
Abstract
Background
p16 has been indicated as a suitable surrogate biomarker of HPV infection. The prognosis of p16-positive oropharynx tumors (OTs) of squamous cell carcinoma (SCC) histology is better than that of p16-negative tumors.
Methods
We analyzed 209 samples of head and neck SCC to establish a predictive cutoff for p16 and determine the role of p16 positivity in OTs versus non-OTs. We compared the outcomes of tumors harboring any percentage of p16-positive cells (≥1%) with those of p16-negative OTs. We then considered 3 cutoffs (10%, 50% and 70% positive cells) to evaluate the outcome of OTs/non-OTs with similar p16 expression and p16-positive versus p16-negative tumors stratified by patient age.
Results
p16-negative tumors among OTs and non-OTs were 29% and 49%, respectively (p = 0.0054). The cumulative distribution showed that the positive values were located around 2 focus points: 2% and 96%. Subgroup analysis showed that only OTs occurred in young patients (aged <65 years) and that there was a ≥70% gain in survival in cases with p16-positive cells.
Conclusions
p16 positivity influences outcome only in young patients and OTs (p = 0.048).
Introduction
HPV positivity is a prognostic factor in squamous cell carcinoma (SCC) of the oropharynx (oropharynx tumors; OTs). However, the role of HPV infection in the upper aerodigestive tract outside the oropharynx is still unclear: some papers showed a positive correlation with outcomes while others did not (1). The limited number of cases in many reports hampers the interpretation of the available literature (2).
p16 is a tumor suppressor protein that acts by slowing the progression from G1 to S phase of the cell cycle. In HPV-related cancers, pRB, the target of p16, is downregulated and the feedback mechanisms regulating p16 expression are inhibited, resulting in overexpression of p16. Currently there is no standard for testing or interpreting HPV detection assays. Moreover, a strong correlation between p16 staining and HPV staining has been established in cancer cells of basaloid nonkeratinizing/partially keratinizing oropharyngeal carcinomas, while in conventional keratinizing squamous carcinoma of the oropharynx p16 staining requires additional HPV testing (3).
p16 positivity shows similar prognostic value to HPV positivity (4) and has been accepted worldwide as a surrogate marker of HPV infection (5). The reliability of p16 as a surrogate biomarker for HPV infection is based on the close correlation between p16 overexpression and HPV infection mainly in oropharyngeal cancers. p16 expression has been shown to have prognostic value even exclusive of HPV status (6-7-8-9).
Overexpression of EGFR, a known negative prognosticator, is less frequent in HPV/p16-positive tumors (4). p16 and EGFR are usually tested by immunohistochemistry (IHC). The advantage of IHC is that it is readily available in any pathology laboratory and relatively simple to evaluate. Unfortunately, IHC analysis is operator dependent and there is a lack of consensus as to what cutoff should be used for the determination of p16 positivity (10, 11). Many authors have chosen 70% of positive cells as the level of clinical relevance (10), but others have indicated lower levels, even as low as 10% (12-13-14). All the used levels showed a survival impact in the reported studies, but whether the extent of the benefit is equivalent is not known.
The correct identification of a cutoff value for p16-positive tumors will be of major importance in the near future, when a different treatment approach will possibly be offered to p16-positive patients. Similarly, understanding the role of p16 positivity outside the oropharynx could have practical consequences.
The aim of the present retrospective study is to verify the most clinically relevant cutoff for p16 and to compare the role of this protein in OT and non-OT primary tumors.
Materials and methods
We retrospectively collected a series of 270 patients with histologically confirmed locally advanced SCC of the head and neck, stage III-IV, treated with curative intent by chemotherapy and radiation therapy between 1997 and 2013 at the S. Croce University Hospital, Cuneo, Italy. Patients received alternating chemoradiation according to our clinical experience (15). In accordance with our internal standard procedures, patients were followed up taking into account the primary tumor site, performance status and response to treatment. Follow-up consisted of physical examination including vocal, breathing and swallowing assessment every 3-4 months for the first 2 years, then every 6 months until the fifth year, then ENT evaluation annually. Super-intensive follow-up was offered to patients still eligible for treatment with curative intent.
Patients with SCC of the maxillary sinus and undifferentiated carcinoma of the nasopharyngeal type (WHO types II and III), as well as patients for whom no adequate histological specimen was available or who were lost to follow-up were excluded. Eventually, specimens from 209 patients were analyzed (200 primary tumors and 9 involved lymph nodes).
IHC staining for p16 and EGFR and interpretation of histopathology were performed on 4-µm sections from formalin-fixed paraffin-embedded (FFPE) tissue blocks. Sections were mounted on glass slides using prediluted ready-to-use monoclonal antibodies: clone E6H4 (MTM Laboratories, Heidelberg, Germany) for p16 and clone 3C6 (Ventana Medical Systems, Inc., Tucson, AZ, USA) for EGFR, on a Ventana BenchMark ULTRA automated immunostainer according to standard protocol.
EGFR staining intensity was quantified according to FDA guidelines on a scale from negative to 3+. For p16, heat-induced antigen retrieval was performed at 95°C for 30 minutes in CC1 solution at pH 8. We evaluated both nuclear and cytoplasmic IHC staining. For positive and negative controls, sections of cervical intraepithelial neoplasia and normal spleen, respectively, were used in every session. Protein expression was evaluated in all cases by the same pathologist by counting the percentage of stained tumor cells over the whole tumor section.
The first analysis was the comparison between p16-positive and p16-negative tumors (considering as positive all tumors harboring at least 1% positive cells) in the whole population. We then compared the outcome of 4 groups: negative (0 positive cells), low positive (1%-9%), medium positive (10%-69%) and high positive (70%-100%) in both OTs and non-OTs. We subsequently considered 2 cutoffs, 10% and 70% positive cells, to define positive and negative tumors on the basis of the clinical literature.
Initially, the comparison between positive and negative tumors was performed separately in OTs and non-OTs to establish the prognostic significance of the tested cutoffs. We then compared the outcomes of OTs and non-OTs with similar p16 expression to define the prognostic role of p16 expression in and outside the oropharynx. We evaluated p16 as a prognosticator in young (<65 years old) and elderly patients.
An informed consent form approved by our ethics committee was routinely signed by all patients included in our database to use histopathological samples for scientific purposes.
Statistical Methods
We carried out the direct comparison between groups using the chi-square test, with Yates’ correction or Fisher's exact test when appropriate. All comparisons were 2-tailed. Survival curves were constructed according to the Kaplan-Meyer method, and differences between p16 status categories were estimated using the log-rank test. Overall survival (OS) was defined as the time from the start of treatment to death or last follow-up. We obtained life status and date of death of patients by registry. P values less than 0.05 were considered to indicate statistical significance.
Multivariate analysis was performed using Cox proportional hazards regression. The criteria for inclusion in multivariate analysis were clinical and statistical significance of the variables in the group analyzed. We therefore included the following clinical variables: age, EGFR, p16, lymph node status and tumor grading in the whole group (i.e., all patients, OT and non-OT). We excluded smoking because almost all patients (82%) were smokers. If the multivariate analysis did not obtain an overall p value <0.05, we excluded from the analysis the parameters with no statistical significance in univariate Kaplan-Meier analysis.
Statistical analysis was done with the Statistical Package for the Social Sciences (SPSS) v.13.
Results
We collected FFPE tissue samples from 209 patients with head and neck SCC. Patients were grouped into 2 cohorts: OT (63 patients) and non-OT (146 patients). Smoking history was known in 186 patients (90%), 93% of whom were heavy smokers (>10 packs/year). The patient characteristics are summarized in Table I.
Patient characteristics
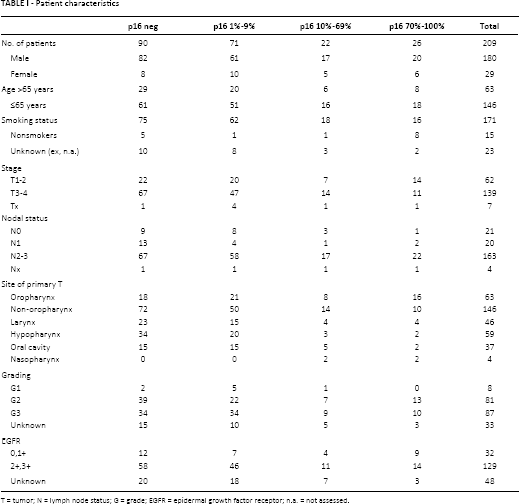
T = tumor; N = lymph node status; G = grade; EGFR = epidermal growth factor receptor; n.a. = not assessed.
Considering as positive all tumors showing at least 1% p16-positive cells, we observed 71% positive tumors among OTs and 50% among non-OTs (p = 0.0054). Taken together, a p16-positive status was associated with an OS advantage (36.8 months vs. 19.5 months, p = 0.02) (Fig. 1). We analyzed treatment response according to p16 status in OTs and non-OTs (Tab. II).
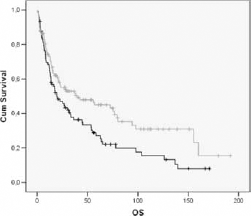
Overall survival in the whole patient population. X-axis: overall survival in months; Y-axis: population percentage. Patient groups: p16 positive (grey line), p16 negative (black line). Median survival time: 39.6 months (p16 positive), 19.5 months (p16 negative). Log-rank test for overall survival: p = 0.02.
Treatment responses in OT and non-OT patients
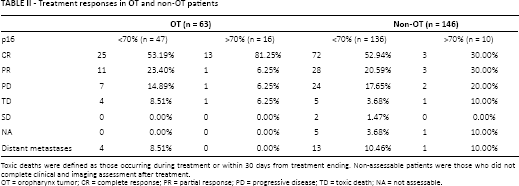
Toxic deaths were defined as those occurring during treatment or within 30 days from treatment ending. Non-assessable patients were those who did not complete clinical and imaging assessment after treatment.
OT = oropharynx tumor; CR = complete response; PR = partial response; PD = progressive disease; TD = toxic death; NA = not assessable.
Univariate Analysis
In the univariate analyses we considered stage variables (T1-2 vs. T3-4, N0, N1, N2-3), grade (1-2 vs. 3) and EGFR status (0-1 vs. 2-3) in OTs, non-OTs and the whole population. EGFR positivity correlated with outcomes in the whole population and in non-OTs (EGFR p = 0.02; EGFR p = 0.019, respectively). Grading was significant in primary OTs but not in non-OTs or in the whole population. No significant correlation was found for the other variables (T and N status) in OTs, non-OTs and the whole population.
Distribution of p16-Positive Cells
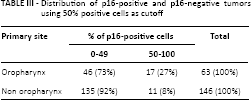
The cumulative distribution showed that the p16-positive values (from 1% to 100% positive cells) were located around 2 focus points at a median value of 2% (lower focus, median value of all positive values between 1% and 50%, range 1-45) and 96% (higher focus, median value of all positive values between 51% and 100%, range 55-99) (Fig. 2). No tumors showed positivity between 46% and 54%. The distribution of positive and negative tumors between OTs and non-OTs based on >50% or <50% is reported in Table III.
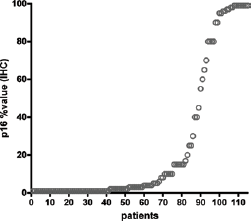
Cumulative distribution of patients on the basis of p16 IHC positivity. Positive cell values range from 1% to 100% and are concentrated around 2 focus points (2% and 96%). X-axis: overall survival in months; Y-axis: population percentage.
Distribution of p16-positive and p16-negative tumors using 50% positive cells as cutoff
Impact of Staining
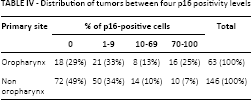
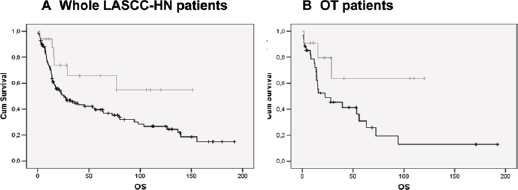
We analyzed the impact of p16 staining in the 4 groups mentioned above (negative, low positive, medium positive and high positive) and observed a different distribution in OTs and non-OTs (Tab. IV). We did not report any statistical difference in outcomes (p = 0.054 in OTs) (Fig. 3). Therefore we considered as positive tumors all those with 70% or more p16-positive cells; we observed a trend in OTs (median OS time 98 vs. 22 months in p16-positive and p16-negative OTs, respectively; p = 0.094) but not in non-OTs (median OS time 16 vs. 25 months in p16-positive and p16-negative tumors, respectively; p = 0.739) (Fig. 4A and 4B). This suggested that >70% of p16-positive cells was an appropriate cutoff.
Distribution of tumors between four p16 positivity levels
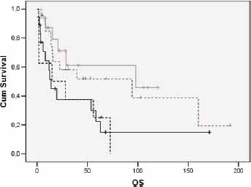
Overall survival in the group with oropharynx tumors. X-axis: overall survival in months; Y-axis: population percentage. Patient groups: p16 >70% positivity (grey line), p16 10%-70% positivity (black dotted line), p16 <10% positivity (grey dotted line), p16 negative (black line). Median survival time: 97.9 months (>70% positivity), 15 months (10%-70% positivity), 94.4 months (<10% positivity), 13.9 months (p16 negative). Log-rank test for overall survival: p = 0.054.
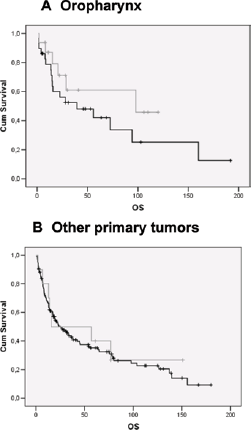
Overall survival in the OT and non-OT patient groups. X-axis: overall survival in months; Y-axis: population percentage. Patient groups: p16 >70% (grey line), p16 <70% (black line). (
Thus, we compared the outcomes of p16-positive tumors (>70% positive cells) in OTs versus non-OTs. The median OS times strongly diverged (98 vs. 16 months in OTs and non-Ots, respectively), but the difference did not reach statistical significance (p = 0.237).
Comparison of p16-negative tumors (<70% positive cells) between OTs and non-OTs showed a completely overlapping outcome (median OS 22 vs. 25 months, respectively; p = 0.916).
Impact of Age
We compared the outcomes of young (≤65 years) and elderly patients (>65 years) in p16-positive and negative tumors in the whole population (p = 0.047) (Fig. 5A). In young patients p16 positivity was associated with a significant gain in overall survival (p = 0.027) (Fig. 5B). No significant difference was observed in elderly patients. We performed the same analysis in the 2 subgroups: OTs and non-OTs. Similarly to the general population, p16 positivity influenced the outcome of young patients in the OT group (p = 0.048) but not that of elderly patients (p = 0.904). In non-OTs p16 status did not influence outcome either in young or elderly patients (p = 0.347 and p = 0.409, respectively).
(
Multivariate Analysis
We performed multivariate analyses separately in OTs, non-OTs and the whole population. The variables included in the model were EGFR (0, 1+ vs. 2+, 3+), p16 (cutoff 70% positive cells), N status (N0, N1 vs. N2, N3), tumor grade (1, 2 vs. 3) and age (cutoff 65 years). Cox regression analysis in OTs showed that both p16 and grading were independent variables correlated with favorable outcome. By contrast, in non-OTs both age and EGFR status correlated with outcome, but not p16 or grading.
In the whole patient population, only age correlated with outcome. The variables included or excluded in the multivariate model were chosen based on the strength of the statistically significant differences between them using the Kaplan-Meyer analysis (for example, age was excluded in the OT patient group analysis because of its lack of statistical significance) (Tab. V).
Multivariate analysis in (A) OT; (B) non-OT; (C) all patients’ population
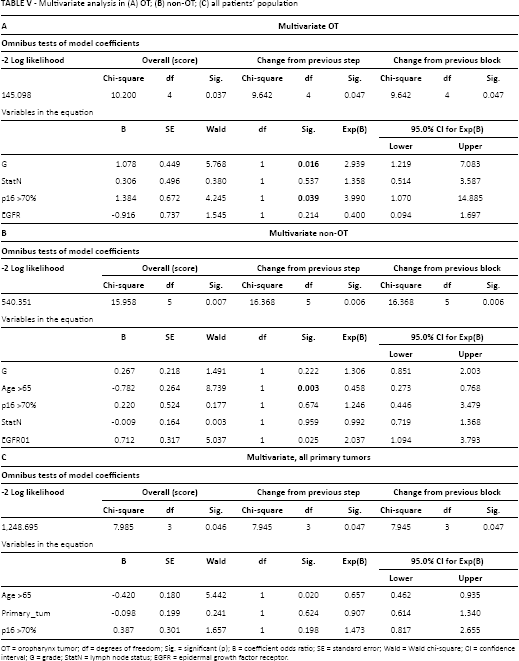
OT = oropharynx tumor; df = degrees of freedom; Sig. = significant (p); B = coefficient odds ratio; SE = standard error; Wald = Wald chi-square; CI = confidence interval; G = grade; StatN = lymph node status; EGFR = epidermal growth factor receptor.
Discussion
The goal of the present study was to identify a clinically relevant cutoff to define p16 positivity in head and neck SCC and to compare the role of p16 positivity in OTs and non-OTs. We intentionally limited the analysis to p16 because it is the test most employed in clinical practice.
Our results indicated that, in the present series and only in OTs, 70% of positive cells is a reliable cutoff to identify tumors with the best outcome. Overall, our data showed that in univariate analysis p16 positivity influenced the outcome of the whole series, but it lost its value in multivariate analysis. p16 significantly correlated with outcome in both univariate and multivariate analysis only in OTs and not in non-OTs.
In the subgroup analysis, the relationship between p16 positivity and outcome was present only in OTs while we did not observe any correlation in non-OTs. Dividing OTs into 4 groups based on the staining percentages (0, 1%-9%, 10%-69%, 70%-100% of positive cells), we surprisingly failed to observe a direct linear correlation between staining and outcome. Indeed, tumors with medium-positive values (10%-69%) had a worse outcome than tumors with low values (1%-9%). There were more elderly patients in the medium-positive group and the number of cases was small, but we have no clear explanation for this observation. It is noteworthy that most cases in this group showed less than 50% staining.
Mills et al (16) suggested that tumors with less than 50% p16 reactivity should be interpreted as equivocal. In light of this observation, the shift in outcome between patients with low values and medium values may be explained.
The analysis by age was also interesting. The prognostic value of p16 in OTs was statistically significant in young patients, but advanced age seemed to nullify the effect of p16. This could be the result of longer exposure to other carcinogens (for example, smoking) in the elderly population. Indeed, most of our patients were heavy smokers. By contrast, there was no impact of age related to p16 in non-OTs, either in p16-positive or p16-negative tumors.
An additional interesting observation is the confluence of positive cases around 2 focal points at the extremes of the range: 2% and 96% of positive cells. Because of this particular distribution, a cutoff of 50% positive cells seems reasonable. Others have also suggested this value (10). Placing the cutoff at 50% did not change the median OS in p16-positive and p16-negative tumors with respect to the higher cutoff (70%) either in OTs or non-OTs. However, the difference between positive and negative tumors at least in OTs (p = 0.13 and p = 0.094 for a cutoff of 50% and 70%, respectively), as it is predictable if patients with a better outcome move to the group with a worse outcome. This observation is speculative and we cannot yet support the adoption of 50% positive cells as the cutoff in routine clinical practice.
If we look at OTs versus non-OTs, the effect of p16 positivity was unclear outside the oropharynx and we did not observe any substantial difference between p16 positivity and negativity in patients with non-OTs.
Noteworthy in our series was the observation that p16 positivity did not impact on the outcome of non-OTs, regardless of the cutoff chosen and the age of the patients. In addition, the outcome of OTs and non-OTs was very similar among p16-negative tumors, while we observed a strong difference between OTs and non-OTs among p16-positive tumors. The small number of p16-positive tumors in non-OTs may partially explain the lack of a correlation between p16 positivity and outcome. However, in the literature one of the explanations for the difference between OTs and non-OTs is the high discordance between p16 positivity and HPV positivity, as observed by Marklund et al (17) and Doxtader et al (18). This observation offers a biological basis in favor of the lack of a correlation between p16 positivity and outcome in non-OTs.
An additional interesting observation is the lack of prognostic significance of EGFR in OTs in univariate analysis. However, the multivariate analyses showed that a weakness of the present study is the lack of analysis by subsites. Indeed, we analyzed patients with non-OTs all together, but the results reported by others suggest a possibly different behavior of p16-positive tumors between subsites. For example, Bova et al (19) reported that patients with p16-positive tumors of the anterior tongue had a significantly better progression-free survival (p = 0.007) and OS (p = 0.02) than those with p16-negative tumors. Conversely, Duray et al found no difference between p16-positive and p16-negative tumors in laryngeal cancers (20). Therefore, the overall analysis of non-OTs in our study may be limited, but the small number of p16-positive tumors, regardless of the cutoff chosen, rules out the possibility of a convincing subgroup analysis.
In our study we have only considered positive staining of tumor cells. Some authors have suggested the use of the staining intensity in addition to the percentage of positive cells (11). Others have rejected this suggestion, stating that the distribution of p16 staining is more important than its intensity (10). We agree with the latter position, mainly because the intensity of positivity is largely operator dependent and may thus be associated with considerable intra- and interlaboratory variability.
In conclusion, our data support the use of the value of 70% of positive cells as the cutoff to identify p16-positive tumors. The present analysis suggests that the impact of p16 positivity on outcome in OTs is lost in elderly patients, at least in this group including mainly heavy smokers. We did not observe any indication in favor of a possible prognostic role of p16 outside the oropharynx.
Footnotes
Acknowledgment
We are grateful to Fondazione Veronesi that granted D. Vivenza and M. Monteverde in 2014 with Post-Doctoral Fellowship 12 months, supporting the progression of this work.
Financial support: None.
Conflict of interest: None.