
Abstract
Purpose
Adequate biomarkers are still required to optimize therapy in patients with locally advanced head and neck squamous carcinomas (HNSCC) treated with chemoradiotherapy (CRT).
Methods
We updated the follow-up of 66 HNSCC patients treated with CRT we described more than 10 years ago, focusing on SNP Arg/Pro (R/P) at codon 72 and somatic mutations in TP53 and on SNP309 in the MDM2 gene.
Results
In wild-type TP53 cases, overall survival (OS) was longer in 72RR and less favorable in 72PP (p = 0.005); when TP53 was mutated, OS was longest in 72PP and less favorable in 72RR and 72RP (p = 0.058). Median OS was significantly shorter in patients with MDM2 SNP309 GG or GT genotypes compared with the TT genotype (p = 0.002).
Conclusions
TP53 SNP72 may be useful in selecting patients for CRT, but has to be related to somatic TP53 mutations. The MDM2 SNP309, easily determined in peripheral blood, might be more convenient as a predictive biomarker.
Introduction
The management of head and neck squamous cell carcinoma (HNSCC) remains an important clinical challenge. HNSCC is the sixth most common cancer in the world and accounts for 4% of all malignant neoplasms in Italy (1). Although early-stage disease is curable with surgery or radiation therapy, more than 60% of patients present with locally or regionally advanced disease (stage III-IV) (1). For such patients the treatment failure rate after surgery and/or radiotherapy is high and the survival poor.
Despite improved local control and overall survival (OS), optimal protocols for the administration of combined-modality treatments (combining radiation and chemotherapy) have not been definitively identified in HNSCC, nor has it been established which subgroup of patients with advanced HNSCC will benefit from integrated treatments (2-3-4). Rapidly alternating chemoradiation is a variation of concurrent chemoradiation that is intended to minimize toxicity (5). It has led to a statistically significant improvement in outcome compared to conventional radiotherapy (6), with a more favorable toxicity profile (7, 8).
Because of the significant treatment-related toxicity associated with combined-modality regimens, it is critical to link treatments to molecular predictors that maximize the therapeutic antitumor effect and minimize toxicity.
Tobacco use and alcohol abuse remain the best established risk factors, but accumulating evidence indicates that viral infections, such as HPV and EBV infections, are associated with squamous cell lesions of the oropharynx and nasopharynx, respectively (9, 10). In particular, it is accepted worldwide that HPV-related oropharynx tumors depicts a distinct molecular, clinical and pathologic disease entity (11).
In earlier work we have shown that a functional single-nucleotide polymorphism (SNP) in the apoptosis-signaling domain of TP53 (R/P at codon 72) influences the clinical response of HNSCC to chemotherapy in cases with mutant and wild-type (wt) TP53 (12, 13).
In squamous cell carcinomas as well as other solid tumors, mutations occurring in the arginine allele (72R) are detected more commonly than those in the proline allele (72P) (12, 14-15-16-17). Many studies have also shown that 72R is more active than 72P in inducing apoptosis (18). Due to its effects as a modulator of TP53 mutant function, it is an interesting possibility that treatment outcome in human cancer is influenced by this polymorphism (16). In particular, we have already demonstrated that clinical response following cisplatin-based chemoradiotherapy (CRT) for advanced HNSCC is influenced by this polymorphism: cancers expressing 72R mutants have lower response rates than those expressing 72P mutants (13).
Furthermore, the stability of the TP53 protein is regulated by the E3 ubiquitin ligase MDM2 protein (mouse double minute 2 homolog). The SNP309 T>G in the promoter region of this gene influences the protein levels (19).
In a more recent study, we showed that the MDM2 SNP309 is indeed highly predictive of outcome, irrespective of mutant or wt TP53 status, and retains independent predictive power compared with recognized clinicopathological variables (20).
In the present study, we investigated the correlation of somatic mutations and polymorphisms in the TP53 and MDM2 genes with clinical outcome in platinum-treated locally advanced HNSCC patients with more than 10 years’ follow-up, partially described in previous articles (12, 13).
Material and methods
Patients and Tumors
We analyzed 66 cases of patients with locally advanced, inoperable, stage III/IV HNSCC who had been referred to the Medical Oncology Department of Cuneo Teaching Hospital between May 1997 and May 2002. The clinical-pathological and molecular characteristics of the patient population had been partially described previously (12, 13, 20) and are summarized in Table I. All patients were heavy smokers (median 45 pack/year) and were homogeneously treated with a combined approach consisting of alternating CRT, as detailed by Merlano (5).
Clinicopathological and molecular characteristics of head and neck cancers
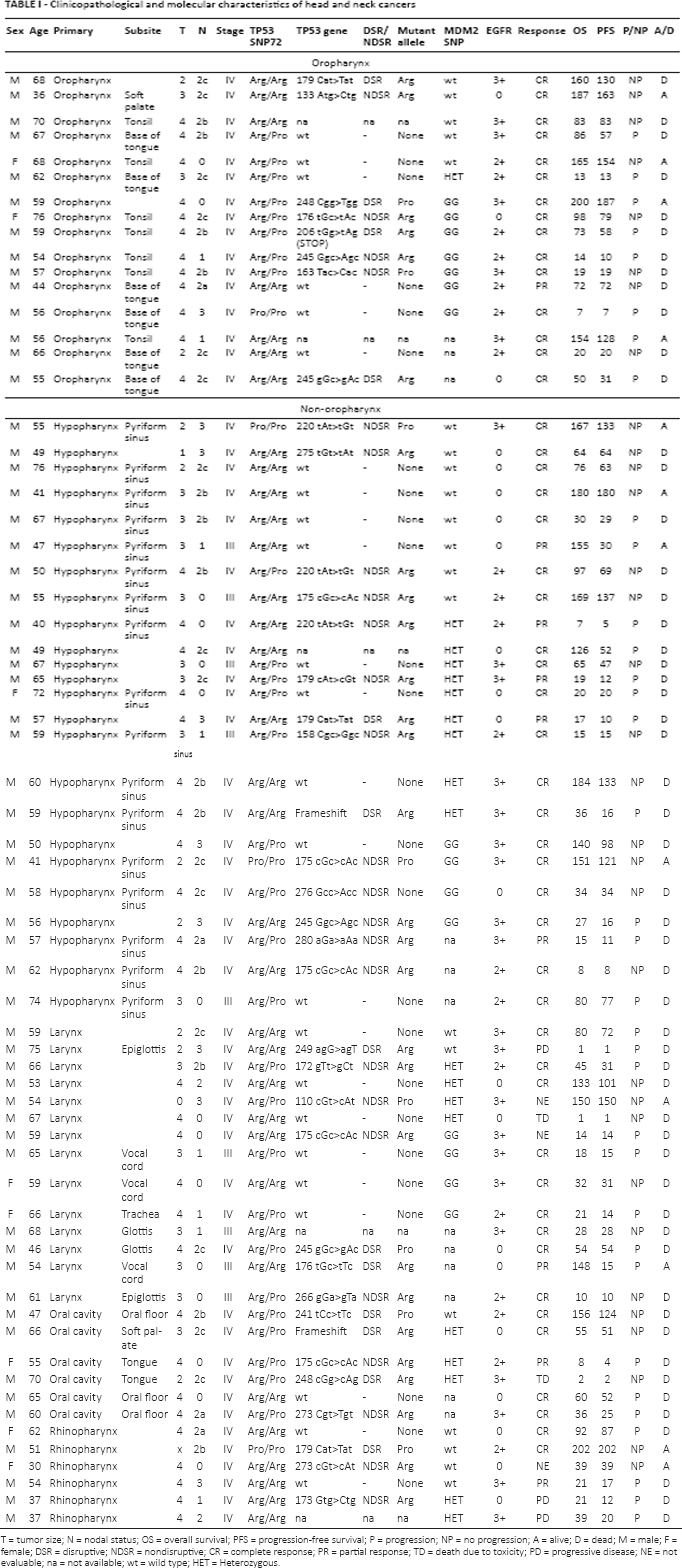
T = tumor size; N = nodal status; OS = overall survival; PFS = progression-free survival; P = progression; NP = no progression; A = alive; D = dead; M = male; F = female; DSR = disruptive; NDSR = nondisruptive; CR = complete response; PR = partial response; TD = death due to toxicity; PD = progressive disease; NE = not evaluable; na = not available; wt = wild type; HET = Heterozygous.
This work was carried out in accordance with the code of ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans. Informed consent for tissue collection and use for scientific purposes was obtained from each patient enrolled in the study.
Analysis of TP53 and MDM2
TP53 mutations and SNP at codon 72 (rs1042522) in 61/66 tumor DNAs extracted from formalin-fixed paraffin-embedded (FFPE) tissue were sought by direct sequencing in the most frequently affected exons 4-10, which were individually amplified as already described (12, 20). Amplification in 5 patients failed for some exons, while SNP genotyping at codon 72 was obtained for all 66 patients.
In germline 72 RP, we identified the polymorphic allele in which the mutation occurred, in order to divide our population in wt or mutant alleles (mutant-72R or mutant-72P) (13).
The mutations were evaluated for possible functional importance at the protein level using available TP53 databases (http://p53.iarc.fr/ and http://p53.free.fr) and the published literature. In particular missense, frameshift and nonsense mutations, together with alterations affecting the splice-site regions were considered as functional mutations. Silent mutations not affecting the amino-acid sequence or located outside the exons and splice-site regions were considered not functional mutations and were allocated to the wt group.
In MDM2, the SNP at position 309 (rs2279744) was analyzed by direct sequencing after PCR amplification of genomic DNA for the 54 patients in whom blood was available for this purpose, as already described (12, 13, 20).
Egfr Expression
EGFR was detected in all patients by immunohistochemistry (IHC) using the EGFR pharmDx™ kit (Dako) and quantified according to FDA guidelines on a scale from 0 to 3+.
HPV16 and p16 Expression
Due to the lack of adequate tissue slides of the oldest cases, HPV16 and p16 were investigated in half of the patients (33/66: 50%) by PCR and IHC, respectively.
HPV was searched using specific primer pairs for the E1 gene of HPV type 16 (NCBI Ref. Seq: NC_001526.2, clone 114/K): E1 forward 5’-GAGATGCAGTACAGGTTCTAAAACG-3’ and E1 reverse 5’-TGCCATACCCGCTGTCTTC-3.
IHC staining for p16 was performed on 4-micron sections from FFPE tissue blocks mounted on glass slides, using prediluted ready-to-use monoclonal antibodies: clone E6H4 (MTM Laboratories) on a Ventana Benchmark ULTRA automated immunostainer. Positivity for p16 was defined as ≥70% positive cells.
Statistical Analysis
OS and progression-free survival (PFS) curves, according to TP53, MDM2 and EGFR status, were calculated using the Kaplan-Meier life-table method; the log-rank test was used to evaluate the statistical significance. OS was defined as the time from treatment start to death from any cause. Surviving patients were withdrawn at the last follow-up or at the last contact. PFS analyses were based on the time from treatment start to the first event (locoregional recurrence, distant metastasis); patients without an event were censored at their last follow-up.
The comparison was done between 2 groups using the chi-square test, with Yates’ correction or Fisher's exact test when appropriate. Fisher's 2-tailed exact test was used to calculate p values for the 5-year survival rates. For all statistical tests a significance level of 0.05 was used. All of the reported p values are 2-sided.
Multivariate Cox proportional hazards stepwise analysis was carried out using binary variables with 95% confidence intervals (CI) and was performed using SPSS version 13. However, due to the low number of HNSCC patients, stratification by primary site was not possible. Moreover, HPV16 and p16 results were excluded from the analysis and not used for any correlation studies since half of the FFPE samples were no longer available.
All the other variables with clinical significance were included in the model and a backward regression analysis was used to identify those factors that significantly affected the risk of death. Since evaluation of the validity of different prognostic factors for survival was the main objective of the study, we kept these factors in the model and applied the backward regression analysis to the other covariates.
When the multivariate analysis did not obtain an overall p value of <0.05 we excluded from the analysis the parameters without statistical significance in the Kaplan-Meier analysis.
Results
Description of TP53 SNP and Mutations in Patient Population
The clinicopathological and molecular data on SNP72 and the mutational status in TP53 are reported in Table I, where patients are grouped by primary tumor site.
At the time of this second analysis, 82% of patients had died (54/66). The median time to death was 4.5 years (95% CI 2.0-7.1). The distribution of the SNP72 genotypes in the 66 cases was RR = 51.5% (34/66), RP = 42.4% (28/66), and PP = 6.1% (4/66), not different from that in the general population: RR = 53.7%; RP = 38.3%; PP = 8% (p = 0.74) (21).
Mutations in the TP53 gene were detected in 60.7% of patients (37/61). Most of the mutations (92%, 34/37) were missense (MS); 1 patient had a nonsense (NS) mutation and 2 had frameshift mutations. Overall, in line with data in the published literature (22), 21% (13/61) were disruptive and 39% (24/61) were nondisruptive mutations (Tab. I).
Twenty of the 24 patients with wt TP53 (83%) experienced a complete response (CR) to treatment, whereas this happened to only 25 of the 37 patients with TP53 mutations (68%). The difference was not significant (p = 0.14).
The presence of mutations resulting in dysfunctional TP53 was not significantly related to any patient, tumor or biological/molecular parameter except age, with a significant difference between the wt and mutant groups of patients (chi-square test p = 0.02) (Tabs. II and III).
Prognostic factors in patients with wild-type versus mutant TP53
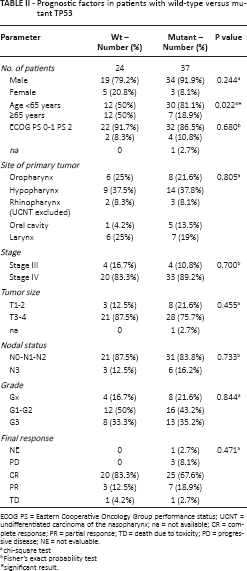
ECOG PS = Eastern Cooperative Oncology Group performance status; UCNT = undifferentiated carcinoma of the nasopharynx; na = not available; CR = complete response; PR = partial response; TD = death due to toxicity; PD = progressive disease; NE = not evaluable.
chi-square test
Fisher's exact probability test
significant result.
Biological prognostic factors in the wild-type versus mutant patients’ group (n = 61)
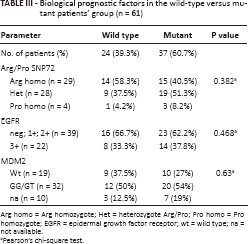
Arg homo = Arg homozygote; Het = heterozygote Arg/Pro; Pro homo = Pro homozygote; EGFR = epidermal growth factor receptor; wt = wild type; na = not available.
Pearson's chi-square test.
Role of Codon 72 Polymorphism and TP53 Mutation as Predictive Biomarker
Clinical outcome in head and neck cancer is influenced by TP53 polymorphism
Taking the whole patient population (n = 66), there was no significant difference in OS between germline 72RP genotypes (p = 0.09), although a trend was observed towards more favorable OS in individuals with 72PP (n = 4) (Fig. 1A; median OS not reached). Intermediate OS in 72RR (n = 34) (median OS 5 years) and less favorable OS in 72RP (n = 28) (median OS 3 years) were also observed.
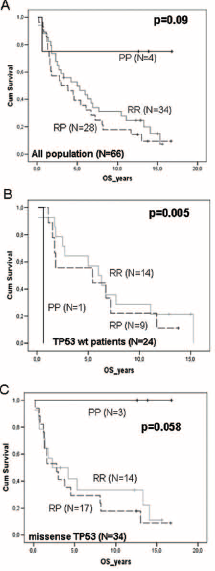
Effect of TP53 RP SNP72 on overall survival (OS) is dependent on TP53 mutational status. The Figure shows the Kaplan-Meier analysis of OS as a function of TP53 RP SNP72 in the whole patient population (n = 66) (
In the 24 cases with wt TP53 (Fig. 1B), OS was shortest in patients with 72PP (median OS 0.6 versus 6.0 years in 72RR; p = 0.003). In individuals with 72RP, OS was intermediate (median OS 5.4 years) between 72RR (p = 0.57) and 72PP (p = 0.02).
Clinical Outcome and TP53 Missense Mutations
In the 34 patients with MS TP53 mutations, OS was longest in the 3 patients carrying 72PP (no statistics were computed because none of the patients had any events) and less favorable in the 17 patients carrying 72RP (Fig. 1C; median OS 2.8 years; log rank p = 0.058). In 14 individuals with germline 72RR we observed a behavior similar to that of individuals with the 72RP genotype (median OS 3.2 years, RR versus RP p = 0.55). Patients with NS and frameshift mutations were excluded.
Identification of Both 72P and Mutation in the same allele is a Predictive Biomarker of Clinical Outcome
Survival curves split by the presence (n = 37) or absence (n = 24) of mutations did not show any statistical significance in relation to OS or PFS (log-rank p = 0.91 and p = 0.97, respectively; Fig. 2A and 2B).
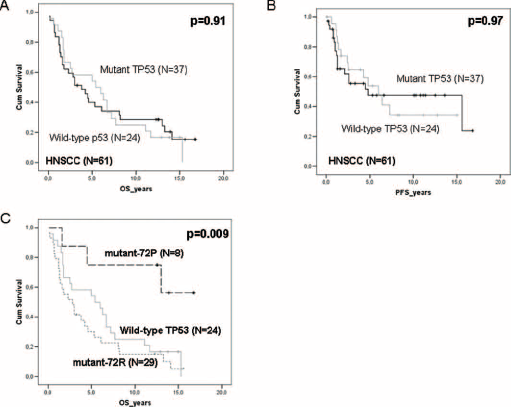
Clinical outcome in head and neck cancer is influenced by TP53 mutations in relation to RP SNP72. Survival curves for all patients analyzed only by the presence or absence of mutations did not show any significant difference in overall survival (OS) or progression-free survival (PFS) (log-rank p = 0.91 and p = 0.97, respectively) (
In cancers carrying TP53 mutations (n = 37), mutations were detected more commonly in the 72R allele: 29 mutations in 72R and 8 mutations in 72P (Tab. I). Patients with mutations in the 72P allele had a significantly longer OS than patients carrying mutations in the 72R allele. Analysis by the log-rank test of the whole population showed that TP53 mutational status and SNP72 polymorphism correlated significantly with survival (OS p = 0.009) (Fig. 2C).
When analyzing OS, we found that 37.5% (3/8) of patients with mutations in 72P had died versus 90% of patients with mutations in 72R (26/29). The median survival was not reached at 15 years in patients with 72P mutations (95% CI not reached) versus 2.8 years in patients with 72R mutations (95% CI 1.2-4.4, 72P vs. 72R, log-rank test p = 0.004; data not shown). The wt TP53 population showed an intermediate value (87.5% dead; median OS 5.7 years, 95% CI 1.1-9.7; wt vs. 72R, log-rank test p = 0.21; wt vs 72P, log-rank test p = 0.015; data not shown).
When analyzing PFS in patients with mutations in the 72P allele, we found that 37.5% (3/8) progressed compared with those having mutations in the 72R allele, 55% (16/29) of whom relapsed (median PFS 15.6 years, 95% CI 0-31.4 vs. 2.1 years, 95% CI 1.5-3.6, respectively; log-rank test p = 0.030, data not shown). The wt TP53 population showed an intermediate value of progression with 14 of 24 patients developing a relapse (58.3%) (median PFS 6 years; 95% CI 3.5-8.5). Analysis with the log-rank test on the whole population showed no significant correlation between TP53 mutational status and SNP72 polymorphism and PFS (p = 0.08, data not shown).
MDM2 SNP309 is an Independent Predictive Biomarker
Genotyping for MDM2 SNP309 was performed in 54 patients; in 51 of these patients also information on TP53 mutational status was available. The results were 27.8% GG, 35.2% GT, and 37.0% TT. Median OS was significantly shorter in patients carrying GG or GT (n = 34) compared with the germline genotype TT (n = 20) (Fig. 3A; log-rank p = 0.002).
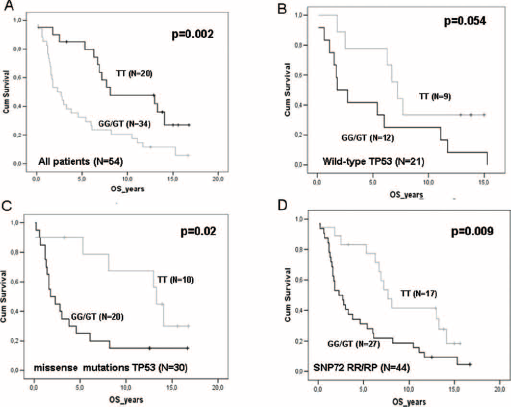
MDM2 SNP309 is predictive of outcome irrespective of TP53 genotype and mutational status. (
Interestingly, this effect was maintained regardless of the TP53 status, with a log-rank test that showed a trend in the wt subpopulation (n = 21) (Fig. 3B) and reached statistical significance in the other subgroups (Fig. 3C and 3D).
Even more interestingly, this predictive effect of the G allele was maintained independent of age, TP53 status, mutant 72P allele and EGFR grade [supplementary Table S1 – Main prognostic factors for overall survival (OS) in multivariate analysis (Cox proportional hazards model), available online at http://www.biological-markers.com].
Discussion
We performed this study to verify, with a follow-up exceeding 10 years, the influence of TP53 SNP72 on the outcome of HNSCC patients treated with CRT previously reported with a shorter follow-up (12, 13).
We are aware that in the last decade it was discovered that HNSCC with biologically active HPV is a distinct molecular entity (11, 23) and patients generally have a better prognosis (24), especially those with oropharynx tumors (11). However, in the present study, due to the small cohort of HNSCC patients (n = 66), we were not able to perform any stratification for primary sites nor for HPV infection and we analyzed the cohort as a whole.
In addition, we evaluated MDM2 SNP309 as a predictive factor in the same series of patients because of its close interaction with TP53. The TP53 gene is one of the most important players in cancer biology and it is now widely acknowledged that TP53 mutations are the most common genetic event in human cancer (25). It is less known which are the genes and proteins involved with TP53 in cancer growth, and whether some of them might be used as biomarkers to identify patients who will benefit from CRT.
In previous papers we have described how TP53 SNP72 influences outcome via functional effects on both mutant and wt TP53 (12, 13). In particular, we demonstrated that treatment outcome in patients with advanced HNSCC undergoing treatment with combined-modality CRT regimens is less favorable in cases expressing mutant 72R TP53 (13). Nevertheless, the overall predictive value of analysis of the germline SNP alone (i.e., independent of the presence or absence of TP53 mutations) is not statistically significant (20). This means that the use of TP53 R/P SNP72 as a predictive marker would require sequence analysis of TP53 in tumor tissue, which, apart from being time-consuming and expensive, is not always possible.
A limitation of our study is that we were not able to analyze the TP53 mutations found in our cohort of patients in the manner suggested by Poeta et al (22), i.e., classified as disruptive versus nondisruptive, and to correlate this with clinical outcome. The reason for this is the small number of patients analyzed and disruptive mutations found (we found 13 disruptive and 24 nondisruptive mutations).
Interestingly, this series of patients with advanced HNSCC with a follow-up longer than 10 years suggests that the analysis of both TP53 R/P SNP72 and TP53 mutation might increase the power of long-term outcome prediction. The result may be explained by the strong influence of this SNP on TP53 protein function, although with different effects, in both wt and mutated tumors.
The ring domain E3 ubiquitin ligase MDM2 is the most important negative regulator of TP53. It serves to keep TP53 levels in check under unstressed conditions (26-27-28). Additionally, also MDMX (alias MDM4), a homolog of MDM2, negatively regulates TP53 (29). Not surprisingly, both MDM2 and MDMX are overexpressed in different neoplasms (30). MDM2, which is strongly linked to TP53, has shown a particular polymorphism at position 309 of the promoter region: a T to G change (MDM2 309) that is associated with enhanced MDM2 expression and protein levels, causing attenuation of the TP53 pathway in vitro (19, 31).
We found a significant correlation between the MDM2 SNP309 genotype and clinical outcome; this is confirmed and maintained independently of other factors that might influence outcome. Thus, we demonstrated in this study and in our previous work (20) that MDM2 SNP309 is highly predictive of outcome, irrespective of whether TP53 is wt or mutant, and retains its independent predictive value compared with recognized clinicopathological and molecular variables of HNSCC such as age, stage, performance status, nodal status, EGFR and TP53 mutation.
Wan et al (32) performed a meta-analysis on cancer risk that involved 27,813 cases with various tumor types and 30,295 controls to clarify the potential interaction between MDM2 SNP309 and TP53 mutational status. The review confirmed our finding that the variant homozygote GG and the heterozygote TG were unfavorable variants in most populations (32).
In conclusion, our results strongly support the candidacy of MDM2 SNP309, determined in simple peripheral blood samples, as a robust predictive marker to stratify HNSCC patients treated with CRT.
Footnotes
Financial support: This work has been partially supported by AIRC and Fondazione Veronesi.
Conflict of interest: The authors have no conflict of interest to declare.