
Abstract
Colorectal cancer is one of the most common malignant cancers, with bad prognosis when distal metastasis occurs. The current study aimed to investigate the potential value of using CCX-CKR expression for the prognosis of colorectal cancer patients. The results showed that CCX-CKR expression was a negative predictor of cancer metastasis, and that it was positively correlated to the patients’ survival rate. Finally, we found that CCX-CKR expression in vitro could modulate cellular migration and invasion abilities, potentially via the regulation of other chemotactic factors/receptors.
Introduction
Colorectal cancer is one of the most common malignant cancers, and the fourth cause of cancer-related mortality (1). Distal metastases significantly contribute to the high mortality rate; the 5-year survival rate in patients with non-distal metastasis is 80%-90%, and is 10%-20% in patients with distal metastasis (2). Therefore, a better understanding of the molecular mechanisms underlying the formation of distal metastasis in colorectal cancer would provide important information for relevant therapies. Chemotactic factors and their receptors regulate tumor growth, angiogenesis, and cancer cell invasion during metastasis (3–5). CXCR4/CXCL12 (SDF-1) represents the best-studied chemotactic factor/receptor pair and is involved in metastasis of multiple malignant cancers including breast cancer, prostate cancer, ovarian cancer, and colorectal cancer (6–8). In addition, also CCR7/CCL19 (CCL21), CCR9/CCL25, and CXCR5/CXCL13 were shown to be involved in colorectal cancer metastasis (9–12).
The ChemoCentryx chemokine receptor (CCX-CKR) is the third atypical chemokine binder identified after Duffy antigen receptor for chemokine (DARC) and D6 (13–15). CCX-CKR can bind to and clear CCL19, CCL21, CCL25, and CXCL13 (16–18). It has been shown that CCX-CKR can inhibit angiogenesis in breast cancer (19), and its expression was found to be negatively correlated with lymph metastasis of invasive breast cancer (20). In addition, CCX-CKR is positively correlated with the total survival rate in gastric cancer patients (21). Yet the type of variations of CCX-CKR expression in colorectal cancer and whether CCX-CKR can be used as a predictive factor for survival analysis is still unknown.
The present study investigated the expression of CCX-CKR in colorectal cancer patients, as well as the relationship between the expression levels of CCX-CKR and the patient survival rates. We further examined the potential molecular mechanisms underlying CCX-CKR expression in colorectal cancer cells. The results showed that the upregulation of CCX-CKR expression was negatively correlated to lymph node metastasis, and positively correlated to the total survival rate of patients. Our in vitro experiments showed that CCX-CKR expression could inhibit the migration and invasion ability of colorectal cancer cells, potentially via the downregulation of CCR7, CCR9, CXCR5, and CXCR4.
Materials and Methods
Clinical data
A total of 136 colorectal cancer patients, who received surgical treatment in our hospital between Jan 2009 and Apr 2009, were retrospectively recruited for analysis. None of the patients received chemotherapy or radiological therapy prior to surgery (detailed clinical data are reported in Tab. I). Tumor tissues were fixed in 10% formalin immediately after surgical removal before being embedded in paraffin.
Patient and Tumor Characteristics

With regard to chemotherapy treatment, patients with severe phase II and III tumors were using FOLFOX (12 phases). Patients who could not tolerate FOLFOX were treated with 5-FU. Phase IV patients were first using FOLFOX (12 phases), and switched to FOLFIRI if with recurrence. Patients who could not tolerate FOLFIRI were treated with Irinotecan only, while patients with worse conditions were using 5-FU + DDP protocol.
Written informed consent was obtained from all patients and the study was approved by the clinical research ethic committee in Xinhua Hospital, at the Shanghai Jiaotong University. The end of the follow-up was set for April 28, 2012.
Cell culture
The human colorectal cancer cell line LoVo was purchased from the American Type Culture Center (MA, US) and maintained in F12-K cultured medium containing 10% FBS (Invitrogen, Shanghai, China). The cells were incubated at 37°C in a 5% CO2 incubator. HCT-116 and HT-29a cell lines were maintained in McCoy's 5a. SW620 was maintained in Leibovitz's L-15 medium. For subculturing, the LoVo cell line was diluted at 1:3, while the HCT-116, HT-29a, and SW620 cell lines at 1:4.
Immunohistochemistry
A total of 136 paired samples of colorectal cancer tissues and nearby normal tissues were prepared for CCX-CKR protein expression analysis as previously described (22). The goat polyclonal antibody CCX-CKR (ab1660, Abcam, UK, 1:250) was used for antigen detection. The staining results were analyzed by 2 independent investigators blind to the patient prognosis.
The staining results were reported with a semi-quantitative system as suggested by a study from Remmele and Stegner, who scored the images by calculating the percentage of staining multiplied for the staining intensity (23). The percentage of staining was scored as 0 (0%), 1 (0%-25%), 2 (25%-50%), 3 (51%-75%), and 4 (>75%). The staining intensity was scored as 0 (negative), 1 (weakly positive), 2 (moderately positive), and 3 (strongly positive). Stainings that scored less than 6 were considered as “low expression” and those that scored more than 6 were considered as “high expression”.
Plasmid construction and lentivirus package
The CCX-CKR cDNA was amplified (primers’ sequences, F: 5′-CACAGACCGGTATGGCTTTGGAACAGAACC-3′ R: 5′-CACAGGAATTCGCAGAGCAGTTTTACCTTT-3′) and cloned into the lentiviral vector pSin for expression. The viral vectors were transfected into human embryo kidney HEK293T cells for lentivirus vector generation with lipofectamine 2000 (Invitrogen, US). The supernatant of the culture medium containing viral particles was harvested 48 hours later, and 8 μg/mL polybrene (Sigma, US) were added for cell transfection.
RT-qPCR
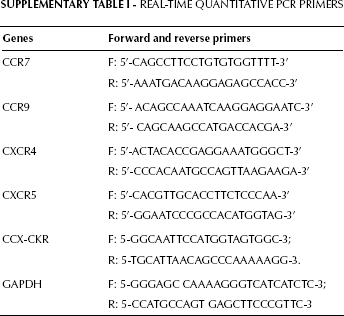
The total RNA was extracted with RNAiso Plus (TaKaRa, Japan) and cDNA was synthesized with the PrimeScript® RT-PCR Kit (TaKaRa, Japan). RT-qPCR was performed on ABI 7500 (ABI, US) with SYBR® Premix Ex Taq™ Kit (TaKaRa, Japan). The primers used are listed in the supplementary Table I.
Real-Time Quantitative PCR Primers
Western blot analysis
The cells were treated with Cell Lysis Buffer (CST #9803, US) and proteins were isolated on 10% SDS-PAGE gel before transfer onto the nitrocellulose membrane. Then the membrane was blocked with 3% BSA solution, before adding the anti-CCX-CKR (Abcam, 1:1000) or anti-GAPDH antibody (Santa Cruz, 1:1000). Finally, the staining was visualized with the HRP-secondary antibody and ECL kit.
Cell migration and invasion tests
Transwell chambers (Corning #3422) were used to analyze the cell migration and invasion abilities. For the migration assay, cells were resuspended in 1% FBS culture medium and added into the upper chamber (LoVo 8×104 cells/well); and 600 μL of 10% FBS culture medium were added to the lower chamber for 16 hours before adding 4% formaldehyde and Hoechst 33342 staining of the lower chamber membrane. The cells were counted under an epi-fluorescence microscope (Zeiss).
For the invasion assay, the upper chamber was embedded with 0.05 mL matrigel (BD Biosciences, 1:8) for 4 hours, and the culture lasted for 21 hours. The rest of the protocol followed the same steps as those for the cell migration assay.
Statistics
The data were analyzed with the SPSS 12.0 software (SPSS Lnc., Chicago, US). The chi-squared test was used to calculate the relationship between CCX-CKR expression and clinicopathological parameters. The overall survival (OS) and progression-free survival (PFS) were calculated from the first day post-surgery until death or first recurrence, and survival curves were estimated with the Kaplan–Meier method. The survival differences across groups were compared with the log-rank test. The Cox proportional-hazard model was used to determine independent prognostic factors for colorectal cancer. The Student's t test was used to compare the differences between experimental groups. A p value <0.05 was considered statistically significant.
Results
Immunohistochemical staining and RT-PCR examination of CCX-CKR
Immunohistochemical staining of CCX-CKR showed a strong soma staining as well as some membrane staining (Fig. 1). The rate of CCX-CKR protein positive expression in colorectal cancer tissues was of 66/136 (49%), while in normal colorectal tissue it was 98/136 (72%, p=0.022).

Immunohistochemical staining of CCX-CKR at different staining intensities.
Intrinsic expression levels of CCX-CKR in the LoVo and other colorectal cancer cell lines were investigated by RT-PCR (Fig. 2). The results suggested that the LoVo cell line exhibited moderate levels of CCX-CKR expression in comparison with other colorectal cancer cell lines. Therefore alterations in the CCX-CKR levels might be able to modify the cellular characteristics of the cell line.

Intrinsic expression levels of CCX-CKR in LoVo and other colorectal cancer cell lines detected by RT-PCR.
Correlations between CCX-CKR protein expression levels and clinicopathological parameters and prognosis in patients with CRC
Among the 136 colorectal cancer cases 70 (51%) showed a low CCX-CKR protein expression (staining <6), while 66 (49%) showed a high CCX-CKR expression. The downregulation of CCX-CKR expression was significantly correlated with lymph node metastasis of cancer cells, while the upregulation of CCX-CKR expression occurred in tissues with negative signs of metastasis (p=0.002) (Tab. II). The CCX-CKR-positive protein expression rate was 18/28 (64%), 23/39 (59%), 14/40 (35%), and 11/29 (38%), respectively for patients with stage I, II, III, and IV colorectal cancer.
Correlation of Ccx-Ckrexpression with Clinico-Pathological Parameters In Colorectal Cancer

Denotesa significant difference between stage I and stage III.
Denotesa significant difference between stage I and stage IV.
Denotesa significant difference between stage II and stage III.
Denotesa significant difference between stage II and stage IV.
In addition, the upregulation of CCX-CKR protein expression was significantly correlated with the TNM staging of the cancer tissue: in cancer tissues staged I and II the CCX-CKR expression levels were significantly higher than those staged III and IV (p=0.006) (Tab. II). Moreover, CCX-CKR expression was not correlated to age, gender, position of cancer, diameter/invasion and depth/distal metastasis of cancer. Finally, the Kaplan–Meier survival analysis revealed that high CCX-CKR protein levels correlated with longer patients’ survival (Fig. 3) (log rank p=0.04).

Kaplan–Meier survival analysis showing that high CCX-CKR expression suggested longer patients’ survival (OS and PFS).
CCX-CKR and patient survival prognosis
The follow-up was of 38 months in all the 136 patients. Within this period, a total of 32 patients died and 60 patients showed disease progression. The 3-year OS rate was 78% and the PFS rate was 56% (71% for stage I-III patients).
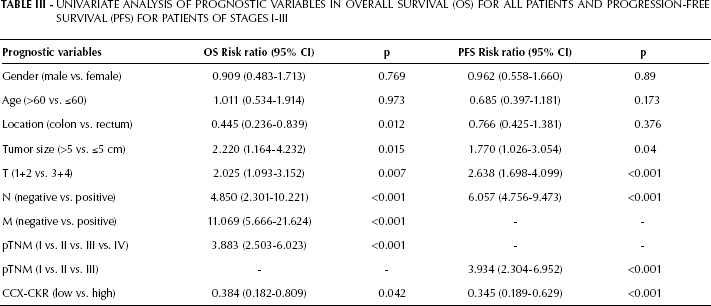
In univariate analysis (Cox's proportional-hazards regression model, Tab. III) CCX-CKR high expression showed significant correlations with OS and PFS. Other predictive factors relevant to OS included tumor location (p=0.012), tumor size (p=0.015), pT (p=0.007), lymph node status (p<0.001), metastasis status (p<0.001), and pTNM stage (p<0.001). All these factors except tumor location were also correlated to PFS (Tab. III).
Univariate Analysis Of Prognostic Variables In Overall Survival (Os) For All Patients And Progression-Free Survival (Pfs) For Patients Of Stages I-III
Multivariate analysis further showed that only metastasis status (RR=3.508, 95% CI: 1.538–6.764, p=0.015) was an independent predictor of OS, while lymph node status (RR=1.258, 95% CI: 0.668–2.323, p=0.016) and CCX-CKR expression levels (RR=0.365, 95% CI: 0.197–0.676, p<0.001) were independent predictors of PFS (Tab. IV).
Multivariate Analysis Of Prognostic Factors In Overall Survival (Os)For All Patients And Progression-Free Survival (Pfs) For Patients Of Stages I-III

CCX-CKR inhibits colorectal cancer cell migration/invasion
To further examine the effects of CCX-CKR on colorectal cancer cells, the protein was expressed with the lentiviral vector Fugw-CCX-CKR for overexpression in the LoVo cell line (Fig. 4A-B). In our transwell chamber assay, the overexpression of CCX-CKR reduced the cell migration and invasion abilities of, respectively, 42% and 30% compared the controls (Fig. 4C-D). Moreover, we found that CCX-CKR overexpression showed no effects on the cell growth and proliferation capabilities (data not shown).

Overexpression of CCX-CKR in colorectal cancer cells leading to decreased cell migration and invasion in transwell chamber assays.
CCX-CKR inhibits the expression of CCR7, CXCR5, and CXCR4
We examined the effects of CCX-CKR overexpression on CCR7, CXCR5, and CXCR4 levels to elucidate potential signaling pathways affecting colorectal cancer cell migration and invasion. The RT-qPCR results showed that the mRNA expression levels of CCR7, CCR9, CXCR5, and CXCR4 were significantly reduced (Fig. 5).

mRNA expression levels of CCR7, CCR9, CXCR5, and CXCR4 were significantly downregulated upon CCX-CKR overexpression in cell lines.
We further examined the mRNA expression of CCX-CKR, CCR7, CCR9, CXCR4, and CXCR5 in 10 samples of colorectal cancer tissues. The results were divided into 2 groups depending on the high or low CCX-CKR expression. In line with our previous findings, we found that, compared to the CCX-CKR low-expression group, the CCR9 and CXCR4 mRNA were downregulated in the CCX-CKR high-expression group, whereas CCR7 and CXCR5 mRNA levels showed a decrease that did not reach statistical significance (Fig. 6).

mRNA expression levels of CCR7, CCR9, CXCR5, and CXCR4 were significantly downregulated upon CCX-CKR overexpression in cancer tissues.
Discussion
This study is the first analyzing CCX-CKR expression in pathological samples from human colorectal cancer patients. We found that in colorectal cancer tissues the expression of CCX-CKR was reduced, in accordance with previous results from gastric cancer tissues (21) but not from breast cancer samples (20). It is conceivable that the gastric tissue is somehow similar to the colorectal tissue; additionally, only few control samples of normal breast tissues were used in the abovementioned study.
Our results showed that the upregulation of CCX-CKR was negatively correlated to the presence of lymph node metastasis, and that its upregulation was mainly observed in TNM stage I and II patients, and associated to a significantly higher survival rate. Taken together these results imply that CCX-CKR upregulation may act inhibiting cancer metastasis, and thus represents a positive factor in colorectal cancer prognosis (19–21).
Multiple chemotactic factors and their receptors are considered important regulators in cancer metastasis (3–5), e.g. CXCR4/CXCL12 (7, 8, 24), CCR9/CCL19 (CCL21), CCR9/CCL25, and CXCR5/CXCL13 (25–27). Targeted therapy could reduce the tumor size, and decrease the metastasis rate in different types of cancers, such as gastric cancer, breast cancer, lung cancer, colon cancer, prostate cancer, and melanoma (10, 25–40). Despite the fact that CCX-CKR can bind and clear CCL19, CCL21, CCL25, and CXCL13, we found that the mRNA expression of these ligands was not changed upon variation of CCX-CKR levels. This is due to the fact that these factors were not secreted by cancer cells, and thus the changes of CCX-CKR levels only caused changes at the protein level (19).
In the present study we found that CCX-CKR can down-regulate the mRNA levels of its endogenous receptors, including CCR7, CCR9, CXCR5, as well as of CXCR4. In future studies it will be important to further investigate how the feedback loop can in fact regulate the variations in the expression of these receptors with specific signaling pathways.
In conclusion, the present study shows that the upregulation of CCX-CKR is negatively associated with lymph node metastasis of colorectal cancer, and positively associated with the OS rate. CCX-CKR could inhibit the migration and invasion of colorectal cancer cells, without affecting cell growth and proliferation. The potential underlying mechanism might be the clearance of relevant ligands at the protein level, as well as the downregulation of CCR7, CCR9, CXCR5, and CXCR4 at the mRNA level. CCX-CKR therefore provides a novel prognostic factor for colorectal cancer patients’ survival, as well as a valuable target for relevant therapies.