
Abstract
Background
The human X-ray repair cross-complementing protein 1 (XRCC1) gene encodes for one of the major repair factors involved in base excision repair (BER), which is reported to be associated with the risk of several cancers. A few studies have explored the association between risk of hepatocellular carcinoma (HCC) and single-nucleotide polymorphisms (SNPs) in different DNA repair genes, with contradictory results. The purpose of this study was to evaluate the association between XRCC1 Arg399Gln polymorphism and susceptibility to HCC.
Methods
A total of 89 HCC patients and 99 randomly selected healthy controls were enrolled. Genotyping of XRCC1 rs25487 was performed by high-resolution melting analysis and Sanger sequencing.
Results
On univariate analysis, a statistically significant association was found between risk of HCC and XRCC1 399Arg/Gln genotype (odd ratio [OR] = 1.88; 95% CI, 1.04-3.43), which was confirmed after adjusting by sex (OR = 1.94; 95% CI, 1.04-3.63). Although not significant, Kaplan-Meier analysis showed a decreased median survival in Arg/Gln genotype carriers in comparison with Arg/Arg carriers.
Conclusions
To our knowledge, this is the first study reporting an association between BER SNP and HCC risk in a population of central-southern Italy.
Introduction
The majority of hepatocellular carcinoma (HCC) cases result from DNA damage caused by hepatitis viruses that are the main potential risk factors for the development of HCC (1). Damage due to endogenous or exogenous exposure may be repaired by enzymes encoded by the DNA repair pathways, such as base excision repair (BER), nucleotide excision repair (NER), mismatch repair (MMR), homologous recombination repair (HRR) and nonhomologous end joining (NHRR). Polymorphisms in DNA repair genes may influence the individual DNA repair capacity, which is crucial for preventing genomic instability and, in turn, may be associated with higher risk of cancer (2). This variable DNA repair capacity correlates with peculiar characteristics such as those expected for cancer susceptibility genes: The proteins encoded by these alleles exhibit reduced rather than absence of function, and this impairment may increase the disease risk. The genes involved in DNA repair can carry some polymorphisms, and the different alleles exhibit incomplete penetrance (3). Among the various DNA repair pathways, BER plays a key role in the removing of DNA damage deriving from exposure to various endogenous and exogenous carcinogens. The BER pathway removes alterations of a single oxidized, reduced or methylated base (4). A potential role for DNA repair genes in hepatocarcinogenesis has been underlined in a recent study showing that transcription of most of these genes was up-regulated in cirrhotic liver of HCC-bearing patients (5).
The X-ray repair cross-complementing group 1 (XRCC1) protein plays a central role in DNA repair pathways (6). XRCC1 gene is located on chromosome subband 19q13.2 with a sequence length of approximately 32 kb, consisting of 17 exons encoding a 70-kDa protein (633 amino acids) (6).
Several polymorphisms in the XRCC1 gene have been described, including Arg399Gln (rs25487) that was signicantly associated with higher levels of DNA adducts, somatic mutations, sister chromatid exchanges and chromosomal damage. These variations could alter XRCC1 function, diminish repair kinetics, resulting in altered efficiency of the protein: As a final effect, a possible induction of the cancer development may occur. Several studies have explored the impact of XRCC1 Arg399Gln polymorphism in various cancers including lung, gastric, esophageal, breast and prostate, as well as gliomas (7–11). However, association studies of XRCC1 Arg399Gln polymorphism in HCC risk have found conflicting results (12–14). XRCC1 genetic polymorphisms could be associated with increased risk of various neoplasms such as head and neck, bladder, breast or lung cancers (15–18). Few studies have evaluated XRCC1 polymorphisms among HCC patients, and it is not clear whether a specific XRCC1 genotype could effectively modulate the risk for HCC (19–21). No data have been reported about XRCC1 polymorphisms and HCC risk in populations originating from Europe.
The aim of our hospital-based case-control study involving a central-southern Italian population was to clarify the effect of the XRCC1 genotypes on the risk of HCC.
Materials and Methods
Participants
Study participants were recruited among patients admitted to the Agostino Gemelli teaching hospital of the Catholic University of Rome (Italy), and eligibility was restricted to white individuals born in Italy. Cases were selected from patients with diagnosis of HCC, admitted to the outpatient liver unit of our hospital. Criteria for exclusion were secondary or recurrent tumors. We reviewed clinicopathological features such as Child-Pugh class, Barcelona Clinic Liver Cancer (BCLC) stage and etiology from medical records. The control group was randomly selected among patients admitted to the same hospital during the same period with a broad range of diagnoses, but without malignancy, chronic diseases, digestive diseases or any prior history of malignancy. Written informed consent was obtained from all study participants, after which each participant provided a venous blood sample. This study was performed according to the Declaration of Helsinki and was approved by the ethics committee of our university.
DNA samples
Genomic DNA was isolated from peripheral blood samples, collected by venipuncture, using High Pure PCR Template Preparation kits (Roche Diagnostic, USA). Extracted DNA samples were quantified by spectrophotometer at 260l group was Few stu20ing High Purcessing. DNA integrity was electrophoretically tested.
Genotyping
Genotyping of XRCC1 rs25487 was performed by high-resolution melting analysis using a LightCycler 480 system (Roche). The reaction was performed in 20 μL final volume including 10 μL of 2× Light-cycler 480 High Resolution Melting Master mix; 2.5 mM final concentration of MgCl2. The primer pairs used were forward, 5′-TAAGGAGTGGGTGCTGGACT-3′, and reverse, 5′-ATTGCCCAGCACAGGATAAG-3′. All primers were designed with Primer3 software and synthesized by Eurofins MWG Operon. Overall samples were amplified on the Roche LightCycler 480 using a touchdown polymerase chain reaction (PCR) program: 95 aC for 10 minutes, followed by 45 cycles of denaturation at 95 WC for 10 seconds, annealing starting at 62 C for 15 seconds and decreasing until 5362 denaturation at 95WG C for 1 minutes. Following the amplification steps, PCR products were denatured at 95°C for 1 minute and cooled to 40 mC so as to form heteroduplexes.
These steps were followed by a high-resolution melting program consisting of a first-step heating at 95 hC and a melting program with temperatures ranging from 65 rC to 95°C. Melting data were analyzed using the Gene Scanning module of the LightCycler 480 software (version 1.3), incorporating normalization of premelt and postmelt regions, temperature shift adjustment and calculation of difference curves. To assess how well our protocol was able to discriminate the mutant from the normal allele, the melting curve of each amplicon, deriving from the heterozygous DNA sample, was compared with that derived from same amplicon from a normal DNA sample (previously sequenced by Sanger method, in triplicate). A randomly selected pool of HRM prescreened samples (1 pool per genotype) was also sequenced for further genotype confirmation.
Statistical analysis
Adjusted odds ratios (ORs) and relative 95% confidence interval (95% CI) estimates were calculated using a conditional multiple regression model to measure the association between HCC and putative risk factors. The exact logistic regression model was also used where appropriate (22). We also examined the possible confounding effect of alcohol and chronic infection with HBV and/or HCV. However, models including these covariates yielded very similar results; thus, given the small numbers in some strata, only the age- and sex-adjusted estimates were presented. A chi-square test of Hardy-Weinberg equilibrium (HWE) for the 3 XRCC1 alleles was performed among controls. Overall survival was estimated using the Kaplan-Meier method, and subgroups were compared by the log-rank test (23). Statistical significance was defined as a 2-sided p value of less than 0.05 for all analyses, which were carried out using the Stata software package (Release 13; Stata Statistical Software, College Station, TX, USA). This paper has been written according to the Strengthening the Reporting of Genetic Association Studies (STREGA) guidelines.
Results
Our study population included a total of 89 HCC patients and 99 controls. We consecutively contacted 120 healthy individuals, who were asked to participate in this study: Only 99 (82.5%) agreed to participate, while 17.5% of them were not interested or did not have enough time to be interviewed and informed regarding the study. The clinical characteristics of our HCC patients are reported in Table I. Significant differences were found both for sex (p<0.001) and for age (p<0.001). The percentage of males was higher among HCC patients than controls (78.6% vs. 48.4%). The mean age was 66.28 years (±10.53) in HCC patients, and 83.76 years (±3.60) in controls. The age differences between the 2 groups were expected because the control group was deliberately chosen from a pool of individuals whose age excluded them from the risk of developing HCC. In fact, besides the ascertainable possible causes, HCC can also develop for reasons defined as cryptogenic. Considering that development and progression of HCC are very slow (about 20 years), it was unlikely that the individuals chosen as controls in the study would develop HCC.
Clinical features of HCC patients
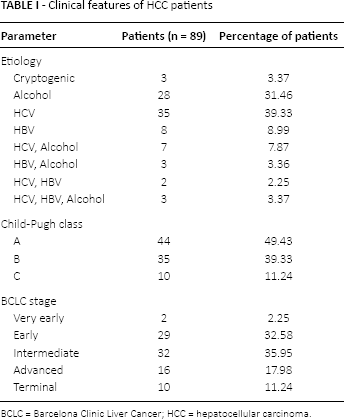
BCLC = Barcelona Clinic Liver Cancer; HCC = hepatocellular carcinoma.
Almost 50% of the HCC patients had Child-Pugh class A HCC. Among the HCC patients, 52.8% were HCV-positive, and 36% were in the intermediate BCLC stage. Statistical analysis did not find any significant association between the genotype 399Arg/Gln and susceptibility to HCC in patients with HCV/HBV or other factors (data not shown).
Table II shows the distribution of the genotypes XRCC1 Arg399Gln among HCC patients and controls. The genotype distribution was in line with the HWE among HCC patients (p = 0.18) and controls (p = 0.13). On univariate analysis, we found a statistically significant association between risk of HCC and XRCC1 399Arg/Gln genotype (OR = 1.88; 95% CI, 1.04-3.43, p<0.05) that was confirmed after adjusting by sex (OR = 1.94; 95% CI, 1.04-3.63, p<0.05); nevertheless, when adjusted by sex and age (OR = 1.66; 95% CI, 0.51-5.34, p>0.05) this association did not reach statistical significance. Although XRCC1 399Gln/Gln homozygote individuals showed a higher risk for HCC (OR = 2.34; 95% CI, 0.98-7.54) than heterozygotes, this association did not reach statistical significance, because of the low number of homozygote individuals.
Frequencies of XRCC1 Arg399Gln genotypes stratified for HCC patients and controls
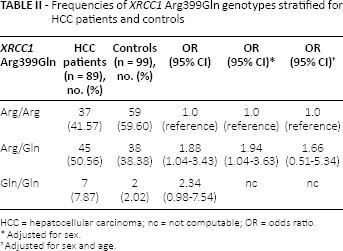
HCC = hepatocellular carcinoma; nc = not computable; OR = odds ratio.
Adjusted for sex.
Adjusted for sex and age.
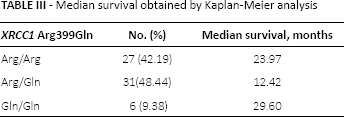
Out of 89 patients who were treated and received chemotherapy after surgery or radiotherapy with or without chemotherapy in the Agostino Gemelli hospital, 25 died within a few years from enrollment or during the treatment. Monitoring over time was possible for the remaining 64 individuals for whom we calculated that the median survival period was 20 months (SD = 21.3). Although not significant, Kaplan-Meier analysis showed a decreased median survival in Arg/Gln genotype carriers in comparison with Arg/Arg carriers (Tab. III). These findings are also shown in Figure 1.
Median survival obtained by Kaplan-Meier analysis
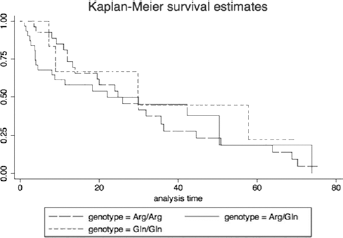
Kaplan-Meier survival curves.
There were no statistically significant differences among the 3 genotypes with regard to survival (log rank test, χ2 = 0.47, p = 0.79).
Discussion
In this study we tried to verify the possible association between XRCC1 Arg399Gln polymorphism and HCC risk in a group of Italian patients. Our study found a statistically significant association between the XRCC1 399Arg/Gln genotype and HCC susceptibility, although this was not confirmed when adjusted by age (Tab. II). To our knowledge, this is the first study regarding the analysis of a possible relationship between such a polymorphism in this DNA repair gene and HCC risk in a homogenous group of Italian patients.
Lately, some molecular epidemiological studies have been conducted to evaluate the role of this XRCC1 polymorphism in cancer risk; however, the results remain contradictory rather than conclusive (24–30). In particular, the Gln/Gln genotype of the Arg399Gln polymorphism was associated with an increased risk of nasopharyngeal (31) and prostate cancer (32, 33), while the same polymorphism was shown not to be correlated with gastric (34), colorectal (35) and skin (36) cancer susceptibility. In contrast, in an Indian cohort, a significant association between between HCC and the Gln/Gln genotype (shown to be a protective genotype against HCC) was reported by Kiran et al (12). However, in different white HCC patient groups, Borentain et al (37) and Long et al (21) showed an increased frequency of Arg/Arg genotype, while Kirk et al (20) found similar findings in an African population. Finally, while the meta-analysis published by Xie et al (38) did not find any association between the XRCC1 Arg399Gln polymorphism and HCC susceptibility, the recent meta-analysis by Qi et al (39) suggested that the XRCC1 Arg399Gln genotype was associated with a significantly increased risk for HCC in a codominant model. The exact mechanism through which the Gln allele could influence the development of HCC still remains unclear.
We underline the fact that limited reports on the role of XRCC1 Arg399Gln polymorphism on the survival of cancer patients (40–44) are present in literature. In this regard, following up 64 HCC patients, we found a decreased median survival period in Arg/Gln genotype carriers: we can speculate that this could be due to reduced enzyme activity and decreased DNA repair capacity. However, the limited number of Gln/Gln patients reduced the statistic power of this result.
Since this is preliminary report, our study is affected by the following limitations: (a) although there are 3 common single-nucleotide polymorphism (SNP) sites in the XRCC1 gene, and haplotype analyses could increase the power of the statistical analysis, a careful review of the literature leads us to analyze only the XRCC1 Arg399Gln polymorphism (14, 45–48); (b) despite the fact that our analysis has shown no significant correlation between the XRCC1 Arg399Gln polymorphism and susceptibility to HCC in HCV-positive patients, as confirmed in previous studies (14), further analysis are needed to evaluate if HCV-positive status could be a significant variable in HCC patients
In conclusion, despite all of the limitations reported above, our study suggests that the 399Arg/Gln genotype in the XRCC1 gene is significantly associated with risk of HCC in a central-southern Italian population group. To better clarify the role of this variant in HCC risk, larger cohorts of patients, possibly in a multicenter study including whites and African Americans, are needed.
Footnotes
List of abbreviations
Financial support: Funding for this study was received from the Erasmus Mundus Western Balkans Fellowship (to B.N.).
Conflict of interest: The authors declare they have no conflict of interest.