
Abstract
Background
The metabolism of vitamin D is complex, its receptor (VDR) and proteins encoded by the genes CYP27B2 and CYP24A1 can influence vitamin D serum levels. The aim of this study was to investigate the relationship of the polymorphisms of VDR (ApaI and BsmI), CYP27B1 and CYP24A1 with serum vitamin D levels in both forms, 25(OH)D3 (circulating form) and 1,25(OH)2D3 (active form), in colorectal cancer (CRC) patients.
Methods
One hundred fifty-two CRC patients and 321 controls were included. DNA was extracted from peripheral blood. Polymorphisms of BsmI and ApaI were identified by PCR-RFLP. Those of CYP24A1 (rs6013897, rs158552 and rs17217119) and CYP27B1 (rs10877012) were determined by gene sequencing.
Results
The median serum levels of circulating vitamin D were not different between CRC patients and controls; however, the percentage of those with deficient vitamin D was higher in patients with cancer. The active form of the vitamin D was higher in CRC patients. VDR, CYP27B1 and CYP24A1 polymorphic genotypes had no influence on serum levels of circulating vitamin D. The correlation between circulating and active vitamin D forms was lower among patients with CRC, regardless of the presence or absence of any genetic polymorphism. The mean serum levels of active vitamin D were higher among patients with polymorphic genotype variants of Apa1 or Bsm1.
Conclusions
CRC patients had a higher frequence of insufficient vitamin D and a higher concentration of active vitamin D. These concentration were higher between patients with polymorphic genotypes variants of ApaI and BsmI, CYP24A1 and CYP27B1. Polymorphic genotypes cause a lower correlation between the forms of vitamin D.
Introduction
Colorectal cancer (CRC) is one of the most common neoplasms, and it is estimated that there are more than 1.3 million cases reported annually worldwide. In Brazil, CRC is the third most frequent neoplasm, behind only breast cancer and prostate cancer (1, 2).
CRC risk factors have been widely studied. These include the risks of inherited genetic diseases (such as Lynch syndrome and familial adenomatous polyposis), sporadic genetic alterations (such as mutations in the RAS gene and microsatellite instabilities), behavioral aspects (such as obesity and ingestion of excessive amounts of meat) and inflammatory bowel diseases (3-6).
Vitamin D is an important biological factor, and its signaling affects several cellular processes such as proliferation, differentiation and apoptosis. Its metabolism involves a complex mechanism that begins with the photolysis of the vitamin D precursor in the skin and undergoes successive hydroxylation processes in the liver and kidneys (7, 8). The metabolism of vitamin D occurs in several organs, such as the intestine, and depends on several proteins encoded by genes of the cytochrome P450 family (8).
Several studies have described vitamin D in its active form (1, 25-dihydroxyvitamin D [1,25(OH)2D3]), as a regulator of proliferation and differentiation in human cancer cells, where it is responsible for promoting cell cycle stabilization and apoptosis and regulating gene transcription (9-12). In the colon, vitamin D together with calcium has been shown to have a protective effect on colorectal carcinogenesis (9).
Several factors including geographic location and climate can directly affect the production of vitamin D and may result in a vitamin D deficiency, which can cause rickets and other chronic diseases such as cancer (13).
In view of the antioncogenic role of vitamin D and knowledge about the polymorphisms of the genes encoding the proteins responsible for their metabolism (such as CYP27B1 and CYP24A1) and, secondarily, about the genes that encode the vitamin D receptor (VDR), it is necessary to study whether these gene variations can affect the metabolism of vitamin D in patients with CRC at an academic, reference hospital.
Methods
Population
This study included 152 patients with CRC (cases) either receiving treatment or who were undergoing follow-up care at the Gastrointestinal Oncology Division, and a control group (controls) of 321 patients without cancer. All of the patients were included sequentially and were outpatients of the Hospital of Sao Paulo–Federal University of Sao Paulo, Brazil.
Patients were 18 years of age or older. A pathologist confirmed a colon or rectal adenocarcinoma. The control group consisted of individuals who were referred to the Central Laboratory of the Hospital of São Paulo for blood exams. There were no differences in age or sex between the 2 groups. Individuals with a change in bowel habits, reporting blood in their feces or with a history of CRC or inflammatory bowel disease were excluded from our study. Patients who reported taking vitamin D tablets were also excluded.
A local committee at the Hospital of São Paulo approved this study. All of the participants were informed about the study and signed the consent form before enrollment in the study.
Age and sex-matched controls who did not have cancer (according to their medical records) were recruited from the central laboratory of the same institution. Patients with changes in their bowel aspects or familiar history of cancer were excluded from the control group (14).
Material analysis
Peripheral blood was collected from the patients for genomic DNA extraction and for evaluation of the serum levels of vitamin D in circulating and active forms. The presence of VDR polymorphisms (ApaI and BsmI) was investigated using polymerase chain reaction (PCR) and genotyping by restriction fragment length polymorphism (RFLP), and the samples were electrophoresed on an agarose gel containing ethidium bromide to visualize the polymorphic products. The single nucleotide polymorphisms (SNPs) of the CYP27B1 (rs10877012) and CYP24A1 (rs6013897, rs158552 and rs17217119) genes were determined by gene sequencing.
DNA extraction from blood was performed using the QIAamp DNA Mini Kit commercial system (Qiagen, Hilden, Germany), according to the manufacturer's protocol. DNA quantification was performed using a ND-1000 Spectrophotometer (NanoDrop Technologies Inc., Wilmington, DE, USA).
The PCR primers and conditions have been described in previous studies (15-17). PCR products were digested for 1 hour by restriction enzymes BsmI at 65°C and ApaI at 25°C (New England Biolabs®). Subsequently, they were separated on a 2% or 3% agarose gel, respectively, stained with ethidium bromide and visualized under ultraviolet light.
The PCR products were purified using the following enzymes: FastAP Thermosensitive Alkaline Phosphatase R (Thermo Scientific, Waltham, MA, USA) and Exonuclease I R (ExoI R; Fermentas, Vilnius, Lithuania), and were then incubated in a thermocycler for 60 minutes at 37°C, followed by 15 minutes at 85°C.
The samples were then plated in a 96-well optical plate, and BigDye® Terminator v3.1 Cycle Sequencing Kit reagents (Applied Biosystems, Foster City, CA, USA) were added to each sample, along with the forward or reverse primers, to a final volume of 20 μL. The mixture was incubated in a thermocycler for 26 cycles at 95°C for 2 minutes, 96°C for 10 seconds, 50°C for 15 seconds and 60°C for 4 minutes.
For sequencing: the BigDye® XTerminator™ Purification Kit (Applied Biosystems, Foster City, CA, USA) was added to the product, and the sealed plate was taken to the shaker for 30 minutes and analyzed using an Applied Biosystems® 3500 × L Genetic Analyzer. The results were visualized and analyzed using Sequence Scanner v1.O software (Applied Biosystems, Foster City, CA, USA).
High-performance liquid chromatography (HPLC), using the appropriate curve calibration and analytical standards and controls, was used to analyze serum vitamin D levels, in both the precursor and active forms.
C9774 (Sigma-Aldrich) was used as standard and Chrom-systems MassCheck® 25-OH vitamin D3 (25(OH)D3) Serum Control (bi-level I + II) as control. The calibration curves were validated daily, with accepted deviations less than 5%. The dosages were repeated when the values were lower or higher than the reference (20-120 ng/mL).
Statistical analysis
The unpaired t-test was applied to verify the differences between the means of the continuous variables of the serum levels of vitamin D concentrations between the 2 groups. The Pearson correlation test was used to compare the mean serum levels of vitamin D and the different polymorphisms in each group. Multivariate analysis was performed to determine the odds ratios (ORs) and 95% confidence intervals (95% CIs) for quantifying the risk of CRC in relation to vitamin D sufficiency status. A p value of less than 0.05 was considered statistically significant.
Results
The mean age of the 152 patients in the CRC group was 62.8 ± 13.02 years and the mean age of the 321 participants in the control group was 62.7 ± 10.42 years (p = 0.945). Men made up 53.3% of the CRC group, and 50.8% of the control group.
The serum levels of circulating vitamin D did not differ between the CRC and control groups (p = 0.278). The proportion of participants with insufficient vitamin D levels was higher in patients with CRC than in the control group (51% vs. 43.3% in the control group), although the difference was not statistically significant (p = 0.126). In this analysis, deficiency in vitamin D levels was a significant risk factor for CRC. Furthermore, approximately half of the participants had a vitamin D deficiency regardless of group (Tab. I).
Vitamin D serum levels and risk of colorectal carcinoma
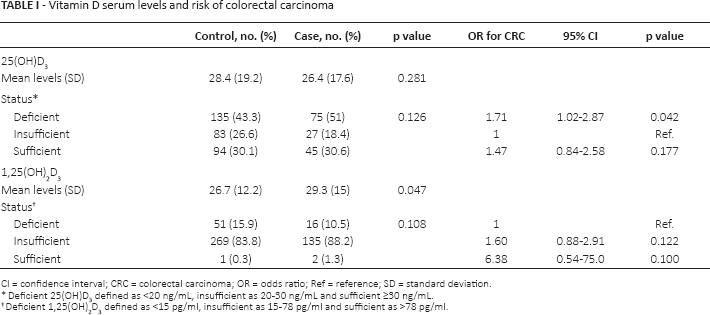
CI = confidence interval; CRC = colorectal carcinoma; OR = odds ratio; Ref = reference; SD = standard deviation
Deficient 25(OH)D3 defined as <20 ng/mL, insufficient as 20-30 ng/mL and sufficient ≥30 ng/mL.
Deficient 1,25(OH)2 D3 defined as <15 pg/ml, insufficient as 15-78 pg/ml and sufficient as >78 pg/ml
Serum levels of active vitamin D were higher in patients with CRC (Tab. I).
To verify the association of SNPs and mean serum levels of precursor or active vitamin D, the SNPs were distributed by genotype (Tabs. II and III). The serum levels of precursor vitamin D were not different between the VDR homozygous genotypes or in the heterozygous and homozygous variants. The mean serum levels of active vitamin D were higher in patients with polymorphic variants of Apa1 or Bsm1. The correlation between the precursor and active forms of vitamin D were higher in the control group. The correlation of the 2 forms of vitamin D among the polymorphic variants genotypes of Apa1 and Bsm1 with CRC was very weak (Tab. II).
Correlations between vitamin D receptor (VDR) polymorphisms and serum level of vitamin D
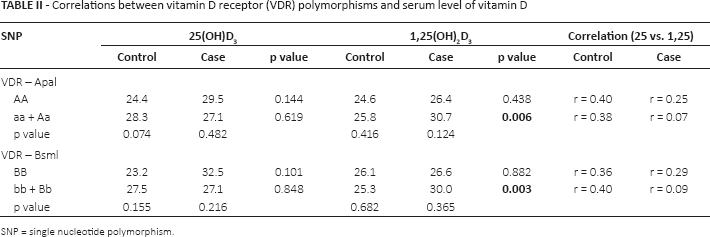
SNP = single nucleotide polymorphism
Correlations between CYP24A1 and CYP27B1 polymorphisms and serum level of vitamin D
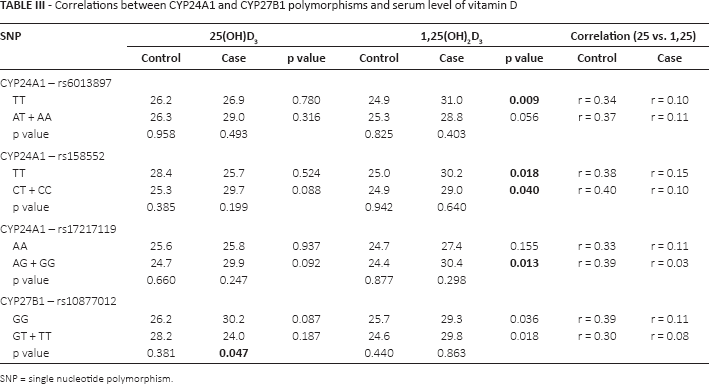
SNP = single nucleotide polymorphism.
For the different CYP24A1 polymorphisms, the mean serum levels of precursor vitamin D did not differ significantly between the groups. However, CYP27B1 was the only SNP studied that did have a statistically significant difference in circulating vitamin D level for the polymorphic genotype variants in the case group. When the serum levels of active vitamin D and the SNPs of CYP24A1 and CYP27B1 were analyzed, the mean serum levels were higher in patients with CRC (Tab. III). As observed for the SNPs of the VDR, the correlation between the 2 forms of vitamin D was lower in patients with CRC.
The relationship between the serum levels of vitamin D (in both precursor and active forms) in patients with CRC and controls was analyzed using the Pearson correlation. We observed a correlation between the serum levels of the precursor and active forms of vitamin D in the control group. However, in the CRC group, this relationship was not observed. This could be due to the higher concentration of active vitamin D levels identified in the serum levels of patients with CRC (Fig. 1).
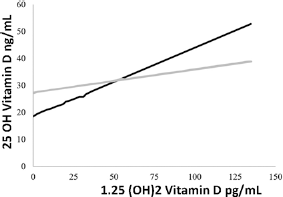
Correlations between circulating (25(OH)D3) and active (1,25(OH)2D3) forms of vitamin D in patients with colorectal cancer (CRC) and control patient group.
We did not find a difference in the correlation between serum levels of 25(OH)D3 and 1,25(OH)2D3 for the SNPs of VDR and CYP24A1. Analyzing the correlation between serum levels of different forms of vitamin D among the groups for each type of polymorphism, there was no difference in the correlation between serum levels of 25(OH)D3 and 1,25(OH)2D3 for the SNPs of VDR and CYP24A1. Although the difference was not statistically significant, the only exception was in rs10877012 of CYP27B1 where there was a higher correlation between levels of precursor and active forms of vitamin D in individuals without the polymorphism (Fig. 2).
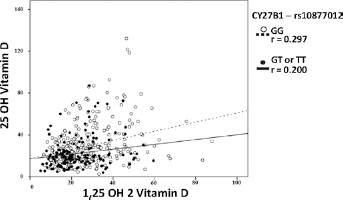
Correlations between circulating (25(OH)D3) and active (1,25(OH)2D3) forms of vitamin D in patients with or without the CYP27B1 polymorphism rs10877012.
Overall, it was observed that for all SNPs, patients in the CRC group had a lower correlation between circulating and active serum vitamin D levels than controls (Tabs. II and III).
Discussion
This case-control study analyzed the VDR, CYP24A1 and CYP27B1 polymorphisms in a total of 473 individuals. The aim of the study was to elucidate any association between these genetic variants and the serum levels of vitamin D in the precursor (25(OH)D3) and active (1, 25(OH)2D3) forms.
Previous studies have described an inverse correlation between the risk of several nonskeletal diseases and the mean circulating serum levels of vitamin D. Several meta-analyses have demonstrated a higher risk of breast, CRC and prostate cancer associated with lower levels of vitamin D (18, 19), and more recently an increased risk of mortality by cancer recurrence (20, 21). Although most studies point to the existence of a relationship, there are some conflicting data (22).
In this study, we did not observe a difference in the levels of active vitamin D between the groups; however, the percentage of patients with deficient precursor vitamin D levels was higher in patients with cancer. In contrast, the concentrations of the active form of vitamin D were higher in patients with CRC.
Analyzing the correlation between serum levels of precursor and active forms of vitamin D, we observed that, although CRC patients had higher serum levels of active vitamin D, they had a lower correlation between the 2 vitamin D forms. Based on our findings, we hypothesized that in patients with CRC, vitamin D metabolism is impaired rather than reduced.
In a previous study, we observed that some polymorphisms were associated with a higher risk of CRC (14). However, there are few studies evaluating the effects of polymorphisms on serum levels of vitamin D in cancer patients. According to Ma et al, carriers of the BB genotype of the VDR BsmI had higher serum levels of active vitamin D compared with individuals with the polymorphic genotype (23). Jorde et al reported that the AA genotype rs6013897 of CYP24A1 had lower circulating serum vitamin D levels compared with TT and AT in breast cancer (24). Similar results were also described by Mondul et al, in patients with CRC (25).
In our study, when the serum levels of precursor and active forms of vitamin D were analyzed for each SNP, there was no difference observed between individuals with or without polymorphisms. The exception was the lower serum level of precursor vitamin D in patients with CRC with the GG genotype compared with the polymorphic GT + TT genotypes of CYP27B1 (rs10877012).
The mean serum levels of vitamin D (in either precursor or active forms) and the risk of CRC may be affected by external factors such as the season, time of sun exposure, age, use of sun screens and pigmentation of the skin. Furthermore, intrinsic factors such as the polymorphisms may affect the synthesis and metabolism of vitamin D, although we found that individuals with CRC had a lower correlation between the precursor and active forms of vitamin D compared with the control group, irrespective of SNPs.
There were some limitations to this study, and therefore, its results should be evaluated with caution. The main limitation lay in the design of case-control studies, which limit the findings to the quality of the pairs between groups. The study population was done in a single clinical center, and this may limit the reproducibility of these findings. Another limitation of our study was the lack of a central review of polymorphisms and serum levels of vitamin D, which may limit the impact of the results presented. Finally, use of the Bonferroni model to adjust the p values for the number of variables assessed resulted in the findings described in Tables II and III being found to be not statistically significant.
This study confirms that individuals with CRC have some type of vitamin D metabolism disorder independent of the presence or absence of polymorphisms in the genes that regulate vitamin D metabolism.
Further studies including in larger populations and with multiple centers could confirm the data described in our study and improve our knowledge of vitamin D disorders in CRC.
In conclusion, patients with CRC had a higher serum concentrations of active vitamin D. Patients with CRC, irrespective of the presence or absence of polymorphisms in VDR, CYP24A1 and CYP27B1, also had a lower correlation between precursor and active forms of vitamin D, which could indicate an impaired vitamin D metabolism.
Footnotes
Financial support: Funding was provided by the FAPESP: Sao Paulo Research Foundation.
Conflict of interest: None of the authors has any financial interest related to this study to disclose.