
Abstract
Background
CD133-positive melanoma cells are thought to be melanoma-initiating cells with cancer stem cell (CSC) characteristics. Some researchers have reported that CD133-negative subsets can also initiate tumors, so the clinical significance of a CD133-positive subpopulation of cells in melanoma remains controversial. This systematic review was designed to assess the value of CD133 as a CSC marker in melanomas. A meta-analysis was also performed to cumulatively analyze the data on CD133 expression levels in the selected studies.
Materials and Method
Eligible studies were identified via an electronic search through various databases including PubMed, MEDLINE, Ovid MEDLINE, and Web of Science (from May 2005 through September 2014) using the following keywords: “CD133 or prominin-1”, “cancer stem cells”, and “melanoma”. Only articles in which CD133 antigen was detected by immunohistochemistry (IHC) were included. A meta-analysis was performed to identify any association between CD133 expression and clinical outcomes.
Results
Two hundred and ninety-nine melanoma cases from 5 studies were evaluated for expression levels of CD133 using IHC. Large heterogeneity was observed among the results (p<0.001, I2 = 94%). Approximately 47.9% (95% CI 23.7%-72.1%) of the studied melanoma cases had high CD133 expression. The I2 value and Q-test p value for heterogeneity were 89.0% and <0.001, respectively, and the pooled estimate of CD133 expression was 61.7% (95% CI 25.1%-98.4%).
Conclusions
Our findings suggest that CD133 is not yet proven to be an appropriate biomarker in identifying CSCs of melanoma. Thus, detection of CD133 in combination with other putative CSC markers may be more valuable for clinical application.
Introduction
Melanoma is the sixth most common skin cancer in the United States and its incidence has been on the rise in industrialized countries and worldwide (1). Currently, 2-3 million nonmelanoma skin cancers and 132,000 melanoma skin cancers are diagnosed around the world each year (2). Despite the treatment strategies available for melanoma, the relapse rate is still high and only few patients achieve long-term survival (3).
The cancer stem cell model proposes that a fraction of cells within tumors, the so-called cancer stem cells (CSCs), confer the capacity of self-renewal, differentiation, tumor initiation, metastasis, recurrence and resistance to treatment (4, 5). CSCs have been identified in various malignancies including acute myeloid leukemia, breast cancer, glioblastoma and melanoma (6-7-8-9).
The first evidence for the importance of melanoma stem cells (MSCs) was shown in 2005, when Fang et al (10) transferred CD20-positive melanoma cell lines into mouse embryonic fibroblasts and observed stem-cell-like properties. Other studies have also isolated pluripotent dermal stem cells (DSCs) from the dermal region of neonatal foreskin, which had self-renewal capacity and expressed the neural crest stem cell markers NGFRp75 and nestin (11). It has also been reported that DSCs can differentiate into various cells including mesenchymal and neuronal lineages and melanocytes, and transform to malignant melanoma after UVA radiation (11, 12). MSCs express various surface markers (5, 13) including CD20 (10); ABC transporter family members such as MDR1, ABCG2 and ABCB5 (14-15-16-17-18); CD271 (19, 20); nestin (21, 22); CD44 and CD133 (23).
Among these markers, CD133 (also known as prominin-1/AC133), a member of the pentaspan transmebrane glycoproteins with a molecular weight of 120 kDa, is considered to be the most important surface marker for identification of MSCs (5, 12, 17, 23-24-25-26-27-28-29). Monzani et al (17) proposed CD133 as a potential MSC marker for both in vivo and in vitro studies. They showed that melanoma tumor biopsies contain a subset of cells expressing CD133. CD133-positive melanoma cell lines showed tumorigenic potential following injection into NOD-SCID mice (10, 17, 18). Klein et al (23) observed increased expression of CD133, CD166 and nestin in primary and metastatic melanomas compared to benign nevi. Porta et al (30) proposed multiple biomarkers including CD133, CD20 and ABC transporter family members for the identification of MSCs. Other investigators have also found that high tumorigenicity and metastatic potential of melanoma cells can be attributed to the high level of CD133 expression (27). Cumulative evidence has indicated that CD133 promotes the metastatic process via interaction with signaling pathways which affect cell polarity and migration (24, 31). The chemotherapy resistance of advanced-stage melanoma is related to a subset of CD133-positive melanoma-initiating cells (MICs) (18). Overexpression of the stem cell markers CD133 and nestin has been reported in metastatic melanoma biopsies as compared to primary lesions and/or benign nevi (23). It has also been shown that CD133 is expressed in hematopoietic stem cells, endothelial cells of microvessels, and endothelial progenitor cells, as well as in many melanoma cases with capability of differentiation into neural cells (23). However, some studies have shown that CD133 expression is not restricted to stem cells, and both CD133-positive and CD133-negative subsets of brain, colon and lung cancers initiate tumors including melanoma (28, 32-33-34). Therefore, the tumor-initiating potential of a CD133-positive subpopulation in melanoma is still not quite certain. In the current study, we conducted a systematic review and meta-analysis of the CD133 expression in melanoma patients in order to assess the value of CD133 as a CSC marker in melanoma and to determine the potential clinical significance of CD133 based on the available data.
Materials and methods
Search Strategy
Publications were identified in different databases including PubMed, MEDLINE, Ovid MEDLINE and ISI Web of Science from May 2005 through September 2014. The following search terms were used for the PubMed search: (melanoma [all fields] OR neoplasm [MeSH terms] OR skin cancer [MeSH terms]) AND (cancer stem cells [all fields] OR tumor-initiating cell [MeSH terms]) AND (CD133 [all fields] OR AC133 [MeSH terms] OR prominin-1 [MeSH terms]).
Study Selection Criteria
Titles and abstracts were reviewed by 3 independent researchers (ZM, EG and EE), then relevant papers were identified by all authors and were further evaluated according to the predefined inclusion/exclusion criteria. The inclusion criteria were 1) only articles that had assessed CD133 in melanoma using IHC; 2) articles that had detected CD133 as a tissue marker; 3) articles providing sufficient data to allow the estimation of an odds ratio (OR) or a relative risk (RR) or hazard ratio (HR) or through personal communication with authors of the articles with incomplete data; 4) articles limited to the English language and published as original research during 2005-2014. Accordingly, non-English-language publications, review papers, any type of articles other than original research, duplicate research articles, research protocols, commentaries, editorials, letters, and books were excluded from the systematic review (Fig. 1).
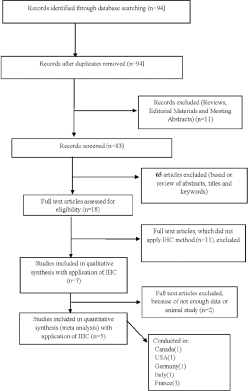
Flow diagram of the study selection in the systematic review.
Data Extraction
Two coauthors (EE, EG) extracted the data using a standardized data abstraction tool, which comprised basic information from each study including the purpose and design of the study, the year of publication, methodology, the main study population, CD133 expression level, survival or prognosis, and source of data. Discrepancies were discussed among 3 authors (ZM, MA and MM) if the abstract was unclear regarding the above parameters. Specific parts of the included papers were then entered in a standard table.
Statistical Analysis
This systematic review and meta-analysis was designed in accordance with the PRISMA statement consisting of a 27-item checklist and a 4-phase flow diagram. Statistical analysis was performed with the Stata 13.1 software (StataCorp). We used meta-analysis to report a pooled estimate for CD133 expression in melanoma. Heterogeneity across studies was evaluated by the Q test and p values (Cochran's Q test, p>0.1 or I2>50%). Pooled estimates for CD133 expression were calculated by a random-effects model.
Results
Search Results
Based on the search strategy, the different databases were checked and a total of 94 articles were identified. Detailed search steps are described in Figure 1. From these articles, 11 were excluded including 5 review articles, 3 editorial materials, and 3 meeting abstracts. Of the 83 remaining published studies, 65 articles were excluded (based on review of abstracts, titles and keywords) and only 18 studies remained for further evaluation. In a further assessment, 11 articles were excluded because they had not used IHC and 2 studies were excluded because they involved animals or did not have enough data for meta-analysis. Eventually, 5 nonduplicated studies met the predefined inclusion criteria for meta-analysis including 299 cases (21, 22, 24, 35, 36). The selected studies were published between 2010 and 2013. All these studies evaluated the expression of CD133 using IHC; 2 of them presented prognostic data of melanoma tumors and 3 studies contained follow-up data and survival information.
Characteristics of Eligible Studies
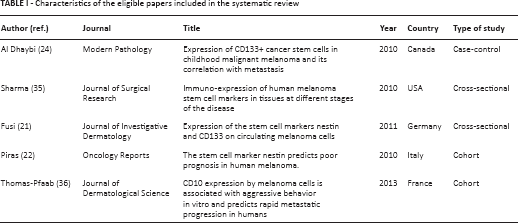
The 5 eligible studies are listed in Table I; the total number of patients was 299, ranging from 6 to 138 cases per study. Four studies applied 5-micron sections of whole tissue (21, 22, 24, 35) and only 1 study utilized tissue microarray (TMA) for IHC staining (36). The results of the included studies are summarized in Table II.
Characteristics of the eligible papers included in the systematic review
Summary of included studies
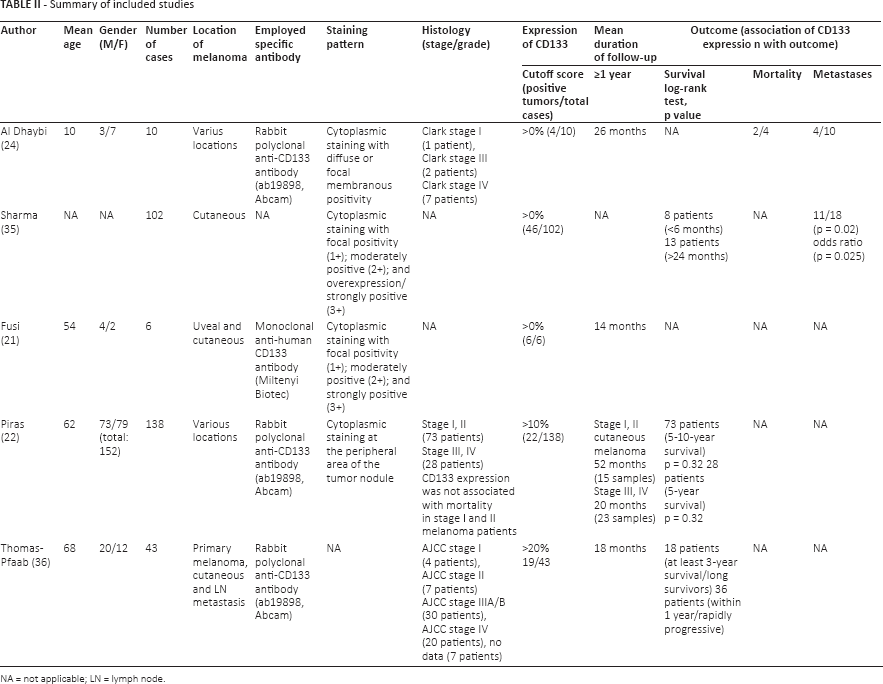
NA = not applicable; LN = lymph node.
In Al Dhaybi's study (24), 12 cases of childhood malignant melanoma and 12 control cases of Spitz nevi were evaluated. Two patients were excluded due to insufficient pathology specimens and lack of follow-up data. CD133 was positive only in 4/10 tumors with Clark III and IV stages. Three patients had lymph node metastasis, whereas 1 patient had multivisceral metastasis. Two patients died of their disease 25 and 17 onths after the diagnosis. No metastasis was observed in 6 CD133-negative tumors (24).
The Sharma et al study (35) involved 111 specimens including primary melanoma (n = 40), lymph node metastasis (n = 32), distant metastasis (n = 19), and benign nevi from patients with a past history of melanoma (n = 11) and from nonmelanoma patients (n = 9). Higher expression of CD133 was observed in lymph node and distant metastatic lesions (p<0.0022, p<0.013) in comparison with benign nevi from nonmelanoma patients. Differences were more significant in lymph node (p<0.0149) than distant metastases (p<0.057) compared to nevus lesions from patients with a past history of melanoma (35).
In the study by Fusi et al (21), CD133 and nestin expression in circulating melanoma cells were compared with the expression levels of these proteins in metastatic tissues from 6 patients with metastatic lesions using IHC. The authors found comparable expression levels of these molecules in circulating melanoma cells and metastatic tissues. CD133 expression did not show any correlation with known unfavorable prognostic factors, nor was it associated with a shorter overall survival (21).
Piras et al (22) studied 130 primary tumors and 32 nodal metastasis biopsy specimens and compared the results with survival and clinicopathological data using the IHC technique. Twenty-four paraffin sections were not available and excluded. Complete clinical data including follow-up until April 2008 were available for 73 patients with AJCC (American Joint Committee on Cancer staging system) stage I and II tumors and for 28 patients with AJCC stage IV melanoma. CD133 expression was not associated with mortality in patients with AJCC stage I and II melanoma. No statistically significant difference in CD133 expression was found between primary and metastatic tumors. Similarly, no significant correlation was observed between CD133 expression and clinicopathological variables or between the survival rate of patients and CD133 expression. Decreased survival in patients with advanced disease was associated with CD133 expression in nodal metastatic lesions (p = 0.008) (22).
In the study by Thomas-Pfaab et al (36), 68 tumors from 32 patients were assessed by IHC (using TMA) for evaluation of CD10, CD20, CD133 and nestin expression. Patients were divided into 2 groups according to their clinical outcome profile including a “rapidly progressive” and a “long survivor” group. Four samples were from patients with AJCC stage I, 7 from patients with stage II, 30 from patients with stage IIIA/B, and 20 from patients with stage IV melanoma; no data were available for 7 patients. Twenty-one tumors were primary melanomas, 25 metastatic lymph nodes, and 22 cutaneous metastases. Thirty-two tumors displayed positive CD10 staining, 19 were positive for CD133, and 50 were positive for nestin. None were positive for CD20 staining. Seventeen tumors were positive for both CD133 and nestin. In the mentioned study, the overall survival and disease-free survival in CD133- and/or nestin-positive melanoma patients were not significantly different from those in CD133-negative melanoma patients. There was no significant difference regarding survival and clinical outcome in patients with nestin or CD133 expression and nestin/CD133-negative patients, whereas CD10 expression was significantly associated with a lower survival rate (36).
Meta-Analysis Results
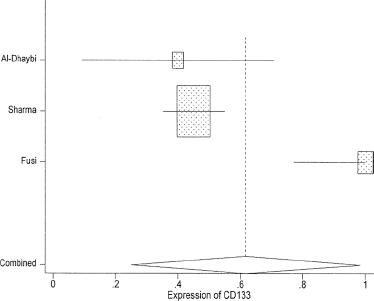
The heterogeneity of the combined results of the 5 studies was evaluated by graphical examination of the forest plots. Statistical evaluation was then performed using the inconsistency index (I2) and Q test p value statistics (37, 38). There was large heterogeneity between the results of the various studies (p<0.001, I2 = 94%). We pooled CD133 expression by a random-effects model using 95% confidence intervals (CIs). Approximately 47.9% of melanoma cases had CD133 expression (95% CI: 23.7%-72.1%) (Fig. 2). Selecting Cells>0 as the inclusion criterion, there were 3 eligible studies (Fig. 3). The I2 and Q test p value for heterogeneity were 89.0% and <0.001, respectively. The pooled estimate of CD133 expression was 61.7% (95% CI: 25.1%-98.4%).
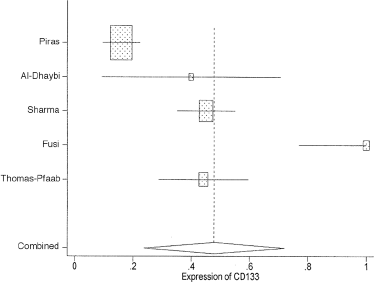
Meta-analysis (with 95% confidence intervals) of CD133 expression in melanoma for the individual studies and all 5 studies combined.
Meta-analysis (and 95% confidence intervals) of CD133 expression in melanoma for 3 eligible studies (with Cells>0 as the inclusion criterion) and all 3 studies combined.
Discussion
To our knowledge, this systematic review and meta-analysis is the first in English to evaluate the significance of CD133 as a putative CSC marker in melanoma. The first evidence for the role of stem cells in melanoma pathogenesis was obtained in 2005, when Fang et al (10) transferred melanoma cell lines into mouse embryonic fibroblasts and observed stem-cell-like properties. These cells can be distinguished by their capacity for spheroid formation, self-renewal activity, tumorigenesis, metastasis, and resistance to chemotherapy (39, 40). Also, chemotherapy resistance of human malignant melanoma is attributed to MICs or MSCs existing in melanoma cell lines and in clinical melanoma biopsies (14, 40-41-42). It was shown that melanoma cell lines express a variety of stem cell markers with various expression levels, which include CD133 (10, 18). CD133 has been applied broadly as a marker for detection and isolation of CSCs in many cancers (9, 37, 43, 44). Although the exact biological function of CD133 remains unclear, it is considered a putative CSC marker in various cancers (9, 37, 43-44-45). The prognostic role of CD133 in cancer patients and its association with poor prognosis has also been recognized in colorectal cancer, gliomas, gastric cancer, and hepatocellular adenocarcinoma (2, 46-47-48-49). Since some recent meta-analysis studies on various tumors including colorectal (38), ovarian (50) and lung (51) cancer reported the tumor-initiating potential of the CD133-positive subpopulation as a CSC marker, in the present study we aimed to evaluate the frequency of CD133 expression in melanoma patients in the individual studies and then in the pooled data of all studies combined. Through analyzing the data from 5 eligible studies involving 299 melanoma cases, CD133 was found to have a 61.7% (95% CI: 25.1%-98.4%) expression rate with the IHC technique, which showed considerable heterogeneity amongst studies. Al Dhaybi et al (24) reported that the expression of CD133 as a CSC marker correlates with poor prognosis in melanoma; positive expression of this marker was observed in all malignant and metastatic melanoma patients. Their results confirmed that CD133 was expressed more in metastatic than primary melanoma lesions. In another study using IHC, increasing expression levels of CD133 were observed when lesions progressed from Spitz nevi to primary and then metastatic melanomas (23).
Although the expression of CD133 is not restricted to CSCs, due to the lack of a tissue-specific marker for CSCs in most tumor types a combination of markers has been suggested for identification of CSCs. Besides CD133, several other biomarkers have been found in CSCs including CD44, ALDH1, CD166 and OCT4 (23, 42). High expression of these markers correlates with worse clinical features and poor prognosis (38, 52). Klein et al (23) observed increased expression of CD133, CD166 and nestin in primary and metastatic melanomas compared with benign nevi. Also, Porta et al (30) proposed multiple biomarkers such as CD133, CD20 and ABC transporter family members for identification of melanoma CSCs. Fusi et al (21) evaluated the expression of nestin and CD133 as stem cell markers in circulating melanoma cells and melanoma tissues and confirmed the presence of these markers in metastatic lesions. CD133 and nestin expression profiles in CMCs were identical to matched metastatic tissue sections, suggesting that these CSC markers can be applied as a detection tool in circulating melanoma cells as well as tissue CSCs. The authors proposed nestin as an appropriate melanoma marker, whereas CD133 did not show any correlation with unfavorable outcome in patients with metastatic cutaneous and uveal melanomas (21). In another study by Piras et al (22), no significant difference was observed in nestin or CD133 expression between primary tumors and metastatic lesions. Furthermore, CD133 expression was not associated with survival and mortality in early stages of melanoma, while nestin was found to be an important early marker for survival in melanoma patients (22). In the study by Sharma et al (35), increased expression of CD133 along with CD166 and nestin was found in the advanced stages of melanoma, and coexpression of these markers was suggested to be applicable for CSC detection, although the exact role of CD133 expression in melanoma outcome was not elucidated. In contrast to the Fusi, Piras, and Sharma studies, our recent report on the clinical significance of CD133 and nestin in skin tumors indicated that the coexpression of these CSC markers correlates with aggressiveness and metastasis (53). Additionally, these markers were overexpressed in melanoma compared to squamous cell carcinoma and basal cell carcinoma (53). Concerning the clinical importance of combined CSC markers in other cancers, Horst et al (46) showed that a combination of CSC markers including CD133, CD44 and CD166 could be more helpful in differentiating high-risk from low-risk colorectal cancer. In a study by Thomas-Pfaab et al (36) on the role of the CSC markers CD133, nestin and CD10 in metastatic progression of melanoma, no significant correlation was observed between CD133 and nestin expression and clinical outcome, suggesting that these markers may not be used as robust clinical factors in melanoma.
Though the results from some studies pointed to a positive correlation between the CD133 CSC marker and melanoma, some controversies still exist. First, although CD133 may be a candidate marker for melanoma, individual studies had low power in detecting a significant association between CD133 expression and progression of melanoma, and many studies emphasized the application of combined CSC markers in studying melanoma and other cancers; these included CD133 and ABCG2 in melanoma (17); CD133 and CD44 in pediatric solid tumors (54); and CD133, OCT4 and SOX2 in rectal cancer (55). Second, previous studies showed CD133 expression in some primary melanoma cell lines but not in all metastatic cell lines (56). Third, it seems that the correlation between high CD133 expression and progression of melanoma would be highly significant when the coexpression of 2 or more markers is studied. Although the CD133-positive subpopulation is considered as CSCs in a variety of human cancers, CD133-negative cells with tumor-initiating characteristics have also been reported in cancers including brain, colon and lung cancer (28, 32-33-34) as well as melanoma (57).
Several limitations of this meta-analysis should be taken into account: with only 299 cases the number of included cases was relatively small, and the included studies were technically heterogeneous (for example regarding the antibody dilutions). Thus further, larger clinical studies are required to evaluate the relation between CD133 expression as a CSC marker and progression of melanoma.
Footnotes
Abbreviations
Financial support: This study was supported by a grant from Iran University of Medical Sciences (grant number #22741).
Conflict of interest: There is no conflict of interest related to this article.