
Abstract
Introduction
Vitamin D receptor (VDR) and proteins encoded by the genes CYP27B2 and CYP24A1 involved in the production and inactivation of vitamin D can influence vitamin D and the susceptibility to colorectal cancer (CRC). The objective of this study was to investigate the relationship between the risk of CRC and polymorphisms in VDR, CYP27B1 and CYP24A1, lifestyle and dietary habits.
Methods
The study included 152 patients with CRC and 321 controls. All participants answered a questionnaire on their dietary habits, alcohol consumption and smoking habits. DNA was extracted from peripheral blood. Polymorphisms of BsmI and ApaI were identified by performing PCR-RFLP. Identification of CYP24A1 (rs6013897, rs158552 and rs17217119) and CYP27B1 (rs10877012) polymorphisms was performed by gene sequencing.
Results
Smoking, alcohol use, and low or no consumption of fruit, cereals and dairy products were associated with an increased risk of CRC. A heterozygous genotype Aa or an association genotype aa + Aa of the VDR ApaI polymorphism increased the risk of CRC. The VDR BsmI polymorphism was not significantly associated with the risk of CRC. Multivariate analysis showed that heterozygous and association genotype AT + AA of the rs6013897 polymorphism, genotype CT of the rs158552 polymorphism, association genotype CT + CC and genotypes AA and GG of the rs17217119 polymorphism of CYP24A1, and heterozygous genotype GT and association genotype GT + TT of the rs10877012 polymorphism in CYP27B1 were associated with a higher risk of CRC.
Conclusions
Dietary habits, lifestyle, and polymorphisms in VDR (ApaI), CYP24A1 (rs6013897, rs158552, rs17217119) and CYP27B1 (rs10877012) were associated with a higher risk of CRC.
Introduction
Worldwide, colorectal cancer (CRC) is the third most common cancer among men and the second most common cancer among women. An estimated 1.2 million new cases and 694,000 deaths occur annually (1). In Brazil, CRC is the third most common cancer, with 34,280 new cases yearly (2).
Improper diet and lifestyle increase the risk of CRC (3, 4). Vitamin D along with calcium exerts protective effects against the development of CRC (5).
Exposure of the skin to the sunlight is the major source of vitamin D in the body, with >90% of vitamin D being obtained in this manner. Synthesis of vitamin D in the skin begins with the action of ultraviolet (UV) light on 7-dehydrocholesterol and its conversion to cholecalciferol (vitamin D3) and ergocalciferol (vitamin D2). During circulation, both bind to vitamin D-binding protein (VDBP) and are transported to the liver and converted to 25-OH vitamin D by 25-hydroxylase. The 25-OH vitamin D is then converted to 1,25-(OH) 2-vitamin D by 1 α-hydroxylase (a protein encoded by CYP27B1) in the kidneys (6, 7). Vitamin D is metabolized in the bowel, bone, liver and kidneys by a mitochondrial enzyme 24-hydroxylase (CYP24) or cytochrome P450 protein encoded by CYP24A1 (7). The active 1,25-(OH) 2-vitamin D is a steroid hormone that is transported by carrier proteins to target cells where it binds to its receptor (VDR) (8, 9). The active vitamin D-VDR complex modulates gene transcription and regulates mineral ion homeostasis.
VDR also mediates the effects of vitamin D on the growth and differentiation of target tissues and on the immune response (6). VDR was first described in 1969 as a protein encoded by a gene located on chromosome 12q12-14. Polymorphisms commonly found in VDR are Cdx2 (exon 1), FokI (exon 2), TaqI (exon 9), ApaI, BsmI, Tru91 (intron 8) and poly(A) (3′ UTR). These polymorphisms have been investigated in various cancers including CRC (8–11). Polymorphisms in VDR differ according to the ethnicity of the population (12) and may influence the effects of vitamin D.
A recent review and meta-analysis analyzed the role of VDR polymorphisms in different cancers (13). Several studies have explored the association of CYP24A1 polymorphisms with cancer.
Because the studies conducted to date have provided inconsistent results with respect to the association of polymorphisms in VDR, CYP24A1 and CYP27B1, ethnicity, and external factors with the risk of CRC, it is necessary to perform further investigations. Thus, the present study evaluated the correlation of polymorphisms in VDR, CYP24A1 and CYP27B1, lifestyle, and dietary habits with the risk of CRC.
Patients and Methods
The study sequentially and prospectively enrolled 152 patients with CRC and 321 controls without cancer. The diagnosis of colorectal adenocarcinoma in patients included in the study was confirmed by the pathologist. The patients were selected from the outpatient records of the Division of Gastrointestinal Oncology of the Federal University of São Paulo. Electronic medical records of patients were used to obtain information on the clinical stages of CRC and overall survival. Patients with a family history of cancer had been excluded.
The study was approved by the local ethics committee. All participants signed an informed consent form before participation in the study.
Age and sex-matched controls who did not have cancer (according to their medical records) were recruited from the central laboratory of the same institution. Patients with changes in their bowel aspects or a family history of cancer were excluded from the control group. A total of 333 patients had been invited to participate, of whom 12 were excluded: 6 had a past history of cancer, 4 a family history of cancer, and 2 had intestinal inflammatory disease.
All participants answered a questionnaire on dietary habits such as the frequency of intake of foods rich in fibers (vegetables, fruit and cereals, specifically granola, flax and oats), red meat, foods with a high oil content (fried foods), and milk and milk products, and on lifestyle habits such as smoking and alcohol consumption.
DNA was extracted from peripheral blood samples by means of a QIAamp DNA Mini Kit® (Qiagen) according to the manufacturer's protocol, and was quantified using an ND-1000 spectrophotometer (NanoDrop; Thermo Fisher Scientific Inc.).
The VDR polymorphisms BsmI and ApaI were identified by performing PCR-RFLP with primers and conditions described in previous studies (14). The primers used for BsmI were 5′-CAACCAAGACTACAAGTACCGCGTCA-3′ (forward) and 5′-ACTTCGAGCACAAGGGGCGTTAGC-3′ (reverse) and for ApaI 5′-CAGAGCATGGACAGGGAGCAAG-3′ (forward) and 5′-GCAACTCCTCATGGCTGAGGTCTCA-3′ (reverse).
The PCR products were digested with restriction enzymes BsmI and ApaI (New England Biolabs) at 65°C and 25°C, respectively, for 1 hour. The digestion products were electrophoresed on 2% and 3% agarose gels, respectively, stained with ethidium bromide, and visualized under UV light.
The polymorphisms in CYP24A1 (rs6013897, rs158552 and rs17217119) and CYP27B1 (rs10877012) were amplified using the primers 5′-CTTGATCCAAATGTCCGCAC-3′ (forward) and 5′-CTTTGGGTAGGTTACTTCTGC-3′ (reverse) for CYP24A1 and 5′-CTTGATCCAAATGTCCGCAC-3′ (forward) and 5′-GCCTGTAGTGCCTTGAGAGG-3′ (reverse) for CYP7B1. The amplicons were electrophoresed on 2% agarose gel stained with ethidium bromide and were visualized under UV light. The PCR products were purified using FastAP Thermosensitive Alkaline Phosphatase® (Thermo Fisher Scientific Inc.) and exonuclease I (Fermentas).
The samples were placed in a 96-well optical plate and sequenced using a BigDye® Terminator v3. 1 Cycle Sequencing Kit and BigDye® Xterminator™ Purification Kit. The plate was then placed in a 3500xL Genetic Analyzer (Applied Biosystems Inc.) for electrophoresis. The products of sequencing were visualized and the results were interpreted using the Sequence Scanner Software v1.0 (Applied Biosystems).
Statistical analysis
The frequency of male or female sex, food intake, drinking, smoking and gene polymorphisms in each group were analyzed using Fisher's exact test and the chi-square test. Differences in quantitative variables between groups were calculated using Student's t-test. Univariate and multivariate analyses were performed to determine the odds ratios (ORs) and 95% confidence intervals (CIs) for quantifying the risk of CRC. The Bonferroni correction was applied to the variables cereals, alcohol and cigarettes. Survival analysis was performed using the Kaplan-Meier method and was evaluated using the log-rank test. P values less than 0.05 were considered statistically significant. The statistical analyses were performed using SPSS version 10.0 for Windows (SPSS Inc.) and STATA Statistics Data Analysis version 8 (Stata Corp).
Results
The mean age (±standard deviation, SD) of the 152 patients with CRC was 62.8 (±13.02) years and that of the 321 controls was 62.7 (±10.42) years. Both groups included more men than women. In most patients with CRC, the cancer was localized in the colon (n = 98, 64.5%). One hundred and four patients (68.42%) did not show any evidence of cancer recurrence and were in follow-up; 61.2% of the patients with CRC had stage II or III cancer. At the end of the study period, 82.9% of patients were alive.
A large number of participants (63.8%-78.2%) in both groups consumed fruit, vegetables and milk daily. An increased risk of CRC was observed among participants who consumed fruit only monthly (OR = 2.22; 95% CI 1.02-4.83; p = 0.041) and cereals weekly (OR = 2.75; 95% CI 1.14-6.65; p = 0.022) or monthly (OR = 3.52; 95% CI 1.42-8.87; p = 0.006). Alcohol consumption was higher among patients with CRC. Moreover, participants who consumed alcohol daily had a 2.17 times higher risk of CRC (OR = 2.17; 95% CI 1.20-3.93; p = 0.009). After the Bonferroni correction, only alcohol consumption and consumption of cereals monthly were significant. Although the prevalence of smokers was higher among patients with CRC, the difference was not statistically significant (p = 0.239).
In controls, the polymorphisms in VDR, CYP24A1 and CYP27B1 were distributed according to the Hardy-Weinberg equilibrium (p>0.05). The heterozygous genotype of the VDR polymorphisms ApaI and BsmI was prevalent in both groups. The heterozygous genotype or the association between heterozygous and homozygous variants of the ApaI polymorphism increased the risk of CRC (p = 0.024 and p = 0.043, respectively; Tab. I). Analysis of the ApaI polymorphism according to sex and heterozygous genotype (Aa) showed that men had a 2.69 times (95% CI 1.45-5.13; p = 0.002) higher risk of CRC than women.
Genotypic distribution of the polymorphisms ApaI, BsmI, CYP24A1 and CYP27B1 and the risk of CRC
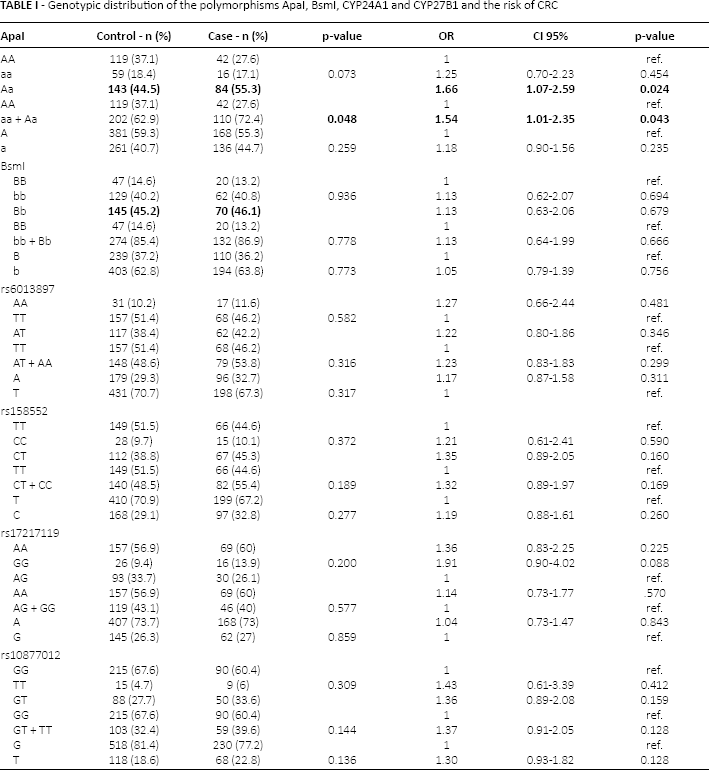
No relationship was observed between the BsmI polymorphism and the risk of CRC (p = 0.936) (Tab. I). Moreover, no correlation was observed between sex and the risk of CRC (p = 0.613 and p = 0.875 for men and women, respectively). The association of the heterozygous and homozygous variants of both VDR polymorphisms did not increase the risk of CRC (OR = 1.08; 95% CI 0.61-1.93; p = 0.77).
The polymorphisms of VDR (ApaI and BsmI) were not associated with poor survival (Fig. 1).
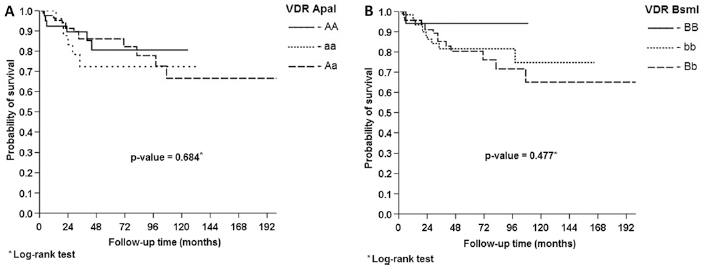
Kaplan-Meier survival curve of patients with CRC with respect to the genotypes of the VDR polymorphisms ApaI and BsmI. ApaI (A), BsmI (B).
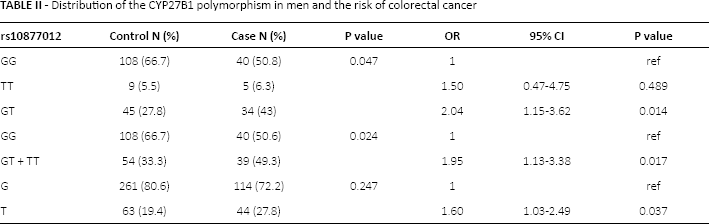
No significant difference was observed in the genotypic or allelic distribution of the CYP24A1 polymorphisms rs6013897, rs158552 and rs17217119 in both groups (Tab. I). The heterozygous genotype GT, the association of GT + TT, and the T allele of the CYP27B1 rs10877012 polymorphism increased the risk of CRC in men by 2.04, 1.95 and 1.60 times, respectively (Tab. II). Grouping all 3 polymorphisms of the CYP24A1 genotypes and CYP27B1, the dominant or recessive models increased the risk of CRC by 3.52 times (OR = 3.52; 95% CI 1.55-8.02; p = 0.003)
Distribution of the CYP27B1 polymorphism in men and the risk of colorectal cancer
No association was observed between the CYP24A1 and CYP27B1 polymorphisms and survival (Fig. 2).
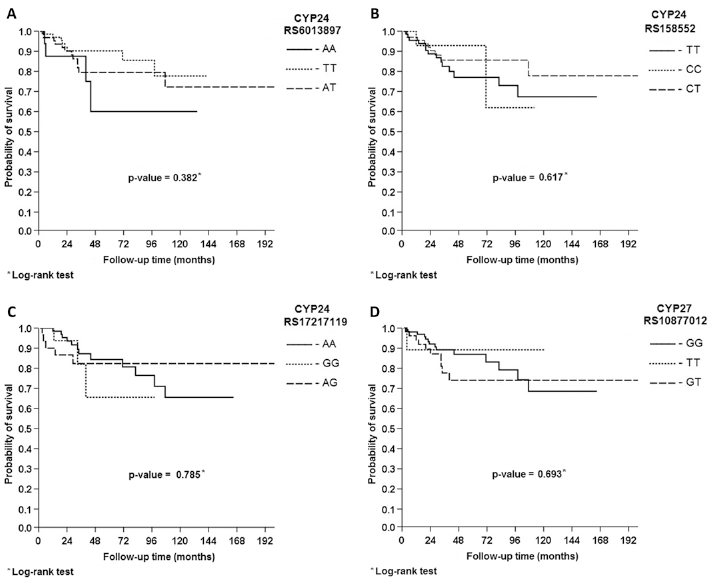
Kaplan-Meier survival curves of patients with CRC with respect to the CYP24A1 and CYP27B1 polymorphisms. CYP2A41 rs6013897 (A), CYP2A41 rs158552 (B), CYP2A41 rs17217119 (C), CYP2A7 rs10877012 (D).
Multivariate analysis was performed for all the polymorphisms studied (Tab. III). It showed that smoking, alcohol consumption and rare (monthly) intake of fruit increased the risk of CRC (data nor shown). The AT genotype of the rs6013897 polymorphism of the CYP24A1 gene was associated with a 3.50 times higher risk of CRC. The CT genotype of the rs158552 polymorphism was associated with a 2.63 times higher risk of CRC. The AA and GG genotypes of the rs17217119 polymorphism were associated with 3.46 (p = 0.005) and 3.79 times (p = 0.015) higher risks of CRC than the AG genotype. The GT genotype of the CYP27B1 rs10877012 polymorphism was associated with a 2.17 times higher risk of CRC (p = 0.004; Tab. III). The other polymorphisms studied were not associated with a higher risk of CRC in multivariate analysis.
Multivariate analysis of the risk of CRC based on the individual and grouped
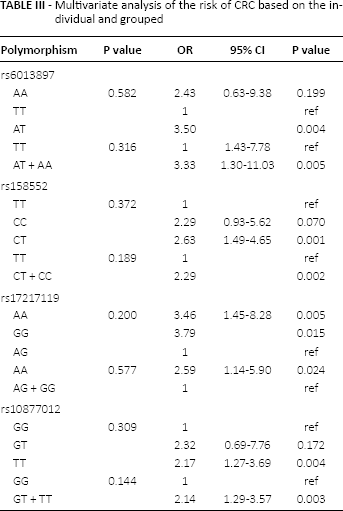
Grouping the CYP24A1 genotypes into dominant or recessive models increased the risk of CRC by 3.33 times for the AT + AA association genotype compared to the TT genotype of the rs6013897 polymorphism. The CRC risk increased by 2.29 times for the CT + CC association genotype compared to the TT genotype of the rs158552 polymorphism, and 2.59 times for the AG + GG association genotype compared to the AA genotype of the rs17217119 polymorphism. Further, the risk of CRC increased by 2.14 times for the GT + TT association genotype of the CYP27B1 rs10877012 polymorphism compared with the GG genotype (Tab. III).
Discussion
This case-control study analyzed the association of polymorphisms in VDR (ApaI and BsmI), CYP24A1 (rs6013897, rs158552 and rs17217119) and CYP27B1 (rs10877012), which are involved in the regulation of vitamin D, with the risk of CRC in 473 participants.
The mean age of the patients with CRC was 62.8 years, which was consistent with the data obtained by the Surveillance, Epidemiology and End Results (SEER) Program of the National Cancer Institute (15). Further, the frequency of CRC was higher among men (53.3%) than among women, which was consistent with other data reported (1).
Various studies have examined the association of intrinsic and extrinsic factors with different diseases. This observation is relevant from a scientific perspective and deserves further investigation. In the present study, we analyzed the association of environmental and lifestyle factors such as smoking, alcohol consumption and food intake (fiber as fruit, vegetables and cereals, red meat, fried foods, and milk or dairy products) and genetic and clinical factors with the risk of CRC. Obesity is also a risk factor of CRC, and a polymorphism of resistin, a gene involved in obesity, −420 C>G “CC”, has been associated with a decreased risk of CRC (16).
Tobacco contains amines and polycyclic aromatic hydrocarbons that induce mutations in oncogenes such as KRAS, BRAF and MYC, thus promoting metastatic and inflammatory responses. Multivariate regression analysis performed in this study showed a statistically significant association between smoking and the risk of CRC in multivariate analysis (OR = 3.62; 95% CI 1.26-10.45 for smokers; p = 0.017).
Ethanol and acetaldehyde are carcinogens that induce mutations in CYP24A1, increase the vulnerability of cells to oxidative stress, and promote increased proliferation and metastasis of cancer cells (17). In the present study, we observed in the multivariate analysis that daily alcohol consumption increased the risk of CRC. A meta-analysis of 16 studies reported an increased risk of colon cancer and rectal cancer among alcoholic participants (17).
Frequent intake of fruit, vegetables, cereals and dairy products may reduce the risk of CRC. In the present study, an increased risk of CRC was observed among participants who consumed fruit only monthly and who did not consume cereals. In contrast, consumption of vegetables was not significantly associated with the risk of CRC. In multivariate analysis, a higher risk of CRC was also observed among patients who ate fruit and cereals rarely. This was consistent with the results of a study involving more than 500,000 participants from 10 European countries who showed an increased risk of liver, lung and colorectal cancer (4). Higher intake of milk and dairy products was inversely correlated with the risk of CRC (18). However, it is necessary to affirm that the small number of controls and patients may make the interpretation of the protective role of diet in our study difficult.
No association was observed between the consumption of red meat, fats (fried food), and the risk of CRC in the present study. Other studies have reported an increased risk of CRC among individuals who consume red meat in large quantities because these foods contain heme (present in porphyrin) that induces gene mutations and cytokine expression. Durko and Malecka-Panas (19) indicated that methods used for cooking meat could also increase the risk of CRC because high temperatures stimulate the production of carcinogenic heterocyclic amines (16). Our results showing no association of fat intake with the risk of CRC are in agreement with those of a randomized clinical trial that reported no association between low fat intake and reduced risk of CRC (4, 17, 19).
VDR mediates the effects of vitamin D during bone and mineral metabolism, growth and differentiation of target tissues, and immune responses (7). A meta-analysis analyzing the role of the VDR polymorphisms in different cancers (CRC, prostate, breast, ovarian, skin, kidney, esophageal and oral cancers and glioma) showed that the VDR BsmI polymorphism was a risk factor for all the cancers studied (p<0.001), with a higher association with CRC (20). The risk of CRC was 1.27 times higher with the BB genotype of the BsmI polymorphism than with the bb + Bb genotype (OR = 1.27; 95% CI 1.02-1.57; p = 0.000). The same study showed that the aa genotype of the VDR ApaI polymorphism exerted a protective effect compared with the AA genotype (OR = 1.11; 95% CI 0.82-1.50; p = 0.022) (20).
In our study, the genotypic and allelic frequencies of the BsmI polymorphism were not different between the 2 groups (p = 0.936 and p = 0.773, respectively). However, the heterozygous Aa genotype of the ApaI polymorphism was associated with a 1.66 times higher risk of CRC (95% CI 1.07-2.59; p = 0.024). In Iranian patients, the homozygous aa genotype of the ApaI polymorphism was associated with an increased risk of CRC (9). In contrast, in a South Korean population, the same genotype was associated with a decreased risk of CRC (14).
In the present study, the Aa + aa genotype of ApaI was also associated with an increased risk of CRC compared with the AA genotype (OR = 1.54; 95% CI 1.01-2.35; p = 0.043). A study in African-Americans by Grant et al (21) showed that women with these genotypes had an increased risk of invasive ovarian cancer (p = 0.01). Similarly, a meta-analysis showed that the ApaI polymorphism was associated with a marginal risk of CRC in European and Asian populations (95% CI 0.80-1.00; p = 0.05) (22).
No correlation was observed between the survival of patients with CRC and the genotypes of the VDR polymorphisms ApaI and BsmI. These results are similar to those of studies on breast, oral and lung cancers (8, 23, 24).
Several studies have explored the association of the CY-P24A1 polymorphisms with various diseases (25). Recent studies have shown no association between the genotypic distributions of the CYP24A1 rs6013897 polymorphism and the risk of CRC (22). In the present study, multivariate analysis showed that the rs6013897 polymorphism of CYP24A1 was associated with a 3.5 times higher risk of CRC (95% CI 1.49-8.21; p = 0.004) in patients with the AT genotype and a 3.33-times higher risk of CRC in patients with the AT + AA genotype compared with patients having the TT genotype. Limited information is available on the CYP24A1 polymorphisms rs17217119 and rs158552. Case-control studies by international consortia have shown no positive correlation of these polymorphisms with prostate cancer (24). In our study, the CYP24A1 polymorphisms increased the risk of CRC. Multivariate analysis showed that the AA and GG genotypes of the rs17217119 polymorphism increased the risk of CRC by more than 3 times compared with the AG genotype. Grouping of the genotypes (AA vs. AG + GG) showed that patients with the AA genotype had a 2.59 times higher risk of CRC that those with the AG + GG genotype. The CT genotype of the rs158552 polymorphism was also associated with a higher risk of CRC.
A few studies have examined the association between CY-P24A1 and CYP27B1 polymorphisms and survival in patients with CRC. One study showed that women with the homozygous AA genotype of the CYP24A1 rs6013897 polymorphism were more likely (86%) to develop breast cancer (13). In our study, no statistically significant association was observed between the genotypes of the CYP24A1 and CYP27B1 polymorphisms and survival in patients with CRC.
Based on our results, we confirmed that environmental factors increased the risk of CRC. The VDR ApaI polymorphism also increased the risk of CRC, but only in the univariate analysis. However, the difference between the groups disappeared when the variables were associated in multivariate analysis. By contrast, with respect to the polymorphisms of the genes CYP24A1 and CYP24A7 the opposite occurred. The present study showed that the CYP24A1 and CYP27B1 polymorphisms, which have been explored rarely, were associated with a higher risk of CRC, thus providing a new perspective on the molecular mechanisms that influence the synthesis and metabolism of vitamin D. However, larger numbers of patients from different populations should be studied to validate the results of the present study.
In conclusion, the heterozygous genotype or the association of the heterozygous genotype with the homozygous variant genotype of the VDR ApaI polymorphism increased the risk of CRC. Multivariate analysis showed that polymorphisms in CYP24A1 (rs6013897, rs158552 and rs17217119) and CY-P27B1 (rs10877012) were also associated with a higher risk of CRC. However, no correlation was observed between the genotypes of the VDR, CYP24A1 and CYP27B1 polymorphisms and the survival of patients with CRC.
Footnotes
Financial support: The São Paulo Research Foundation (FAPESP) supported this study.
Conflict of interest: The authors have no conflict of interest to disclose.