and VA patency remain unclear. Previous anecdotal publications (15, 16) regarding VA stated that ultrafiltration volume affects VA survival, but no observational studies have reported an association between intradialytic ultrafiltration volume and VA patency. Thus, the aim of this study was to determine whether large-volume ultrafiltration is associated with VA failure, using results obtained from phases 3 and 4 of the Japan Dialysis Outcomes and Practice Patterns Study (J-DOPPS).
Methods
Study design
The J-DOPPS 3 (2005-2008) and 4 (2009-2011) were prospective cohort studies based on data from randomly selected adult patients undergoing hemodialysis at more than 60 randomly selected dialysis facilities in Japan. These were part of the Dialysis Outcomes and Practice Patterns Study (DOPPS) (17) that aimed to clarify the association between hemodialysis practice and patient outcomes, including mortality, hospitalization, health-related quality of life, and VA outcomes, using worldwide samples. All participants provided informed consent, and the study protocol was approved by the Ethics Committee of Kyoto University Graduate School and Faculty of Medicine. Details of the DOPPS sampling and study methods have been described previously (17).
Study subjects
The target population included adult hemodialysis patients (aged ≥18 years) who had an arteriovenous fistula (AVF) or an arteriovenous graft (AVG). Such subjects were selected from J-DOPPS 3 and 4 if data on ultrafiltration volume per bodyweight (%UV; see below) were available. In the present study, subjects were further limited to those who had received hemodialysis for >1 year, since patients new to dialysis tend to have unstable VA and are more likely to experience various VA events other than thrombosis.
Outcomes and exposure
The outcome of interest was VA thrombosis. The primary outcome was primary patency; that is, the time until VA thrombosis that necessitated any of the following vascular salvage procedures: catheter placement, thrombectomy, surgical repair, thrombolysis, angioplasty, or stenting. The secondary outcome was secondary patency; that is, the time until use of a new VA port due to VA thrombosis. The date of incidence of these outcomes was identified for each patient, and the survival time was defined as the period from the start of observation until the occurrence of the initial event. Each subject was censored after the initial event.
The exposure of interest was %UV at baseline. In DOPPS, bodyweight was recorded before and after dialysis by medical staff at each facility. We calculated %UV as follows:

Statistical analysis
%UV was categorized into tertiles (defined as low, middle, and high), and these categories were used for all analyses. To describe patient characteristics, continuous variables were expressed as the mean and standard deviation, and categorical variables were expressed as percentages. Patient characteristics were also described in terms of the three categories of %UV. The incidence of patency failure was described in terms of the three categories by using the incidence rates as well as Kaplan-Meier survival curves.
Unadjusted and multivariable-adjusted Cox proportional hazard regressions were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs). In the multivariable model, the following possible confounders were included: patient age, sex, years in end-stage renal disease, body mass index, serum phosphorus and albumin levels, single-pool Kt/V, access blood flow, VA location, AVG use, six comorbidities (diabetes mellitus, cardiovascular disease, cardiac valvulopathy, cerebrovascular disease, hypertension, and peripheral vascular disease), and medications used (erythropoiesis-stimulating agents, antiplatelets, and anticoagulants). For the results of the multivariable models, trends with adjusted HRs were tested. A multiple imputation approach using a chained-equations method was employed to account for missing values of confounding factors. A total of 515 patients (18.8%) had missing confounder values. All analyses were performed using Stata SE version 13.1 (StataCorp LP, USA). The p values <0.05 were taken as indicators of statistical significance.
Results
Patient characteristics
Of the 5298 patients enrolled in DOPPS 3 and 4, 2736 (51.6%) were eligible. Their mean age was 63.4 years, 38.1% were women, and mean %UV was 4.5%. The majority of patients (2539 out of 2736; 92.8%) had an AVF, and the others had an AVG. Table I shows the patient characteristics for the study population overall and for the low, middle, and high %UV subgroups.
Baseline demographics and other characteristics in the study population
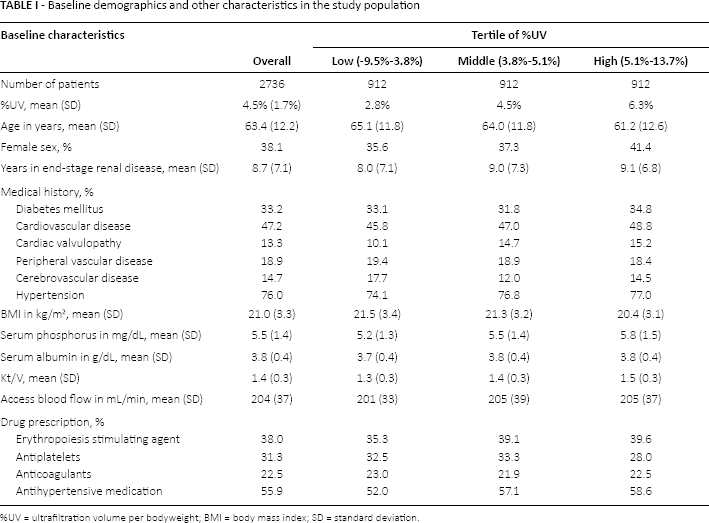
%UV = ultrafiltration volume per bodyweight; BMI = body mass index; SD = standard deviation.
Incidence of patency failure
Among the 2736 patients over a mean follow-up period of 2.3 years, there were 351 primary patency failures. The incidence rate was 5.6 events/100 person-years. There were 103 secondary patency failures, and the incidence rate was 1.6 events/100 person-years.
Association between %UV and incidence of primary patency failure
Higher %UV values were associated with more primary patency failures: the incidences were 4.7, 5.0, and 6.7 events/100 person-years, respectively, for the low, middle, and high %UV subgroups. Figure 1A shows the Kaplan-Meier survival curves for primary patency by subgroup.
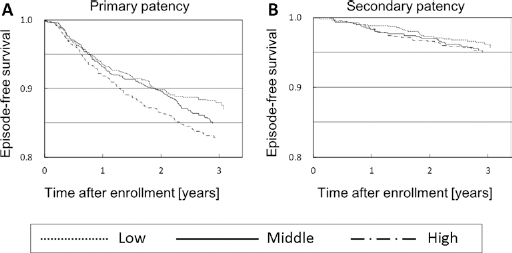
Kaplan-Meier curves for primary (
Compared with that in the low group, the incidence was higher in the middle and high groups: crude HRs were 1.20 (95% CI, 0.91-1.56) and 1.41 (95% CI, 1.09-1.84), respectively, and the adjusted HRs were 1.16 (95% CI, 0.88-1.52) and 1.41 (95% CI, 1.07-1.87), respectively, (trend p = 0.015) (Fig. 2).
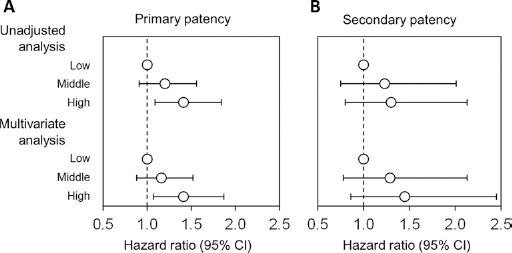
Association between ultrafiltration volume per bodyweight (%UV) and primary (
Association between %UV and incidence of secondary patency failure
Although statistically non-significant, the same trends as for the primary outcome were observed for secondary patency. The incidence rates for patency failure were 1.3, 1.6, and 1.7 events/100 person-years, respectively, for the low, middle, and high %UV subgroups. Survival curves stratified according to tertile are shown in Figure 1B.
Compared with the low group, the HRs for the middle and high subgroups were: crude HRs, 1.23 (95% CI, 0.75-2.01) and 1.30 (95% CI, 0.80-2.13), respectively, and adjusted HRs, 1.29 (95% CI, 0.78-2.13) and 1.45 (95% CI, 0.86-2.45), respectively, (trend p = 0.16) (Fig. 2).
Discussion
In this study, we examined the association between VA patency and ultrafiltration volume during dialysis by using data from the J-DOPPS. This was the first study designed to analyze the relationship between VA patency and intradialytic ultrafiltration volume.
The results showed that greater intradialytic ultrafiltration volume was associated with a greater incidence of primary VA failure (p = 0.015). Similarly, our analyses demonstrated a trend toward increased secondary VA failure (p = 0.16) with greater intradialytic ultrafiltration volume. Although we did not observe a significant correlation between intradialytic ultrafiltration volume and secondary VA failure probably due to the small number of events, the point estimates of HR for secondary VA patency were similar to those for primary VA patency. These results support the hypothesis that ultrafiltration volume during dialysis affects VA patency. On the other hand, allowable ultrafiltration volume directly affects the patient burden of food intake, so further studies are needed to ascertain the relationship between ultrafiltration volume and secondary patency.
In a previous literature, Brattich et al (16) showed that low blood pressure, volume depletion, and decreased cardiac output as a surveillance item for low output were risk factors for VA thrombotic occlusion or stenosis. Chang et al (18) showed that patients with large-volume ultrafiltration were likely to have VA failure in a sub-analysis of data from the hemodialysis (HEMO) study subjects, but their results were not statistically significant. The study further showed that the frequency of episodes of large-volume ultrafiltration was directly associated with the frequency of episodes of intradialytic hypotension, supporting our results. Taken together, these studies suggest that intradialytic hypotension might cause insufficient blood flow to the VA and increase the risk of VA thrombosis.
Quintaliani et al (4) examined the incidence of VA occlusion and survival of native AVFs in patients undergoing daily dialysis compared to those in patients undergoing standard dialysis three times per week. Their results showed that the incidence of AVF failure in the daily dialysis group was less than that of the group undergoing dialysis three times per week, and that the AVF survival rate of the daily dialysis group was superior to that of the group undergoing dialysis three times per week. In general, the bodyweight gain of the daily dialysis group should be smaller than that of the group undergoing dialysis three times per week, and their results suggested that large-volume ultrafiltration increased the risk of VA thrombosis.
To avoid the effect of an early VA failure, the subjects enrolled in the present study were further limited to those who had been undergoing hemodialysis for >1 year. In other words, we targeted matured AVFs in this study. With regard to VA maturation, native AVFs often fail early within the first month due to technical errors in VA operation (15). Uremic damage and hemodynamic injury to the vessel after VA creation play a role in initial VA non-maturation (2, 19). Dember et al (20) showed that 60% of placed AVFs failed to mature for dialysis in their large, multicenter, randomized controlled clinical trial. Allon and Robbin (3) showed that the mean 1-year primary survival rate for AVFs was 70% (range, 42%-90%). Therefore, the number of VA events in this analysis was small, so we assumed that this study properly evaluated the relationship between ultrafiltration volume and VA patency.
“How we can secure VA safely” is the most important effort for all the dialysis team and patients, because they can manage their bodyweight gain between dialysis sessions that is major determinant of ultrafiltration volume. Furthermore, dialysis staff can also help improve VA survival by educating patients on how to manage bodyweight gain between dialysis sessions.
There are several limitations to the present study. First, data related to blood pressure and hemoglobin levels during hemodialysis were not available for each patient. The J-DOPPS only had information for pre- and post-dialysis blood pressure. The blood pressure fluctuation patterns during dialysis vary widely, and it is very difficult to clarify whether blood pressure during hemodialysis had an effect on VA patency. Second, we obtained pre- and post-dialysis hemoglobin measurements for only one day. In other words, the present study could not adjust for the effects of factors such as hemoglobin concentration or decreased blood pressure during dialysis. Finally, due to the overwhelmingly high usage of AVFs for VA in Japan, this study could not evaluate the relationship between the patency of AVGs and ultrafiltration volume. In order to clarify the relationships between intradialytic ultrafiltration volume and AVG patency, worldwide data are required.
In conclusion, this study showed that large-volume ultrafiltration during hemodialysis is associated with the occurrence of frequent VA intervention. Preventing a larger intradialytic ultrafiltration volume, for example, by reducing bodyweight gain between dialysis sessions, might contribute to extending VA patency.
Footnotes
Financial support: The DOPPS is administered by Arbor Research Collaborative for Health and is supported by scientific research grants from Amgen (since 1996), Kyowa Hakko Kirin (since 1999, in Japan), Sanofi/Genzyme (since 2009), Abbott (since 2009), Baxter (since 2011), and Vifor Fresenius Renal Pharma (since 2011), without restrictions on publications.
Conflict of interest: S. Fukuhara and T. Akizawa have acted as scientific advisors to and received grants from Kyowa-Hakko Kirin. T. Akiba reports personal fees from Japan Tabacco, Toray, and Astellas, and grants from Kyowa-Hakko Kirin, Chugai, and Novartis during the conduct of the study. Other authors have nothing to declare.