
Abstract
Introduction
The quality of the life in patients requiring long term hemodialysis is directly proportional to the long-term patency of their vascular access. Basilic vein transposition for vascular access (BAVA) represents a suitable option for creating a tertiary native vascular access for hemodialysis on the upper extremities for patients requiring long term hemodialysis. The purpose of the study is to compare BAVAs with arteriovenous grafts (AVG).
Method
Data collection was based on selecting all of the patients with BAVA created in the time period in between January 1996 and August 2011. A questionnaire was created and sent to the selected hemodialysis centers. The resulting set of data was statistically analyzed and evaluated.
Results
In the time period between 1 January 1996 and August 2011, arteriovenous access for hemodialysis was created in 6754 patients (7203 procedures in total). Out of these patients, 175 BAVAs were created. Our patient database of those undergoing the BAVA procedure consisted of 98 females (56%) and 77 males (44%) with an average age of 64.5 years. The prevalence of diabetes mellitus was 60% (105 patients). Primary patency after 12 months was 68.8%, 24 months 59.7%, 36 months 53.8, 48 months 53.8%, and 60 months 50%. Primary assisted patency after 12 months was 89.9%, 24 months 84.6%, 36 months 77.8%, 48 months 77.9%, 60 months 70.8%. Secondary patency after 12 months was 89.4%, 24 months 86.9%, 36 months 81%, 48 months 78.9%, 60 months 75.7%. Twenty-nine BAVAs (16.5%) were obliterated.
Conclusion
Patients benefit from this type of procedure due to the longer patency of a native arteriovenous access, as well as a lower incidence of infectious complications.
Introduction
The creation and maintenance of well-functioning vascular access (VA) for hemodialysis has always been a major challenge and concern for patients, nephrologists, and vascular surgeons. Well-functioning VA is vital in patients with end-stage renal disease undergoing long-term hemodialysis. 1 Radiocephalic and brachiocephalic arteriovenous fistulas still remain the first and a second choice for creating a native VA for hemodialysis. 2 If these options are exhausted or not possible due to anatomical reasons, basilic vein transposition may be considered. The basilic vein is used very rarely for intravenous lines and venipunctures due to its unsuitable anatomical localization. The increasing number of elderly and diabetic patients with end-stage renal failure requiring long-term hemodialysis requires different VA strategies. This group of patients requires multiple operations and endovascular interventions in order to maintain a well-functioning VA. In such difficult cases, where all the other alternatives of VA placement on the upper extremities have been exhausted, basilic vein transposition and the creation of brachial-basilic arteriovenous fistula (BAVA) offers a suitable alternative over central vein cannulation, decreasing the overall cost of dialysis patients and morbidity emphasized by the KDIGO guidelines.3–5
Method
We performed a restrospective analysis of all BAVAs created in the time period from January 1996 to August 2011. The number of placed BAVAs performed in this time period was 175, accounting for 24% of the total number of procedures performed at this time period. Every patient indicated for BAVA had exhausted all possibilities for creating a native radiocephalic and brachiocephalic arteriovenous access. Before a BAVA was placed, every patient underwent an angiographic evaluation of the basilica vein and deep venous system. All patients with unsuitable anatomy for BAVA were excluded, and BAVA was not performed. All BAVAs were implanted in the standard manner as described later. All BAVAs were created as a one-stage procedure. Surgical dissection of the brachial artery and basilic vein with ligation of all visible branches was performed. After the dissection of the basilic vein, the resection of the vein at its proximal end was performed. The resected distal basilic vein was washed with heparinized saline solution. A tunneling device was used to create a superficial subcutaneous tunnel for the basilic vein in order to create good access for hemodialysis cannulation. An end-to-side anastomosis of ~4–6 mm was created between the basilic vein and the brachial artery using a polyprolylene 6-0 suture. Needle puncturing for hemodialysis was allowed six weeks after the graft implantation.
During BAVA creation, antibiotic therapy with cefazolin (1 g) was given intravenously 1 hour before the procedure and then in 12-hour intervals. In total, each patient was intravenously administered 3 g of cefazolin. No anticoagulation protocol was applied during the procedure. Patients with antiaggregation drugs continued in their therapy after the implantations. Patients receiving anticoagulation therapy were switched to low-molecular-weight heparin for the time period of the surgery, and then put back on their original anticoagulation therapy after the surgery.
Every patient underwent an ultrasonography checkup within the first month of the initial surgery, and then in regular intervals until the BAVA was terminated. Every patient underwent frequent checkups from their nephrologists during hemodialysis, where renal parameters were monitored and their general state of health was examined. Subsequently, a retrospective analysis of our patient's database was performed.
Data collection was based on selecting all the patients with BAVA created in the time period in-between January 1996 and August 2011. A questionnaire was created and was sent to the selected hemodialysis centers. The main points of the questionnaire were as follows: age of the patient at the time of BAVA creation, the time interval between the BAVA and the first endovascular or surgical intervention, BAVA patency, the time of BAVA access closure, and, if applicable, the information about possible cause of death of the patient. The definitions used to define patency were as follows: the primary patency: time from the creation of BAVA to the first endovascular or surgical intervention; the primary-assisted patency: time from the creation of BAVA to the first closure of the BAVA; and the secondary patency: time from the creation until the final closure of the BAVA. The resulting set of data was statistically analyzed and evaluated. Because the research comprised a retrospective analysis of anonymized data, it was exempted from seeking ethical committee approval.
The Kaplar–Meier method was used for calculating primary, primary-assisted, and secondary patencies. Statistical analysis was performed by using MedCalc version 12.2.1.0.
Results
In the time period from January 1996 to August 2011, we performed 7203 VA surgeries at our center. The number of placed BAVAs performed in this time period was 175, accounting for 2, 4% of the total number of procedures performed at this time period. All created BAVAs were used for hemodialysis. Our patient's database consisted of 98 females (56%) and 77 males (44%) with an average age of 64.5 years. The incidence of diabetes mellitus was seen in 60% (105) of patients. Primary patency was 68.8%, 59.7%, 53.8%, 53.8%, and 50% after 12, 24, 36, 48, and 60 months, respectively. Primary-assisted patency was 89.9%, 84.6%, 77.8%, 77.9%, and 70.8% after 12, 24, 36, 48, and 60 months, respectively. Secondary patency was 89.4%, 86.9%, 81%, 78.9%, and 75.7% after 12, 24, 36, 48, and 60 months, respectively (Fig. 1). A total of 29 (16.5%) BAVAs were obliterated, 144 (82%) BAVAs created in this time period remained patent until the end of follow-up period, or the patient's death; 53 (30%) of the implanted BAVAs are patent up to date. Infectious complications were found in 3.4% (6) of patients. In comparison, 1032 arteriovenous graft (AVGs) were implanted in the same time period at our center. The patency of our AVGs are as follows: the primary patency of AVG was 54%, 29%, and 12% for 6, 12, and 24 months, respectively; the primary-assisted patency of AVG was 83%, 69%, 54.5%, 44%, and 37% for the time period of 12, 24, 36, 48, and 60 months, respectively; and the secondary patency of AVG was 87%, 78%, 68.6%, 62%, and 55.8% for 12, 24, 36, 48, and 60 months, respectively. AVG infectious complications at the given time period was 6%. 6 When AVG vs. BAVA patency results were compared, BAVA had significantly higher secondary patency at 60 months, 75.7% vs. 55.8% of AVG. Also infectious complications were significantly lower in BAVA patients, 3.4% vs. 6% of AVG.
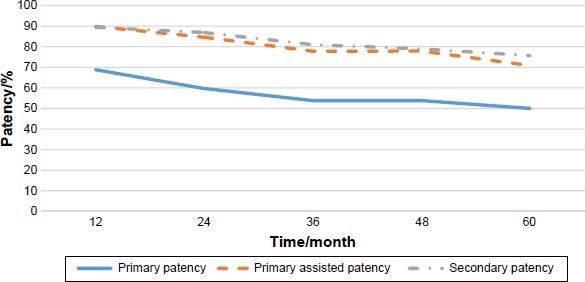
Basilic vein transposition patencies.
Discussion
The first choice for a VA in a patient requiring long-term hemodialysis is radiocephalic and brachiocephalic arteriovenous fistulas. 7 If the primary and secondary arteriovenous fistulas fail, the tertiary option for VA is problematic and not a clearly resolved issue. The available alternatives are either prosthetic vascular graft (AVG) or BAVA. It is well known that autogenous VA is preferred before the use of AVG due to its improved patency and lower risk of infectious complications.8,9 However, AVG has some advantages when compared with BAVA such as easier creation in obese individuals, earlier puncture after graft placement, and greater reintervention rate in access failure. 10 Davoudi M. et al showed that there are no major differences in primary patency between AVG and BAVA. 8 This finding was supported by other published studies comparing AVG vs. BAVA patencies.11–14
Basilic vein transposition is technically more challenging than the AVG placement. In order to achieve good access of the basilic vein for repeated venepuncture, its superficialization must be performed. In concurrence with the published literature, the main disadvantage of BAVA is its high rate of nonmaturation reaching up to 38%. There are many reasons for such a high level of nonmaturation: technical aspects of the procedure, torque of the vein, and anatomical abnormalities of the basilic vein, as described by Anaya-Ayala et al. 15 The first basilic vein transposition was reported by Dagher et al. 16 Over the past decade, different modifications of the original basilic vein transposition have emerged, such as endoscopic harvest, basilica vein elevation, and one- and two-stage basilica vein transposition.17–19 One of the most debated questions of today is the one-stage vs. two-stage basilic vein transposition. So far, the published data do not allow to determine the superiority of one technique over the other.4,20,21
Currently, there are only a couple of studies published in literature that compare patency, complications, and outcome analysis of different techniques of basilic vein transposition.3,22,23
Conclusion
Arteriovenous access created by transposition of basilic vein represents a surgically more complicated and time-consuming procedure when compared with the use of prothetic vascular graft. Patients benefit from this type of procedure due to the longer patency of a native arteriovenous access, as well as the lower incidence of infectious complications. Definite data on which procedure should be used when we consider a basilic vein transposition are not apparent. Published data are not consistent with the superiority of one procedure over the other. A randomized, prospective study is needed to demonstrate the superiority of one procedure over the other in order to define the gold standard technique for basilic vein transposition.
Author Contributions
Conceived and designed the experiments: RN. Analyzed the data: RN, MS. Wrote the first draft of the manuscript: RN. Contributed to the writing of the manuscript: PM, JHrubý. Agree with manuscript results and conclusions: JL, PM. Jointly developed the structure and arguments for the paper: RN, JL. Made critical revisions and approved final version: JL, JHlubocký. All authors reviewed and approved of the final manuscript.