
Abstract
Objectives
A relationship exists between sirtuin-1 expression and growth and survival of malignant tumors. This study aimed to investigate the prognostic value of sirtuin-1 and vascular endothelial growth factor (VEGF) expression in patients with liposarcoma by examining associations between their expression levels and clinical outcomes.
Methods
Clinical and histopathological characteristics and follow-up and survival information were retrospectively reviewed for 42 liposarcoma cases. Sirtuin-1 and VEGF protein expression levels were evaluated by immunohistochemistry and their associations with clinical parameters were analyzed using the Spearman-rho test. Univariate and multivariate Cox regression analyses were performed to identify potential prognostic factors. Kaplan–Meier analysis was performed to analyze overall survival.
Results
Sirtuin-1 and VEGF protein expression levels were significantly associated with histological grade, metastasis, and American Joint Committee on Cancer stage. A significant positive correlation was observed between sirtuin-1 and VEGF expression levels (R = 0.677). In univariate analysis, sirtuin-1 and VEGF expression were correlated with shorter overall survival, but the association was significant only for sirtuin-1 (hazard ratio = 3.752, 95% confidence interval 1.553–9.062) in multivariate analysis.
Conclusion
Sirtuin-1 and VEGF expression levels are significantly correlated with progression of liposarcoma, and sirtuin-1 expression significantly predicts a poor prognosis in patients with liposarcoma.
Introduction
Liposarcoma is a locally malignant mesenchymal tumor and the most common soft tissue sarcoma. 1 The biological behavior of liposarcoma is highly aggressive, and patients with liposarcoma are susceptible to local tissue invasion and distant metastasis. Accordingly, liposarcoma is associated with a high mortality rate. Despite major advances in chemotherapy in recent decades, no effective chemotherapy regimen has been determined for liposarcoma. Therefore, for patients with late-stage or recurrent liposarcoma, there are few options other than surgery. 2 Because the clinical prognosis of liposarcoma remains poor, further research aimed at developing effective therapeutic strategies is urgently required.
Chemotaxis is an important regulatory process in a variety of biological processes, such as stem cell homing, hematopoiesis, extracellular matrix remodeling, and cell-mediated wound healing.3,4 Previous research has consistently demonstrated a close relationship between tumorigenesis and chemokine expression. 5 Therefore, such cytokines are candidates as therapeutic targets to prevent progression of tumors. Additionally, studies examining the value of cytokines as markers for predicting responsiveness to treatment and tumor progression are important.
The sirtuins, which include SIRT1–7, are NAD+-dependent deacetylase enzymes that are found in mammals. Sirtuins are located in various cellular compartments and participate in many catalytic activities. 6 The most well-characterized sirtuin, SIRT1 (silent mating type information regulation 2 homolog 1), is a type III histone deacetylase. SIRT1 expression increases chemoresistance and is associated with progression of cancers and poor prognosis of patients with cancer.7,8 SIRT1 might contribute to chromatin remodeling, which promotes cancer progression. 9 Moreover, SIRT1 overexpression has been observed in breast, prostate, gastric, and ovarian cancers, as well as in lymphoma.10–13
Another essential process for tumor growth is angiogenesis. Vascular endothelial growth factor (VEGF) is a highly specific vascular endothelial cell mitogen that may participate in carcinogenesis by inducing angiogenesis and increasing microvascular permeability.14,15
Because of the potential roles of SIRT1 and VEGF in progression of cancer, we hypothesized that SIRT1 and VEGF expression has prognostic value in patients with liposarcoma. To test this hypothesis, we examined the expression patterns of SIRT1 and VEGF in patient-derived liposarcoma tissue samples and studied the associations of SIRT1 and VEGF expression with clinical outcomes.
Patients and methods
Patients
The present study evaluated paraffin-embedded liposarcoma specimens that were collected from patients who visited the Fourth Hospital of Hebei Medical University between 2004 and 2012. The clinical and histopathological characteristics, as well as follow-up and survival information, were available for all patients, and were collected retrospectively from medical records. Radiotherapy and chemotherapy were not administered before surgery in any case. Patients’ data were grouped according to the age, sex, tumor size ( < 5 cm and ≥5 cm), histological grade according to the Fédération Nationale des Centres de Lutte Contre Le Cancer (FNCLCC), the presence of distant metastasis, and American Joint Committee on Cancer (AJCC) staging. This study complied with the Declaration of Helsinki and was approved by the Human Ethics and Research Ethics Committees of the Fourth Hospital of Hebei Medical University. Written informed consent was obtained from all patients.
Immunohistochemistry
For immunohistochemical analysis, a tissue microarray was produced using 4.0-mm diameter tumor core samples with one core per case. Antigen retrieval was performed by microwaving the array in sodium citrate buffer for 10 minutes. Immunohistochemical staining was carried out using a previously described protocol. 16 Primary antibodies included mouse anti-human rabbit anti-human SIRT1 antibody (1:50, clone H-300; Santa Cruz Biotechnology, Santa Cruz, CA, USA) and goat anti-human VEGF (1:100; Santa Cruz Biotechnology). Immunohistochemically stained sections were analyzed under an optical microscope by three pathologists who were blinded to all patients’ data. The mean number of positively stained cells was determined in five fields-of-view at 400× magnification. Evaluation of immunohistochemical staining was performed according to Friedrich’s immune reactivity score 17 and graded as follows: (1) 0 points if < 1% of cells were stained; 1 point if 1% to 25% of cells were stained; 2 points if 25% to 50% of cells were stained; 3 points if 51% to 80% of cells were stained; and 4 points if >80% of cells were stained. Staining intensity was graded according to the degree of staining color depth as follows: 0 points if there was no staining; 1 point for buff staining; 2 points for darker buff staining; and 3 points for tan staining. The final immunohistochemical scores were calculated as the product of the staining percentage score and the staining intensity score, and staining was described as low (0–3 points, −/+), moderate (4–7 points, ++), or high (>7 points, +++).
Western blot analysis
Protein in each sample was separated by sodium dodecyl sulfate-polyacrylamide gel electrophoresis (10%) and transferred to a polyvinylidene fluoride membrane (Millipore, Billerica, MA, USA). The membranes were blocked by 5% non-fat-milk and then incubated with primary antibodies against SIRT1 (1:100, Santa Cruz Biotechnology) and VEGF (1:200, Santa Cruz Biotechnology) at 4°C overnight. After washing, the membranes were incubated with the corresponding horseradish peroxidase-conjugated secondary antibodies for 1.5 hours at room temperature. The signals were finally detected using Clarity Western ECL Substrate (Bio-Rad, Hercules, CA, USA). Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was used as the internal control for normalization of expression levels.
Statistical analysis
The end of follow-up was defined as the date of death or last contact through June 2019. Overall survival was defined as the time from the date of diagnosis to the date of last contact or death. Associations of potential prognostic factors were analyzed using the χ2 test. For correlation analysis, the Spearman-rho test was used to compare histological and clinical variables. Univariate and multivariate analyses were conducted using Cox proportional hazards regression analysis. Survival curves were plotted by the Kaplan–Meier method. All statistical analyses were conducted using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). In all analyses, statistical significance was set at a p value < 0.05.
Results
Associations of SIRT1 and VEGF protein expression levels with clinicopathological characteristics
The clinical characteristics of the 42 patients included in this study are shown in Table 1, along with the expression patterns of SIRT1 and VEGF in these patients. The mean age was 40.6 ± 16.1 years (range, 6–64 years), and the median overall survival was 41 months (range, 7–89 months). Representative images of SIRT1 and VEGF staining and expression in liposarcoma tissues are shown in Figure 1A and 1B, respectively. In liposarcoma tissues, staining for SIRT1 and VEGF was primarily nuclear, but the staining scores showed variation from low to high among the cases. Specifically, SIRT1 expression was low in 21.4% (9/42) of cases, moderate in 31.0% (13/42), and high in 47.6% (20/42), whereas VEGF expression was low in 21.4% (9/42), moderate in 35.7% (15/42), and high in 42.9% (18/42). SIRT1 and VEGF protein expression levels were significantly associated with histological grade (p = 0.005), distant metastasis (p = 0.005), and AJCC staging (p < 0.001). However, no significant associations were observed between the expression levels of these proteins and the other clinicopathological features included in the analysis. Notably, a significant positive correlation was found between SIRT1 and VEGF expression (R = 0.677, p < 0.001; Table 2).
Clinicopathological variables and SIRT1 and VEGF protein expression in patients with liposarcoma.

The Spearman-rho test was used for analysis. SIRT1: sirtuin-1; VEGF: vascular endothelial factor; AJCC: American Joint Committee on Cancer. *p < 0.05.

(A) Representative immunohistochemical staining of SIRT1 and VEGF. (a) Low expression of SIRT1 in liposarcoma, (b) moderate expression of SIRT1 in liposarcoma, (c) high expression of SIRT1 in liposarcoma, (d) low expression of VEGF in liposarcoma, (e) moderate expression of VEGF in liposarcoma, and (f) high expression of VEGF in liposarcoma. The cells with positive expression show brown staining. (B) Quantitative western blot verification of the expression patterns observed by immunohistochemistry. SIRT1: sirtuin-1; VEGF: vascular endothelial factor; GAPDH: glyceraldehyde-3-phosphate dehydrogenase.
Correlation of SIRT1 and VEGF protein expression.

The Spearman-rho test was used for analysis. SIRT1: sirtuin-1; VEGF: vascular endothelial factor.
High SIRT1 and VEGF protein expression correlates with poor overall survival of patients with liposarcoma
The results of univariate Cox proportional hazard analysis for overall survival are shown in Table 3. Sex, age, and tumor size were not significant predictors of overall survival. However, the presence of distant metastasis (p < 0.001), higher histological grade (p = 0.029), and higher AJCC stage (p < 0.001) were predictive of shorter overall survival (Table 3, Figure 2). Additionally, univariate analysis showed that increased SIRT1 (p < 0.001) and VEGF (p = 0.001) protein expression levels based on higher staining scores were significantly associated with shorter overall survival (Table 3, Figure 2).
Clinicopathological factors associated with liposarcoma by univariate Cox proportional regression analysis.

OS: overall survival; HR: hazard ratio; 95% CI: 95% confidence interval; SIRT1: sirtuin-1; VEGF: vascular endothelial factor; AJCC: American Joint Committee on Cancer. *p<0.05.
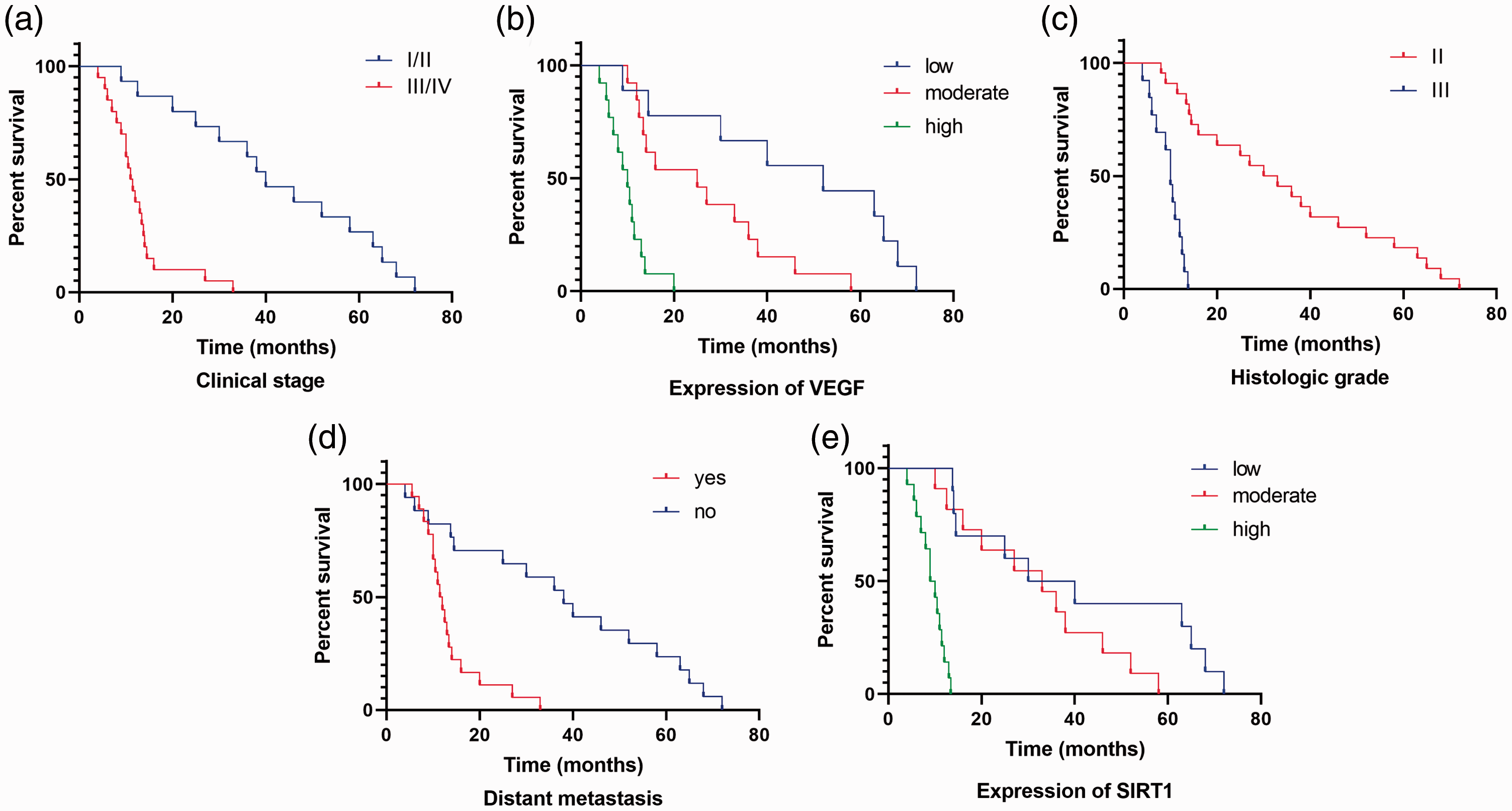
Overall survival curves of patients with liposarcoma. (a) Associations of overall survival with clinical stage, (b) VEGF expression, (c) H3K27me3 expression, (d) distant metastasis, and (e) SIRT1 expression. p values were determined by comparing survival distributions using the log-rank test. SIRT1: sirtuin-1; VEGF: vascular endothelial factor.
High SIRT1 protein expression predicts poor survival of patients with liposarcoma
The results of multivariate Cox proportional hazard analyses of univariate factors associated with overall survival are shown in Table 4. In multivariate analysis, only distant metastasis, AJCC stage, and SIRT1 expression were significant independent prognostic factors for overall survival in patients with liposarcoma (all p < 0.05). Therefore, patients with liposarcoma and distant metastasis, a higher AJCC stage, and higher SIRT1 expression had a significantly greater risk of mortality (p log-rank: 0.003; Figure 2). These findings suggest that SIRT1 expression is a significant potential clinical prognostic factor for patients with liposarcoma.
Clinicopathological factors associated with liposarcoma by multivariate Cox regression analysis.

OS: overall survival; HR: hazard ratio; 95% CI: 95% confidence interval. AJCC: American Joint Committee on Cancer; SIRT1: sirtuin-1. *p < 0.05.
Discussion
In the present study, we examined the expression patterns and prognostic significance of SIRT1 and VEGF in liposarcoma. To the best of our knowledge, this is the first study to show increased SIRT1 and VEGF protein expression levels in liposarcoma tissues. Additionally, high SIRT1 and VEGF protein expression levels were significantly associated with unfavorable clinical variables, including distant metastasis and a more advanced AJCC stage. A positive correlation was observed between SIRT1 and VEGF expression, and high levels of both proteins were positively correlated with advanced clinical features, such as a high clinical stage, high histological grade, and distant metastasis. Although high protein expression levels of both SIRT1 and VEGF were significantly associated with shorter overall survival in patients with liposarcoma in univariate analysis, only SIRT1 expression levels were an independent prognostic indicator of overall survival in multivariate analysis. Overall, our study indicated that SIRT1 and VEGF protein expression in liposarcoma tissues may be used to assess progression of liposarcoma and to predict the prognosis of patients with liposarcoma.
SIRT1 is a histone deacetylase with critical roles in a variety of processes associated with tumor formation, such as apoptosis, inflammation, genetic stability, autophagy, and the immune response.18,19 However, the mechanisms by which SIRT1 functions in these processes are complex. Recent studies have shown that the functional role of SIRT1 in tumor progression varies among different types of tumors. 20 However, overexpression of SIRT1 is consistently correlated with tumor cell survival through deacetylation and subsequent degradation of the p53 tumor suppressor. 21 Additionally, SIRT1 overexpression is a predictor of a poor prognosis in multiple tumor types, including soft tissue sarcomas.22,23 In angiosarcoma, SIRT1 overexpression is associated with invasive proliferation and malignant transformation. 23 A recent study showed associations between SIRT1 expression and metastasis and poor prognosis in osteosarcoma, and treatment with a SIRT1 inhibitor resulted in osteosarcoma cell death in vitro and prohibited tumor growth and spread in vivo. 24 In the present study, high SIRT1 expression was found in more than 40% of liposarcoma cases, which is consistent with the findings of previous studies. 22
VEGF is a mediator of angiogenesis that acts by increasing microvascular permeability. 25 Therefore, VEGF is upregulated in angiogenic disorders, such as atherosclerosis, hemangioma, liver and kidney disease, inflammatory diseases, and cancer. Accordingly, the expression level of VEGF is commonly used as a marker for detecting such disorders. In soft tissue tumors, VEGF is secreted by mesenchymal tumor cells and peritumoral mast cells for induction of angiogenesis. 26 Importantly, previous studies have reported that VEGF expression is significantly associated with survival of patients with various types of cancer.27–29 Univariate analysis in the present study showed an association between VEGF expression and overall survival of patients with liposarcoma. However, this association did not remain significant in multivariate analysis.
Tight regulation of SIRT1 and VEGF expression may play an important role in progression of cancer. Therefore, in addition to serving as a prognostic marker, SIRT1 represents a novel target for therapeutic intervention in patients with liposarcoma. SIRT1 and VEGF promote angiogenesis, although their exact roles in liposarcoma remain to be fully determined. Therefore, additional in vivo and in vitro investigations of the molecular mechanisms by which these proteins promote tumor progression are required.
The present study has several limitations. First, immunohistochemistry is a semi-quantitative analytical method. Therefore, some bias was possible in determination of staining scores. To minimize such bias, the samples were analyzed independently in a blinded fashion by three pathologists, and if disagreement occurred, a consensus was reached by discussion among the pathologists. Second, the sample size of 42 cases was relatively small. Therefore, our findings need to be confirmed in a larger population.
In summary, the majority of patients with liposarcoma in this study showed moderate or high protein expression of SIRT1 and VEGF. Additionally, high SIRT1 and VEGF protein expression levels were associated with unfavorable clinical characteristics and a poor prognosis among patients with liposarcoma. The mechanistic roles of SIRT1 and VEGF in tumorigenesis in liposarcoma require further investigation. However, our results indicate that SIRT1 expression may be useful in predicting the prognosis of patients with liposarcoma and serve as a potential therapeutic target for treatment of liposarcoma.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Key Project of Medical-Science Research of Hebei Province (No. 20180564) and the Project of the Natural Science Foundation of Hebei Province (No. H2019206309).
Supplemental Material
Supplemental material for this article is available online.