
Abstract
Introduction
A retrospective chart review was conducted of visual analog scale (VAS) scores completed before and after trigger point injections (TPIs) for pelvic floor myofascial spasm to evaluate response.
Methods
Sixty-eight female patients who underwent TPIs from October 9, 2007 to March 12, 2015 were included. The primary end point was the difference between scores. Secondary analyses were conducted for patients who needed repeat TPIs. Descriptive and paired t test analyses were used.
Results
The key result was an improvement in VAS scores for 65% (44/68) of patients (p<0.0001). The median pre-injection VAS score was 7 (1 to 10), (mean 6.3). The median post-injection VAS score was 4 (0 to 9), (mean 4.3). The median difference between scores in patients who improved was 3 (1 to 8), (mean 3.6). Seventeen of 68 (25%) patients needed repeat TPI, and the median time between injections was 1.5 months (1 to 7 months), (mean 2.2 months). When analyzing pre-injection VAS scores in patients who underwent subsequent repeat injection when compared to patients who did not require repeat injection, there was no difference (p = 0.32). In addition, the differences between pre- and post-injection VAS scores in the patients who underwent repeat injection and those who did not was not significant (p = 0.26).
Conclusions
We report on 68 women who underwent TPIs, with an improvement in VAS pain scores in 65%. It appears that TPIs for pelvic floor myofascial spasm are successful in reducing pain scores for patients who are refractory to primary therapy.
Introduction
Chronic pelvic pain affects roughly 14% of women in the USA, predominantly between the ages of 30 to 50 years. It is most widely defined as the presence of pain in the pelvic region for more than 6 months. In many cases, the cause is undiagnosed (1). While gynecologic problems such as endometriosis or pelvic inflammatory disease may cause episodic or continuous pain that interferes with the patient's quality of life, chronic pelvic pain can originate from non-gynecologic causes (2). Considered a diagnosis of exclusion, myofascial pain syndrome, or trigger point pain, is a subtype of chronic pelvic pain defined by short, tight pelvic floor muscles with hypersensitive trigger points. It commonly presents with symptoms of overactive bladder, dyspareunia, or constipation, as well as aching, burning, clenching, or feelings of heaviness (1). Local trigger point pain may refer to distant areas or cause development of additional trigger points in surrounding muscle groups. Digital reproduction by a transvaginal or transrectal exam may elicit a local twitch response (3). The exact incidence of pelvic floor myofascial spasm is not known; however, Carter (3) reported an incidence of 7% in 500 patients.
Although the etiology of myofascial pain and pelvic floor myofascial spasm is unclear, acute or repetitive trauma to the pelvic floor from sports injuries, obstetric delivery, sexual trauma, post-traumatic stress disorder, or previous surgeries may cause hyper-intensive stimulation of the motor plate of the pelvic floor muscles (4). A prospective study using a validated questionnaire reported that operative vaginal delivery may have more of a negative impact on postpartum sexual functioning at 6 months after delivery compared to spontaneous vaginal delivery and cesarean delivery; however, results of other investigations have been conflicting with most reporting no evidence of a direct association between mode of delivery and postpartum sexual outcomes (5, 6). Additionally, diminished blood supply due to poor posture, leg length discrepancy, and joint misalignment may cause hypersensitivity of muscle pain receptors (7, 8). Hypersensitivity and chronic pain may also be associated with central sensitization, in which pain sensory input from the peripheral nervous system elicits an increase in the excitability and synaptic efficiency of neurons in the central nociceptive pathway (9). Persistent reactivity results in allodynia and hyperalgesia (9). Development of central sensitization from peripheral chronic pain is likely the result of predisposing factors including stress response (10), pre-existing anxiety about pain (11, 12), previous psychological or physical trauma (13), and poor sleep (14).
In one case series of 49 patients, 92% of patients suffering from myofascial pain demonstrated trigger points in the levator ani muscles, while 65% demonstrated trigger points in the suprapubic muscles, 45% in the obturator internus muscles, and 43% in the iliopsoas muscles (15). Physical examination of the involved muscles requires knowledge of pelvic floor anatomy. Forming the levator ani muscles, the pubococcygeus muscles are found between the 1 and 5 o'clock and the 7 and 11 o'clock positions, the iliococcygeus is found between the 4 and 8 o'clock positions, the obturator internus is found superior and lateral at the 10 and 2 o'clock positions, and the coccygeus is found deeper at the 5 and 7 o'clock positions (Fig. 1) (16).
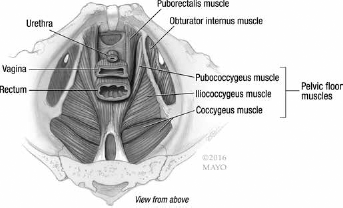
Pelvic floor muscle anatomy.
Patients typically have a history of or undergo evaluation for other causes of pain in the pelvis before making the diagnosis of pelvic floor myofascial spasm. Management of patients with pelvic floor myofascial spasm involves a multidisciplinary collaborative approach. Specialties may include gynecology, physical therapy, gastroenterology, urology, and pain management.
First-line therapies in the management of pelvic floor myofascial spasm include behavioral modification, topical heat/ cold, muscle relaxants, and physical therapy. Pelvic floor physical therapy typically includes breathing exercises, posture correction, manual therapy, and stretching (7). At our institution, pelvic floor physical therapy consists of 1 to 2 sessions per week for a total of 8 to 12 sessions by a trained physical therapist. Sessions involve manual therapy, including transvaginal or transrectal trigger point release, connective and scar tissue mobilization, and neural mobilization/stretching.
Drug therapy is with non-addicting medication and may include nonsteroidal anti-inflammatory drugs (NSAIDs), gabapentin, pregabalin, antidepressants, benzodiazepines (orally or vaginally), and skeletal muscle relaxants. If a patient is addicted to narcotics, referral to a chronic pain rehabilitation program is undertaken.
Trigger point injections are recommended as a treatment for pain flares or for patients with pelvic floor myofascial spasm with tender trigger points who are unable to tolerate physical therapy. Injections typically consist of local anesthetics and a steroid. Langford et al (17) found that 13 of 18 patients (72%) with chronic pelvic pain and palpable levator ani muscle trigger points reported pain relief 3 months after trigger point injections. Complete pain relief was reported by 33% of patients. Despite this study's limited size, it reflects that nonsurgical, office-based therapies such as trigger point injections can be effective. Trigger point injections in conjunction with physical therapy may enhance patient response to physical therapy and accelerate improvement, although patients may notice more soreness following treatment (17).
Zoorob et al (18) conducted a randomized trial of 29 pelvic floor myalgia patients with 17 receiving physical therapy and 12 receiving levator-directed trigger point injections of a mixture containing 40 mg/mL triamcinolone, 2% lidocaine, and 0.25% bupivacaine. Treatments were administered weekly. Up to 6 trigger point injections or 12 physical therapy sessions were allowed. Pain was assessed 1 month after completion of treatment using the Numeric Rating Scale (NRS) and Patient Global Impression of Improvement Index. Sexual function was assessed using the Female Sexual Function Index. Both groups demonstrated reduction of vaginal pain based on improved NRS values; 94% of the physical therapy cohort and 83% of the trigger point injections cohort reported improvement in levator ani muscle pain. Although both therapies improved sexual function, improvement in sexual pain favored physical therapy. The time, in weeks, to pain improvement favored trigger point injections (4.4 weeks vs. 7.3 weeks for pain to be rated at least “a little better”). The study concluded that either approach may be acceptable for myofascial pain; however, disclosing differences in time before appreciable pain improvement may factor into patient decision making (18).
We aim to evaluate treatment success by reviewing visual analog scale (VAS) scores before and after trigger point injections to the pelvic floor in patients with pelvic floor myofascial spasm that are refractive to primary therapy.
Methods
The retrospective chart review was approved by the Mayo Clinic Institutional Review Board. Patient charts were accessed through a secure hospital-based portal, and data were collected by an author (LF) and study participants. The clinical setting was a tertiary care medical and surgical gynecology outpatient office. Charts of 68 patients who underwent outpatient transvaginal trigger point injections for pelvic floor myofascial spasm were reviewed between October 9, 2007 and March 12, 2015. Female patients who completed VAS scores before and after the procedure were eligible. A 10-point VAS was used ranging from “no pain” (score of 0) to “pain as bad as it could possibly be” (score of 10). Post-injection VAS scores were mailed in by patients 1 to 2 weeks after treatment. We collected demographic and clinical data on age, race, parity, smoking status, sexual activity, presenting symptom, duration of pain, coexisting conditions, previous operations, imaging, and medications.
All patients were clinically diagnosed with pelvic floor myofascial spasm with tender palpable trigger points after evaluation to exclude other undiagnosed causes of chronic pelvic pain. The treatment flow sheet is depicted in Figure 2. Presenting symptoms, medical/surgical history, and physical examination findings guided diagnostic work-up. All patients who underwent trigger point injection were undergoing pelvic floor physical therapy concurrently.
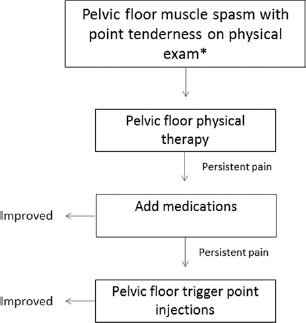
Management of pelvic floor myofascial spasm - Treatment flow sheet.
All patients received injections from the same provider, a female pelvic medicine and reconstructive surgery specialist. Between patients, the trigger point injection technique varied in specific locations injected, total sites injected, and the inclusion of the steroid component in the mixture. The steroid component was avoided in patients using other local or systemic steroids. It was also not used in several other circumstances, including patients with diabetes mellitus, immunosuppression, or an allergy to steroids. Trigger point injection to the pelvic floor is described in detail in Appendix 1 (available online as Supplementary material at www.j-endometriosis.com) and the instrument set-up is displayed in Figure 3.

Pelvic floor trigger point instrument set-up: 10 mL 3-finger syringe, 22-gauge spinal needle, trumpet guide (left to right).
The primary end point was the difference between pre-and post-injection scores. Our secondary endpoints included assessment of repeat trigger point injection and duration between injections. Recorded VAS pain scores before and after the repeat injections were not available for review. Missing patient data were not factored into final calculations. Descriptive and paired t test analyses were used for collected data using JMP v.10.0.0 software (SAS Institute Inc, Cary, North Carolina, USA) downloaded on a secure desktop. Our study complies with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement of the Enhancing the QUAlity and Transparency Of health Research (EQUATOR) network (http://www.equator-network.org/reporting-guidelines/strobe/).
Results
After retrospective review of pre- and post-injection VAS scores, an improvement in scores was seen in 44 of 68 patients (65%; p<0.0001). The median pre-injection VAS score was 7 (range, 1 to 10; mean, 6.3) (Fig. 4A). The median post-injection VAS score was 4 (range, 0 to 9; mean, 4.3) (Fig. 4B). In patients who improved, the median difference between pre- and post-injection scores was 3 (range, 1 to 8; mean, 3.6). Of 68 patients, 17 (25%) needed repeat trigger point injection. The median time between injections was 1.5 months (range, 1 to 7 months; mean, 2.2). When analyzing pre-injection VAS scores in patients who underwent subsequent repeat injection compared to patients who did not require repeat injection, there was no difference (p = 0.32). In addition, the differences between pre- and post-injection VAS scores in patients who underwent repeat injection and those who did not was not significant (p = 0.26).
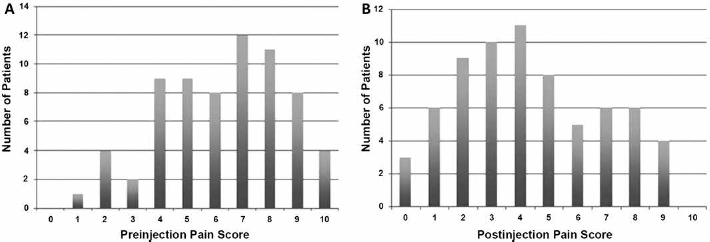
(A) Pre- and (B) post-injection visual analog scale scores.
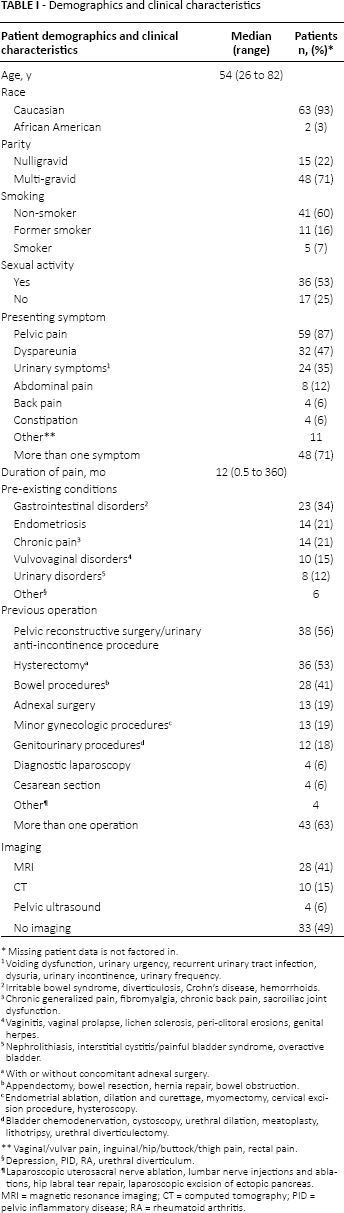
Patient demographic and clinical characteristics are present in (Tab. I). The median age of patients was 54 years (range, 26 to 82 years). The majority of patients were Caucasian (n = 63, 93%), multigravidas (n = 48, 71%), nonsmokers (n = 41, 60%), and sexually active (n = 36, 53%). The median reported duration of pain upon initial consultation was 12 months (range, 0.5 to 360; mean, 36 months). Among the medication categories used by patients, benzodiazepines were the most common (n = 61, 90%), followed by antidepressants (n = 39, 57%), narcotics (n = 33, 49%), NSAIDs (n = 29, 43%), muscle relaxants (n = 28, 41%), and neuroleptics (n = 15, 22%) (Tab. II). The most common medication initiated after diagnosis of pelvic floor myofascial spasm was vaginal diazepam (n = 19). Others were oral diazepam (n = 14), tizanidine (n = 11), and gabapentin (n = 1).
Demographics and clinical characteristics
Missing patient data is not factored in.
Voiding dysfunction, urinary urgency, recurrent urinary tract infection, dysuria, urinary incontinence, urinary frequency.
Irritable bowel syndrome, diverticulosis, Crohn's disease, hemorrhoids.
Chronic generalized pain, fibromyalgia, chronic back pain, sacroiliac joint dysfunction.
Vaginitis, vaginal prolapse, lichen sclerosis, peri-clitoral erosions, genital herpes.
Nephrolithiasis, interstitial cystitis/painful bladder syndrome, overactive bladder.
With or without concomitant adnexal surgery.
Appendectomy, bowel resection, hernia repair, bowel obstruction.
Endometrial ablation, dilation and curettage, myomectomy, cervical excision procedure, hysteroscopy.
Bladder chemodenervation, cystoscopy, urethral dilation, meatoplasty, lithotripsy, urethral diverticulectomy.
Vaginal/vulvar pain, inguinal/hip/buttock/thigh pain, rectal pain.
Depression, PID, RA, urethral diverticulum.
Laparoscopic uterosacral nerve ablation, lumbar nerve injections and ablations, hip labral tear repair, laparoscopic excision of ectopic pancreas. MRI = magnetic resonance imaging; CT = computed tomography; PID = pelvic inflammatory disease; RA = rheumatoid arthritis.
Medication use
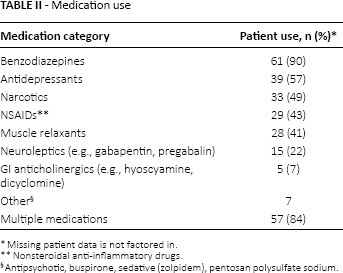
Missing patient data is not factored in.
Nonsteroidal anti-inflammatory drugs.
Antipsychotic, buspirone, sedative (zolpidem), pentosan polysulfate sodium.
Discussion
Pelvic floor myofascial spasm is often an overlooked cause of chronic pelvic pain that coexists with other conditions. It is after work-up for other etiologies of pelvic pain that the diagnosis of pelvic floor myofascial spasm is made. With proper evaluation of the pelvic floor, the diagnosis is easily confirmed. Of the patients in our subset, 76% had pre-existing gastrointestinal disorders, endometriosis, and chronic pain. Furthermore, approximately half of patients underwent an imaging study as part of their pelvic pain work-up (Tab. I). Patients usually undergo treatment for other conditions that are not the main contributor of reported symptoms.
The clinical characteristics of patients with pelvic floor myofascial spasm add to the complexity of diagnosis. Most patients present with more than one symptom, use multiple medications, and have had multiple previous operations. In our review, pelvic pain, dyspareunia, and voiding and defecation dysfunction were among the common presenting symptoms. The two most common categories of previous operations were pelvic reconstructive surgery/urinary anti-incontinence procedures and hysterectomies with or without concomitant adnexal procedures (Tab. I). It is, therefore, paramount to make the diagnosis of pelvic floor myofascial spasm after excluding other causes in the setting of multiple confounding presenting symptoms and surgical histories.
Medications along with physical therapy are considered first line in the management of patients with pelvic floor myofascial spasm. Vaginal diazepam is our preferred medication to start when patients undergoing physical therapy are having persistent pain. Vaginal administration of benzodiazepines (compounded vaginal diazepam 5 mg suppository twice daily as needed) has a more favorable adverse effect profile than the oral route, which is more sedating (Tab. II) (17, 18).
A multidisciplinary approach to patients with pelvic floor myofascial spasm is essential in management. All of our patients were undergoing prescribed pelvic floor physical therapy either at our institution or elsewhere. Pain management and gastroenterology services were involved in 24% of patients either prior to initial consultation or through referral by our department.
Patients with persistent painful trigger points despite physical therapy and medication are considered candidates for injection to the pelvic floor. Through the results of our retrospective review, we demonstrate statistically significant improvement in VAS pain scores with pelvic floor trigger point injections. These results expand on the previously cited studies (17, 18). The proposed mechanisms of action of trigger point injections are disruption of reflex arcs within skeletal muscles, release of endorphins, and mechanical changes in abnormally contracted muscle fibers.
The majority of patients did not need a repeat injection, and those who did had pain relief for an average of 2.2 months between injections. Initial pain scores and pain score differences did not differ significantly between patients who underwent repeat injection versus the patients who did not undergo repeat injection. This observation suggests that relapse of pain is of a complicated nature, and patients may present and respond to injections similarly even though they may need further therapy in the future. Furthermore, our study was not powered to determine the potentially complex relationship between patient characteristics and need for repeat injection, especially since we did not have VAS scores for the repeat injection. With larger studies, it may be possible to predict patients who will likely need repeat therapy based on clinical characteristics and pain scores.
In addition to VAS pain scores, it is important to recognize that sexual health and quality-of-life measures are deserving of attention when evaluating the response of trigger point injections to the pelvic floor. Our study does not evaluate these measures; however, our institution is currently using validated questionnaires in our patient population to investigate this for further study.
Other modalities available for the management of refractory pelvic floor myofascial spasm to conservative therapy (medications and physical therapy) include botulinum toxin and electrical nerve stimulation. Botulinum toxin A injection into the pelvic floor has been found to be effective. The results of a prospective pilot study of 21 patients who underwent electromyographic-guided botulinum toxin A injections into the pelvic floor showed improvement in pain, dyspareunia, and quality-of-life measures up to six months after injections. Side effects of botulinum toxin injection include bleeding at the injection site, mild flu-like symptoms, urinary and flatal incontinence, and constipation (19). In our practice, patients who do not experience a long duration of pain relief with pelvic floor trigger point injections are offered off-label use of botulinum toxin injections to the pelvic floor after counseling on the risks and benefits. We inject the pelvic floor trans-vaginally into areas of spasm with 200 U of botulinum toxin without electromyographic (EMG) guidance. Furthermore, use of vaginal transcutaneous electrical nerve stimulation as adjunctive therapy in patients with pelvic floor myofascial spasm may improve pain from levator muscle spasm; however, randomized controlled studies with a standard approach are needed (20, 21).
The strengths of this review include its novel use of VAS scores before and after trigger point injection to the pelvic floor to demonstrate response; and its analysis of patients who required repeat injection. In addition, our review can serve as a pilot study for future multicenter, prospective studies.
The main limitations of our review are its retrospective nature and small sample size. Compound mechanisms play a major role in pain syndromes making it hard to extrapolate data without confounding relationships potentially altering conclusions. As discussed earlier, the presence of multiple comorbidities in our cohort is an important bias to be considered. Furthermore, we did not subject patients to a wash-out period from other medications or procedures, including muscle relaxants and physical therapy. These observations are considered potential confounding bias affecting the validity of our study results in evaluating pelvic floor injections. Other limitations further amplifying this effect include absence of a control group, changes in an individual's physician practices over time, missed data, and recall bias. Our results may not be generalizable to the general population, notably since our cohort presented to a tertiary care specialized center.
Conclusions
Trigger point injection to the levator ani muscles is a minimally invasive, nonsurgical treatment option for patients who have pelvic floor myofascial spasm and are refractive to physical therapy and medication. We report on 68 women who underwent injections by a single physician and show an improvement in VAS pain scores in 65% of patients. Further study is needed to address the use of trigger point injection and the applicability of a standardized treatment algorithm for pelvic floor myofascial spasm using large, prospective randomized controlled studies.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has financial interest related to this study to disclose.