
Abstract
Background
PD-1 and its ligand PD-L1 belong to the co-inhibition molecules, which can downregulate immune responses. The PD-L1 polymorphism and the level of soluble PD-L1 (sPD-L1) were investigated in non-small cell lung cancer (NSCLC).
Methods
A total of 288 NSCLC patients and 300 controls were enrolled. An A/C polymorphism at position 8923 in the PD-L1 gene was genotyped using the polymerase chain reaction-restriction fragment length polymorphism method.
Results
The prevalence of the 8923C allele was significantly higher in NSCLC patients than controls (10.2% versus 5.3%, p = 0.002, odds ratio 2.03, 95% confidence interval 1.30-3.17; data were adjusted for age and sex). NSCLC patients also showed increased plasma levels of sPD-L1 compared to controls (1.92 ng/mL versus 0.91 ng/mL, p<0.001). Furthermore, lung adenocarcinoma patients had higher sPD-L1 levels than patients with squamous cell carcinoma (p<0.01). However, no association was observed between the different genetic variants and plasma concentrations of sPD-L1.
Conclusions
The PD-L1 8923A/C polymorphism could be associated with increased susceptibility to NSCLC. Plasma levels of sPD-L1 are significantly increased in NSCLC patients, especially those with adenocarcinoma.
Keywords
Introduction
Lung cancer is a malignant cancer with high morbidity and mortality rates worldwide (1). The disease is caused by many genetic and environmental factors such as tobacco smoking, infectious agents and radiation. In the last 2 decades, there have been an increasing number of studies focusing on the hereditary component of this disease. However, the specific mechanism is still unclear. Genome-wide linkage scans and genome-wide association studies (GWAS) make great efforts to offer sufficient power to seek disease-causing genetic factors (2).
Programmed death ligand 1 (PD-L1) is the third member of the B7 superfamily (3). Accumulating evidence has suggested that PD-L1 is involved in the negative regulation of the immune response. PD-L1 is expressed in T and B cells, macrophages and dendritic cells (4). It is also expressed in NSCLC cells (5). PD-1/PD-L1 interaction can downregulate T-cell responses and is an important pathway by which cancer cells evade the host immune surveillance (6, 7). PD-L1 has 2 forms of expression, a membrane-bound form and a soluble form. These 2 forms also have been found in other members of the B7/CD28 family such as CTLA-4 (8), CD28 (9) and B7-H4 (10). Some studies have shown that the abnormal expression of soluble PD-L1 (sPD-L1) can affect immune responses, which may result in autoimmune diseases and tumors (11-13).
Several single nucleotide polymorphisms (SNPs) in the PD-L1 gene have been observed in the Asian population (http://snp.ims.u-tokyo.ac.jp/index.html), where the 8923A/C polymorphism has been widely reported. The SNP can be detected in the Chinese population and is associated with autoimmune Addison's disease (14), type 1 diabetes (12), ankylosing spondylitis (15) and large B-cell lymphoma (16). However, reports about the SNP in lung cancer are rare. In this study, we investigated whether there is a correlation between the PD-L1 8923A>C SNP and NSCLC. Moreover, we investigated the effect of this polymorphism on sPD-L1 expression.
Materials and Methods
Study population
Between January 2011 and December 2014, a total of 288 patients (190 men and 98 women) with NSCLC who registered at Shandong Cancer Hospital were recruited. All patients were newly diagnosed and diagnoses were confirmed by histopathological examination. Peripheral blood from patients was collected prior to systemic therapy. The median age of the patients was 42 years (range: 26-78). The control group was made up of 300 volunteers who visited the same hospital during the same period. We only allowed Han Chinese into the group to exclude possible effects of ethnicity. Randomly selected controls were matched to the cases by age (±5 years) and gender. Informed consent was obtained from each participant at the time of recruitment. The study was approved by the review board of Shandong Cancer Hospital. Peripheral blood was collected from each study participant.
Genotyping
Genomic DNA was extracted from peripheral blood leukocytes using the AxyPrep Blood Genomic DNA Miniprep Kit (Fastagen, Shanghai, China) according to the manufacturer's instructions. The primers to amplify a 553-bp PCR product for rs74589371 (position 8923) were 5’-AATGGCTTGTTGTCCAGAGATG-3’ and 5’-GTACCACATGGAGT- GGCTGC-3’. PCR products were digested with Eco91I (New England Biolabs, Ipswich, MA, USA) and separated on 3% polyacrylamide gels. The presence of the A allele allowed the digestion of the 553-bp amplicon into 2 products of 456 bp and 97 bp, and the C allele resulted in 326 bp, 130 bp and 97 bp. About 10% of the PCR products were examined by DNA sequencing to confirm the genotyping results. Results between polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) and DNA sequencing analysis were 100% concordant.
Assessment of sPD-L1 level
Levels of sPD-L1 were tested using an enzyme-linked immunosorbent assay (ELISA) kit (PDCD1LG1 ELISA kit, USCN Life Science, Wuhan, China) according to the manufacturer's instructions. Each sample was analyzed in duplicate. The intra- and interassay coefficients of variation were <9%.
Statistical analyses
The SPSS statistical software package version 19.0 was used for all statistical analyses. The genotype and allele frequencies of the PD-L1 polymorphism were compared using the chi-square test. Odds ratios (OR) and 95% confidence intervals (CI) were calculated to assess the relative risks. Demographic and clinical data between groups were compared by the chi-square test and Student's t-test. Plasma levels of sPD-L1 were compared by Student's t-test. P<0.05 was considered statistically significant.
Results
Clinical Characteristics of the Study Participants
The clinical characteristics of the participants are presented in Table I. No significant differences in age or gender were observed between cases and controls. However, there was a significantly higher percentage of smokers in the patient group compared with the control group (61.8% vs. 46.3%, p<0.001).
Characteristics of NSCLC patients and controls
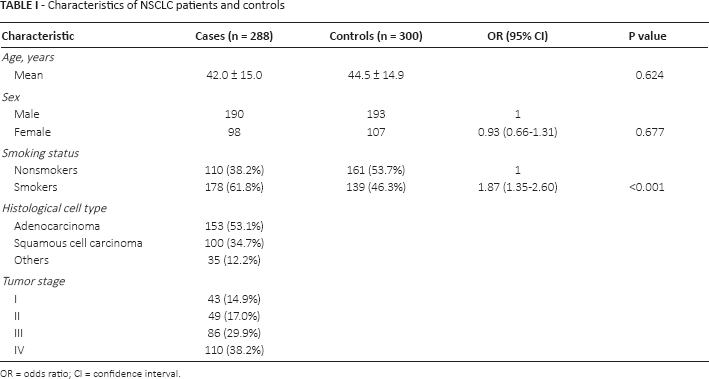
OR = odds ratio; CI = confidence interval.
Association between PD-L1 gene Polymorphism and NSCLC Susceptibility
The genotype and allele frequencies of the PD-L1 8923A>C polymorphism in NSCLC and control groups are summarized in Table II. The frequencies of AA, AC and CC genotypes were 80.9%, 17.7% and 1.4%, respectively, among NSCLC patients, and 89.7%, 10.0% and 0.3% among controls. The C-allele frequency was significantly higher in NSCLC patients than controls (10.2% vs. 5.3%, p = 0.002, OR = 2.03, 95% CI 1.30-3.17; data were adjusted for age and sex). In addition, we investigated the association between the PD-L1 gene polymorphism and smoking status in NSCLC patients. The results showed that the distribution of the SNP was similar between patients with different smoking status (data not shown).
Distribution of PD-L1 A>C polymorphism at position 8923 in NSCLC patients and healthy controls
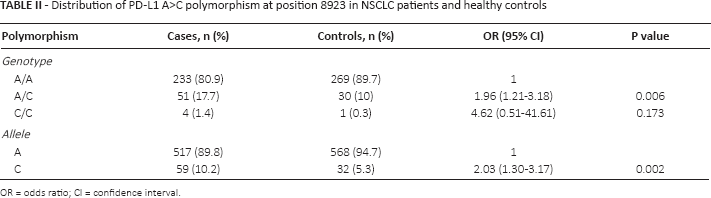
OR = odds ratio; CI = confidence interval.
Plasma level of sPD-L1 and NSCLC
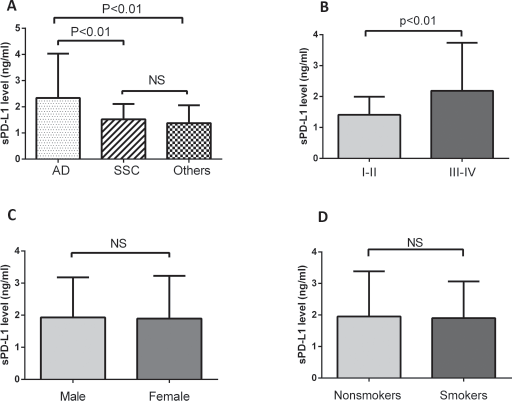
We investigated the plasma levels of sPD-L1 in NSCLC patients and controls, and found that patients had higher levels (1.92 ng/mL vs. 0.91 ng/mL, p<0.001) (Fig. 1). Furthermore, patients with adenocarcinoma had higher sPD-L1 levels than those with squamous cell carcinoma (p<0.01) (Fig. 2A). Similarly, patients with advanced clinical stages of disease (III-IV) had higher levels than those at early stages (I-II) (Fig. 2B), suggesting that sPD-L1 may be correlated with the progression of NSCLC. However, gender and smoking seemed not to affect the sPD-L1 level in NSCLC patients (Figs. 2C, 2D).
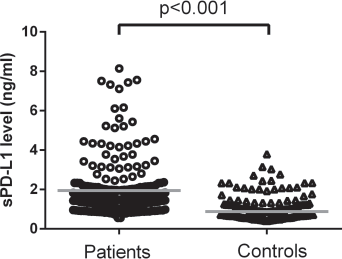
Plasma levels of sPD-L1 in NSCLC patients and controls.
(
Effect of PD-L1 gene polymorphism on sPD-L1 level
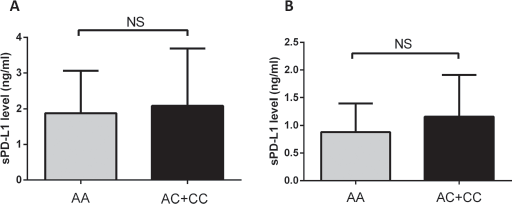
We further evaluated whether the PD-L1 gene polymorphism could affect sPD-L1 levels. The results revealed that the levels of sPD-L1 were similar between AA genotype and C allele carriers (Fig. 3).
(
Discussion
It has been reported that the PD-L1 8923A>C SNP is associated with different diseases. However, knowledge about the relation of this SNP to NSCLC remains limited. In this study, we found that the 8923C allele was associated with an increased risk of NSCLC in a Chinese population.
The PD-L1 gene has been mapped to chromosome 9p24 spanning 17.9 kb and including 7 exons. The gene is highly conserved. The A/C polymorphism at position 8923 in the PD-L1 gene occurs in intron 4. This locus has been reported to be associated with Graves’ disease (17) and lung cancer (18). Our results are consistent with the previous report (18). However, the function of the 8923 polymorphism is not clear. Hayashi et al (17) found that the polymorphism is near or within transcriptional factor binding sites, which may affect the processing and the binding affinity of transcriptional factors. Thus, the SNP may result in the production of a protein that lacks functional domains.
PD-L1 exists in humans in a membranous form and a soluble form that contributes to a precise immune regulation network (19, 20). Although no studies have confirmed that sPD-L1 is a direct inhibitory signal of PD-1-positive T cells, sPD-L1 can inhibit neighboring cells by participating in blood circulation and combining the surface receptors of distant cells, which may contribute to the occurrence and development of malignant diseases (21, 22). sPD-L1 has been found in a variety of diseases such as rheumatoid arthritis (11), renal cell carcinoma (23) and type 2 diabetes mellitus (24). Our data showed elevated levels of sPD-L1 in NSCLC patients, especially those with adenocarcinoma, suggesting that sPD-L1 secretion may have cell specificity (Fig. 1, Fig. 2A). In addition, we observed a positive association between sPD-L1 levels and stages of NSCLC (Fig. 2B), which suggests a potential effect of sPD-L1 on tumor progression.
We investigated whether the 8923A/C polymorphism could affect sPD-L1 expression. However, we did not observe any differences between subjects with different genotypes (Figs. 3A, 3B), which indicates that the SNP may not affect the promoter activity of the PD-L1 gene. Further experiments are needed to explore whether this polymorphism could affect the expression of membranous PD-L1.
There are some limitations to our study. First of all, only 1 SNP was investigated, which may produce marginal effects. In addition, since an SNP study or GWAS is based on the common disease-common variant (CD-CV) hypothesis, it may generate a lot of potential bias. By examining 288 NSCLC patients and 300 controls, we found that the prevalence of the 8923C allele was significantly increased in NSCLC patients. However, it might be premature to conclude there is an association between the 8923A/C SNP and the risk of NSCLC. Further studies with a larger sample size and different study population would be necessary. Also, it would be interesting to conduct prospective studies to confirm these findings.
In summary, our results suggest that the PD-L1 8923A/C polymorphism may be associated with an increased risk of NSCLC. Furthermore, an elevated plasma level of sPD-L1 was observed in NSCLC patients. This research sheds some light on the pathogenesis of NSCLC.
Footnotes
Financial support: None.
Conflict of interest: The authors declare no competing interests.