
Abstract
Objectives
To determine the levels of carbohydrate antigen 125 (CA125) and tissue polypeptide-specific antigen (TPS) in saliva of patients with oral squamous cell carcinoma (OSCC) and patients with nonneoplastic disease of the oral cavity, and to investigate their diagnostic value and their relationship with pathological grade and clinical stage.
Methods
A total of 97 hospitalized patients with OSCC, 36 patients with nonneoplastic disease of the oral cavity and 50 healthy individuals were included in this investigation. Mixed saliva was collected from these patients and the healthy controls before treatment. Saliva samples were analyzed by enzyme-linked immunosorbent assay (ELISA).
Results
The saliva CA125 and TPS concentrations were significantly higher in patients with OSCC than in patients with nonneoplastic disease and healthy controls, but not significantly different between patients with nonneoplastic disease and controls. Neither the saliva CA125 nor the TPS level was correlated with pathological grade and clinical stage. The sensitivity, specificity and accuracy of saliva CA125 and TPS for the diagnosis of OSCC were 80.0%, 66.0%, 75.7%, and 82.1%, 74.0%, 79.3%, respectively. When CA125 and TPS were analyzed independently, there was no significant difference in sensitivity, specificity and accuracy between the two markers. When CA125 and TPS were analyzed in combination, there was no significant difference in sensitivity, specificity and accuracy between independent detection and combined detection.
Conclusions
The saliva CA125 and TPS concentrations were elevated in patients with OSCC. CA125 and TPS may prove to be useful tumor markers in OSCC.
Keywords
Introduction
Oral squamous cell carcinoma (OSCC) is a common human malignancy, with an increasing incidence (especially in younger people) and a 5-year mortality rate of 50% (1), which has not changed significantly in more than 50 years (2). Most oral cancers are superficial and easily detected, but sometimes it is difficult to distinguish between OSCC and precancerous lesions such as oral lichen planus, leukoplakia, lesions with dysplasia, and persisting ulcer. In addition, postoperative radiotherapy and/or covering the resection site with reconstructive flaps (regional or free vascularized) often makes early diagnosis an impossible task. The determination of biomarkers as a means to obtain an early diagnosis of cancer and find possible therapeutic targets is an important development in the clinical setting.
Highly sensitive tumor-specific marker tests may help to detect cancer at an early stage and hence increase the success of treatment (3). Tumor markers in saliva can be an attractive, effective alternative to markers in serum as salivary testing is noninvasive. A study found that the reported increase in salivary tumor markers may be used as a diagnostic tool, especially when a concurrent analysis for significantly increased markers is done (4). The tumor markers carbohydrate antigen 125 (CA125) and tissue polypeptide-specific antigen (TPS) have been reported to have potential clinical value for OSCC (5). A study showed that serum TPS was significantly higher in patients with OSCC than in healthy controls (6). The purpose of the present study was to determine the levels of CA125 and TPS in saliva of patients with OSCC, and to investigate their diagnostic value and their relationship with clinical stage and histological differentiation.
Materials and Methods
Materials
Between March 2010 and January 2011, 97 hospitalized patients with histologically confirmed OSCC who were treated at the Department of Oral and Maxillofacial Surgery, Capital Medical University School of Stomatology in Beijing were included in the study. The diagnosis of OSCC was confirmed in each case by a pathology report based on histological examination. The patients included 57 men and 40 women with a median age of 61.62 years (range 34 to 83 years). The primary cancer sites were tongue (36), gingiva (30), buccal mucosa (16), floor of mouth (10) and palate (5). Of the 97 lesions, 42 were well differentiated, 46 moderately differentiated, 1 poorly differentiated and 8 were carcinoma in situ according to the WHO classification (7). The clinical stage distribution of the 97 patients according to the UICC classification (8) was as follows: stage I, 39; stage II, 17; stage III, 11; and stage IV, 30. All patients were treated with curative surgery. Thirty-six patients with nonneoplastic disease of the oral cavity were also examined. The patients included 22 men and 14 women with a median age of 60.89 years (32 to 78 years), and the lesions consisted of leukoplakia (16), lichen planus (12) and persisting ulcer (8). The diagnosis of the nonneoplastic lesions was confirmed by pathology.
The control group consisted of 50 age-matched (28-85 years, mean: 62.26) healthy individuals without known signs of cancer or inflammatory diseases, who had the same sex distribution (29 men and 21 women) as the patients with OSCC. They were staff and faculty members of our Hospital and School of Stomatology. The samples were collected at the time of regular physical checkups.
Saliva sample collection
Whole saliva was collected shortly before the administration of definitive therapy (radiation, chemotherapy, surgery) under nonstimulatory conditions in a quiet room between 7 AM and 8 AM before eating and at least 7 days after the patients underwent biopsy. Those patients and controls who regularly took antihypertensive drugs, anticoagulants, hypoglycemic drugs or any other medication were advised to stop taking these 3 days before saliva collection. Patients were asked to generate saliva (at least 2 mL) and to spit into a wide test tube for 10 minutes. Following collection, the saliva was immediately centrifuged at 3000 r/min at 4°C for 20 minutes to remove squamous cells and cell debris. The resulting supernatant 1.5 mL saliva was used for further biochemical analysis. All samples were kept frozen and stored at −80°C until assayed. Repeated thawing and freezing of samples was avoided. Saliva samples were slowly melted at 4°C before analysis (9).
Assessment of salivary tumor markers
The concentrations of CA125 and TPS were measured with a commercially available ELISA kit (National Instruments Corporation, Austin Texas US) according to the manufacturer's instructions regarding pipette standards, controls and samples per well (CA125 100 μL; TPS 50 μL). Two empty wells were left for background absorbance measurement (blank). One hundred microliters ELISA HRP conjugate was added to each well except the blank wells and incubated for 2 hours±10 minutes on a shaker. The wash solution was prepared by dissolving 1 wash tablet in 500 mL deionized water. The wells were aspirated and washed 3 times with 0.3 mL wash solution, then TMB substrate was added to each well (CA125 100 μL; TPS 200 μL) including the blank wells, and incubated in the dark for 20±1 minutes. Fifty microliters stop solution was added to each well followed by shaking on a shaker for 1 minute. The absorbance was read at 450 nm within 30 minutes of addition of the stop solution.
Statistical analysis
Statistical analysis was performed with the SPSS 17.0 software (SPSS, Inc., Chicago, IL, USA). P values <0.05 were considered significant. Normally distributed data were expressed as means±standard deviation, and data with a skew distribution were expressed as medians and range. We used nonparametric statistical analyses to calculate the differences between groups. Logistic regression was used to analyze the sensitivity, specificity and accuracy of the 2 markers. To compare percentages we performed chi-square analysis.
Results
Saliva CA125 and TPS levels in patients and controls
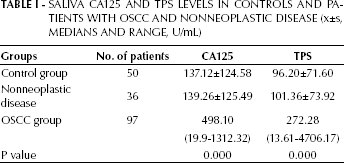
Saliva CA125 and TPS levels were significantly higher in OSCC patients than in patients with nonneoplastic disease and healthy individuals (p<0.05), but not significantly different between patients with nonneoplastic disease and healthy controls (p>0.05). The cutoff levels of CA125 and TPS were 342.05 U/mL and 213.98 U/mL, respectively, corresponding to the upper limits of the 95% confidence intervals (X+1.645S) of the 2 markers in the control group (Tab. I). Linear regression and correlation analysis were used to determine the effects of age on CA125 and TPS levels in the control group, which showed that there was no significant correlation between CA125 and TPS levels and age (p=0.515 and p=0.509, respectively).
Saliva Ca125 And Tps Levels In Controls And Patients With Oscc And Nonneoplastic Disease (X±S, Medians And Range, U/Ml)
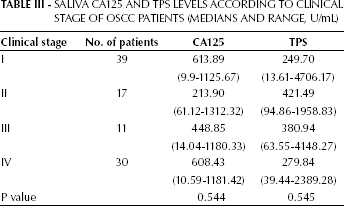
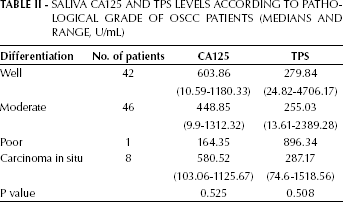
Saliva Ca125 And Tps Levels According To Pathological Grade Of Oscc Patients (Medians And Range, U/Ml)
Saliva Ca125 And Tps Levels According To Clinical Stage Of Oscc Patients (Medians And Range, U/Ml)
Relationship of saliva CA125 and TPS levels with histological differentiation and clinical stage
Different saliva CA125 and TPS concentrations were found in tumors with different histological differentiation (Tab. II) and different stage (Tab. III), but the difference was not significant and neither saliva CA125 nor TPS levels were correlated with these 2 parameters (p>0.05).
Diagnosis of OSCC based on saliva CA125 and TPS
The sensitivity, specificity and accuracy of saliva CA125 and TPS for the diagnosis of OSCC were analyzed by logistic regression (Tab. IV). When CA125 and TPS were analyzed independently, TPS had higher sensitivity, specificity and accuracy. But chi-square analysis showed that there was no significant difference in sensitivity, specificity and accuracy between CA125 and TPS (p=0.711, p=0.383 and p=0.401, respectively). When CA125 and TPS were examined in combination, the combined detection had higher sensitivity, specificity and accuracy than that of CA125 alone, but there was no significant difference between combined detection and detection of CA125 alone in sensitivity, specificity and accuracy (p=0.575, p=0.517 and p=0.401, respectively). Combined detection had higher sensitivity and lower specificity than TPS alone but the same accuracy as TPS alone. There was no significant difference between combined detection and detection of TPS alone in sensitivity, specificity and accuracy (p=0.848, p=0.822 and p=1.00, respectively).
Sensitivity, Specificity and Accuracy of CA125 AND TPS for the Diagnosis of Oscc
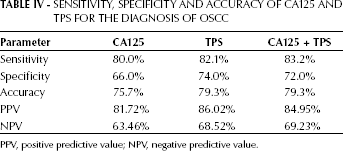
PPV, positive predictive value; NPV, negative predictive value.
Discussion
Bast et al first reported on CA125 in 1981 (10). They developed a radioimmunoassay for CA125 and found that the serum level of CA125 was increased in more than 80% of women with epithelial ovarian cancer and in less than 1% of healthy controls. In 2001, the gene encoding CA125 was found to be located on chromosome 17 (11, 12). An immunohistochemistry study showed that in normal conditions embryonic alimentary canal epithelium, amniotic membrane, adult pleura and abdominal cavity mesothelial cells produce CA125, and that CA125 expression is upregulated in malignant tumor cells and the protein released into the circulation (13).
Estimation of serum CA125 was first used to study ovarian cancer, when it was found that serum CA125 levels correlated with clinical stage, histological differentiation and lymph node metastasis, and serum CA125 levels could be used as an adjunct in monitoring treatment response (14).
One study examined the immunohistochemical expression of CA125 in mucoepidermoid carcinomas and adenoid cystic carcinomas from salivary glands. There was no correlation between positive expression of CA125 and the clinical course of patients (15). There have been few reports on studies of saliva tumor markers in oral cancer. Nagler et al examined saliva CA125 in 21 patients with squamous cell carcinoma of the tongue (4). They found that the saliva CA125 concentrations were significantly increased in patients with OSCC, but because of the limited number of patients, the true value of saliva C125 as an OSCC marker needed to be further determined. In the present study, a larger sample (97 cases of OSCC arising from different sites of the oral cavity) was investigated to confirm the previous findings.
TPS was first described by Bjorklund et al in 1957 (16). TPS is a tumor proliferation marker whose levels in serum increase when rapid cell divisions occur. Hepatic cells, mammary gland duct, endocrine cells, thyroid gland and prostate gland produce TPS. Malignant epithelial tumor cells also produce TPS (17). Bjorklund et al reported that TPS may be a potential tumor marker (18). Serum TPS level indicates tumor activity before breast cancer is clinically manifested and even if the mass is small (19). TPS is released into the circulation during cellular degradation and its level can be determined in serum (20).
Increased serum TPS levels have been found in several kinds of malignant tumors including lung cancer (21), pancreatic cancer (22), prostatic carcinoma (23) and urothelial cancer (24). The serum TPS level was also found to be significantly higher in OSCC patients than in healthy individuals, and the sensitivity and specificity of serum TPS for the diagnosis of OSCC was 87% and 69%, respectively (6). Nagler et al (4) investigated saliva TPS levels in 21 patients with OSCC and found that TPS concentrations were significantly higher in patients with OSCC than in healthy controls.
The present study showed that both saliva CA125 and TPS levels were significantly higher in OSCC patients than in patients with nonneoplastic disease and healthy individuals, but not significantly different between patients with nonneoplastic disease and healthy controls. A concurrent analysis of the 2 significantly increased markers revealed a sensitivity and a specificity of 83.2% and 72.0%, respectively, which are higher than those (71% and 75%) reported by Nagler et al (4). This suggests that the increase in saliva CA125 and TPS levels may provide additional diagnostic markers to be used with other parameters and physical examinations, and the 2 markers may also be of value in the differential diagnosis between OSCC and nonneoplastic diseases of the oral cavity. We also found that there was no significant difference between CA125 and TPS in sensitivity, specificity and accuracy, suggesting that CA125 and TPS may have the same value as tumor markers for oral cancer. In the current study, the relationship between CA125 and TPS and histological differentiation and clinical stage was also analyzed. However, saliva CA125 and TPS levels were found not to correlate with histological differentiation and clinical stage.
The diagnostic value for malignant tumor is limited if only 1 tumor marker is examined (25). Two markers were therefore tested in combination in this study with the aim of increasing the diagnostic value. When concurrent analysis of CA125 and TPS was done, combined detection had higher sensitivity, specificity and accuracy than detection of CA125 or TPS alone, but the difference did not reach statistical significance.
In conclusion, the present study showed that saliva CA125 and TPS concentrations were elevated in OSCC patients, and their sensitivity, specificity and accuracy were relatively high, which suggests that these substances may prove to be useful as diagnostic aids for oral cancer. In addition, salivary tumor marker testing is encouraging in view of the many advantages of saliva measurement in comparison with serum analysis.
Footnotes
Acknowledgment
The authors thank Professor Sun Zhen for her suggestions and help in the research proposal and paper writing.