
Abstract
Background
Cripto-1 (CR-1) plays an important role in angiogenesis related to tumor growth, in concert with vascular endothelial growth factor (VEGF), and enhanced expression of CR-1 has been reported in lung cancer tissue.
Methods
Patients with lung cancer (n = 156) and healthy volunteers (n = 60) were enrolled in the study. Serum CR-1 and VEGF concentrations were measured using enzyme-linked immunosorbent assay.
Results
Patients with lung cancer had higher serum CR-1 (4.03 ± 1.49 ng/mL vs. 1.13 ± 0.43 ng/mL, p<0.05) and VEGF (503.62 ± 112.74 pg/mL vs. 398.62 ± 117.84 pg/mL, p<0.05) levels than the control group. With stage progression in non-small cell lung cancer (NSCLC), serum CR-1 levels increased, and patients with distant metastasis had higher levels than those without metastasis (p<0.05). In NSCLC, the low CR-1 group (<1.54 ng/mL) had a better overall survival rate compared with the high CR-1 group (>1.54 ng/mL, p<0.05).
Conclusions
Our study suggests that serum CR-1 is a useful diagnostic and prognostic marker for NSCLC patients.
Introduction
Lung cancer is the leading cause of cancer-related death worldwide (1). Although advances in noninvasive methods have improved our ability to detect lung cancer, more than 75% of lung cancer patients present at an advanced stage of disease, so that patients have little prospect of effective and curative treatment, with a 5-year survival rate of only 15% (2). The poor prognosis is due largely to lack of sufficient screening and early diagnostic tools for physicians.
Tumor markers play a key role in patient management for many malignancies. The potential uses of serum tumor markers include aiding early diagnosis and determining prognosis. Tumor markers that are currently available for lung cancer, such as carcinoembryonic antigen (CEA), cytokeratin 19 fragment (CYFRA21-1) and neuron-specific enolase (NSE), are not satisfactory for diagnosis at an early stage or for monitoring the disease because of their relatively low sensitivity and specificity in detecting the presence of cancer cells (3-6). Therefore, more studies are required to discover novel biomarkers to diagnose early lung cancer.
Cripto-1 (CR-1) is a member of the epidermal growth factor-cripto FRL1 cryptic (EGF-CFC) family (7, 8). CR-1 is overexpressed in breast, colon, lung, stomach, pancreatic and ovarian cancers (9). Furthermore, CR-1 expression is significantly increased in premalignant lesions, such as colon adenomas, intestinal metaplasia of the gastric mucosa and ductal carcinoma in situ of the breast (10). Recently, it has been reported that plasma CR-1 might be a novel biomarker for the early detection of breast and colon carcinomas (11). CR-1 is overexpressed in lung cancer tissues, and the levels of CR-1 expression are associated with the prognosis (12, 13), but serum levels of CR-1 have not been evaluated in lung cancer. We measured the serum levels of CR-1 in lung cancer patients and assessed their clinical significance.
Patients and Methods
Patients
Our study enrolled 156 lung cancer patients, including 120 with non-small cell lung cancer (NSCLC) and 36 with small cell lung cancer (SCLC), from December 2009 through November 2012. As control subjects, 60 sex- and age-matched healthy volunteers were enrolled in the same period. Baseline demographic data are presented in Table I. Histological type was determined according to the classification by the World Health Organization. Lung cancer staging was performed for all of the patients according to the Union for International Cancer Control (UICC-7) staging system (14). Overall survival (OS) was defined as the time interval between the date of diagnosis to the date of death or last contact. The median follow-up of surviving patients at the time of analysis was 24 months (range 3-42 months). The date of the last follow-up was 20 February 2014.
Demographic and clinical characteristics of lung cancer patients and controls
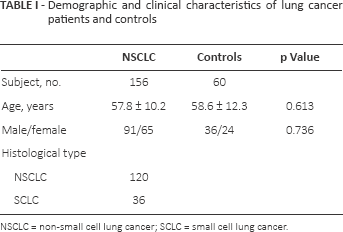
NSCLC = non-small cell lung cancer; SCLC = small cell lung cancer.
This study was approved by the Ethics Committee of Nanjing Chest Hospital, and informed consent was obtained from each patient.
Sample Collection and Determination of CR-1 and VEGF Concentrations
Serum samples were obtained from patients before treatment, at the time of diagnosis and on operation. Samples were centrifuged at 1,500 g for 10 minutes at −4°C. The supernatant was stored at −80°C for assessment of the concentrations of CR-1 and vascular endothelial growth factor (VEGF). An enzyme-linked immunosorbent assay was used to measure CR-1 and VEGF (Quantikine; R&D Systems, Minneapolis, MN, USA). All assays were run in duplicate, with dilutions as appropriate, and the technicians were blinded to clinical data.
Statistical Analysis
Statistical software (SPSS for Windows, version 18) was used for the analysis. The Mann-Whitney U test was used to compare patients and control groups, and the Kruskal-Wallis test was used to compare several groups. Spearman correlation of rank coefficient was used to analyze correlations between parameters. The cutoff value of the serum concentrations of parameters was calculated using a receiver operating characteristic (ROC) curve. Univariate survival analysis was performed using the Kaplan-Meier method and the log-rank test. Multivariate analysis was conducted to determine an independent impact on survival using the Cox proportional hazard method. Values of p<0.05 were considered statistically significant.
Results
Serum CR-1 and VEGF in lung cancer patients and control subjects
Patients with lung cancer had higher serum CR-1 levels than the control group (4.03 ± 1.49 ng/mL vs. 1.13 ± 0.43 ng/mL, p<0.05; Fig. 1A). Serum VEGF levels were also higher in patients with lung cancer than in the control group (503.62 ± 112.74 pg/mL vs. 398.62 ± 117.84 pg/mL, p<0.05; Fig. 1B).
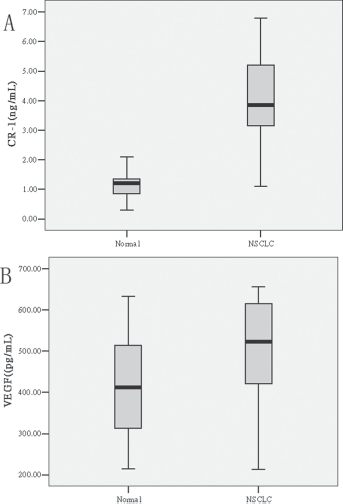
Serum cripto-1 (CR-1)
In all patients with lung cancer, serum CR-1 was significantly correlated with VEGF (Spearman r = 0.356, p<0.01; Fig. 2).
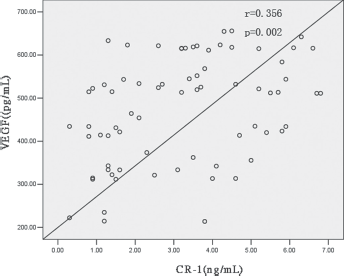
Correlation between serum cripto-1 (CR-1) and vascular endothelial growth factor (VEGF) levels in patients with lung cancer. In all patients with lung cancer, serum CR-1 was significantly correlated with VEGF (p<0.01).
Comparison of serum CR-1 and VEGF depending on stage progression in patients with NSCLC
Serum CR-1 and VEGF were compared according to stage progression in 120 patients with NSCLC. With stage progression, serum CR-1 levels increased and were significantly higher in stage IV than in stages I-III (p<0.05). Similarly, serum VEGF levels increased with the stage, although serum VEGF levels in NSCLC patients with stage IV tended to be higher than in those with earlier stages (p = 0.050, Tab. II).
Comparison of serum CR-1 depending on tumor progression in NSCLC
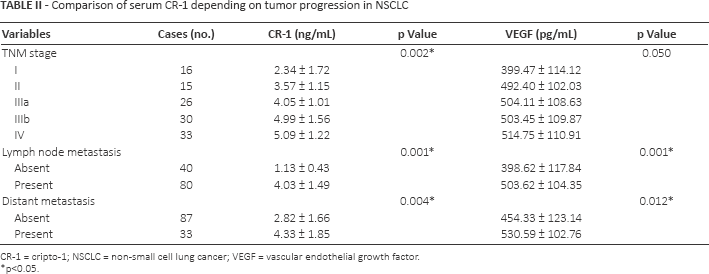
CR-1 = cripto-1; NSCLC = non-small cell lung cancer; VEGF = vascular endothelial growth factor.
p<0.05.
In the subgroup analysis, serum CR-1 levels were higher in stage I than in controls (p<0.05), whereas serum VEGF levels in stage I were not significantly different from those in controls. The levels of CR-1 and VEGF were significantly correlated with lymph node metastases (p<0.05), and distant metastases (p<0.05).
ROC analysis of serum CR-1 and VEGF
ROC curves for serum CR-1 and VEGF concentrations were constructed to determine cutoff values. The sensitivity and specificity of serum CR-1 levels in lung cancer patients relative to the control group were 80.8% and 56.7%, respectively, at a cutoff value of 1.54 ng/mL. The sensitivity and specificity of serum VEGF levels in lung cancer patients relative to the control group were 44.9% and 90.0%, respectively, at a cutoff value of 454.37 pg/mL. The area under the curve for serum CR-1 (0.794) was greater than for VEGF (0.643) (Fig. 3).
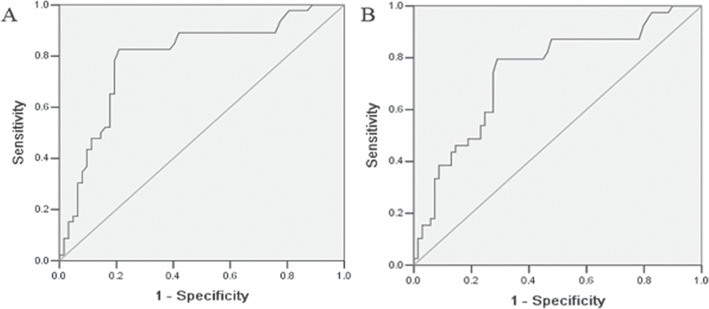
ROC curves for the serum cripto-1 (CR-1)
Association of serum CR-1 and VEGF levels with survival
Serum CR-1 and VEGF levels were dichotomized using median values for the survival analysis. The mean follow-up period was 21.6 ± 3.7 months in all lung cancer patients. In NSCLC patients, the low serum CR-1 group (<1.54 ng/mL) survived longer than the high serum CR-1 group (≥1.54 pg/mL; p<0.05; Fig. 4A). There was a significant difference in the survival was noted between the low serum VEGF group (<454.37 pg/mL) and high serum VEGF group (≥ 454.37 pg/mL; p<0.05; Fig. 4B).
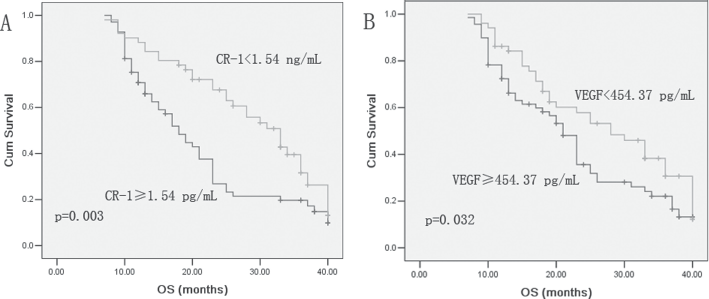
Kaplan-Meier survival analysis of non-small cell lung cancer (NSCLC) patients according to serum cripto-1 (CR-1)
Cox multivariate analysis was used to test the contribution of the serum CR-1 levels, tumor stage, age, sex and distant metastases on patient survival. Serum CR-1 levels were independent prognostic factors for OS in patients with NSCLC (Tab. III).
Multivariate Cox proportional hazards analysis for survival in NSCLC
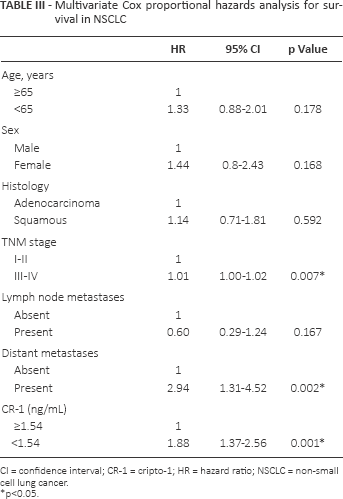
CI = confidence interval; CR-1 = cripto-1; HR = hazard ratio; NSCLC = non-small cell lung cancer.
p<0.05.
In the SCLC patients, the low serum CR-1 group (<1.54 pg/mL) survived longer than the high serum CR-1 group (≥1.54 pg/mL, p<0.05). However, no significant difference in the survival time was noted between the low serum VEGF group (<454.37 pg/mL) and the high VEGF group (≥454.37 pg/mL, p>0.05).
Discussion
CR-1 plays an important role in tumorigenesis by promoting cell proliferation, survival, migration and invasion and tumor angiogenesis (15). Of the many proangiogenic factors, VEGF is one of the most important. It is overexpressed in lung cancer tissue and related to prognosis (16, 17). Serum VEGF levels have been evaluated in lung cancer patients and with few exceptions were associated with tumor progression and prognosis (18-20).
CR-1 is highly expressed in lung cancer tissue. However, few studies have examined the clinical implications of serum CR-1 levels in lung cancer. Our measurements suggested that CR-1 was superior to VEGF for differentiating lung cancer from controls, and especially at distinguishing lung cancer patients with distant metastasis from those without. An increase in serum CR-1 in NSCLC depending on clinical stage and the significant elevation in patients with distant metastasis is theoretically plausible given that angiogenesis is essential to tumor progression, and CR-1 is mainly expressed in the tumor cells of lung cancer tissue.
In the present study, serum VEGF was significantly related to the stage of NSCLC, and it was correlated with serum CR-1 level. Serum VEGF levels in lung cancer have been shown to be related to stage progression in some studies but not consistently (18, 19, 21). Laack et al reported a significant relationship between serum VEGF and stage (22). Their results could be considered similar to our data.
Several previous studies have shown an association between CR-1 expression and cancer prognosis (9, 23). Xu et al indicated that there is a significant correlation between increased CR-1 mRNA expression levels and poor prognosis in lung cancer (13). This study supports the increasing body of literature demonstrating the expression of CR-1 in the prognosis of human cancers. The most striking association we observed in NSCLC patients was a significant correlation between increased serum CR-1 level and unfavorable prognosis.
In conclusion, increased serum CR-1 levels were significantly associated with poor prognosis. The present study provides evidence that serum CR-1 levels can be considered diagnostic and prognostic markers in NSCLC. More large-scale prospective studies are warranted to confirm the findings.
Footnotes
Financial support: This work was supported in part by a grant from the Twelve-Five Plan, which is the major program of the Nanjing Medical Science and Technique Development Foundation (Molecular Mechanism Study on Metastasis and Clinical Efficacy Prediction of Non-small Cell Lung Cancer) (to L.K.-Y.). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of interest: The authors declare that they have no competing interests.