
Abstract
Background:
Conservative treatment of lateral clavicle fractures (Neer type II) often ends with unsatisfactory results for patients. Operative treatment is thus gaining acceptance. A retrospective study found success using a double plate technique for these injuries. For the current study, a standardized testing setup was developed to compare the mechanical properties of single versus double plate technique for lateral clavicle fractures.
Methods:
Six synthetic bones were tested for each technique. Neer type IIB fractures were created using computer-aided design (CAD). Fatigue testing was carried out with a cantilever bending test. Parameters measured were cycles undergone, failure load and stiffness at the point of failure.
Results:
The standardized testing setup was able to provide reproducible failures. The double plate technique lasted about 16,000 more cycles and withstood an additional 22.4 N on average.
Conclusions:
The new modified standardized testing setup produced reproducible fixation failures for both clavicle fracture fixation techniques. The double plate technique seems to be mechanically superior to the single plate technique.
Introduction
Fractures of the clavicle are common, especially among adolescents and young, active adults. They represent 2.6% of all fractures, with an overall incidence of 64 per 100,000 (1, 2). Of these, approximately 21% occur laterally (3). Fractures of the lateral clavicle remain a challenging problem in orthopedic practice. They can be classified as Alman group 2 fractures (4). Neer (5) adopted this classification, but subdivided group 2 fractures into more specific types. Neer type II fractures are medial to the coracoclavicular (CC) ligaments, and therefore usually lead to significant displacement.
Lateral fractures are unstable in 25% of all cases (6, 7). Even if the distal fragment remains relatively in its anatomic position, whether the fragment will separate or not depends on the forces applied by the arm (8). The unacceptably high rate of nonunions in conservatively treated fractures is the result of this unstable fracture pattern (6, 9, 10).
Poor outcomes can be quite obvious, such as persistent pain, limitations of shoulder movement and/or compression of the brachial plexus. To avoid such complications, many authors (1, 2, 11-14) support open reduction and internal fixation if the indications described above are present. Thus, open reduction and internal fixation (ORIF) is gaining acceptance as a treatment for severe clavicle fractures and nonunions. If fixation is indicated, numerous surgical techniques can be implemented.
Although the use of internal fixation is technically demanding and associated with particular risks, because the brachial plexus and subclavian vessels lie just beneath the clavicle, it is among the most favored therapies for midshaft fractures (1, 15-18).
There are very few data available regarding lateral clavicle fractures and their treatment. When ORIF is indicated, plating remains one of the most favored treatments. Within the category of internal fixation with plates, there is still a variety of possible treatment options, ranging from an AO hook plate or locked plate fixation, to double plate fixation.
Double plate fixation was originally used to treat complex distal radius fractures (19). A retrospective case study (20) introduced the idea of using the double plate technique for lateral clavicle fractures and supported the idea by achieving good outcomes with stable fixation, even when the lateral fragments were small and comminuted.
In a biomechanical comparison study, locking compression plates (LCPs) were superior to typical implants for midshaft clavicle fractures (21). Therefore, it can be expected that precontoured LCPs are also better than typical implants for lateral clavicle fractures when ORIF is indicated.
The purpose of this present study was to define a standardized biomechanical testing setup to compare the mechanical properties of different fixation techniques for lateral clavicle fractures where there were indications for open reduction (Neer type II). The single plate technique was compared with the double plate technique. The main question was whether the double plate technique is similar to the single plate technique regarding its mechanical properties, thus either supporting or disputing the findings of the retrospective study that introduced the double plate technique for these fractures (20).
Materials and methods
The Neer type IIB was chosen as a fracture with indications for ORIF. This fracture occurs either between ruptured conoid and intact trapezoid ligaments or lateral to both ruptured ligaments. Either way, this leads to superior-posterior displacement of the medial fragment due to traction of the sternocleidomastoid muscle.
Using a 3-dimensional (3D) image file of a right clavicle (Sawbones, Malmo, Sweden), a Neer type IIB fracture was constructed using computer-aided design (CAD) (Autodesk Inventor 2012). Attention was paid to reproduce the fracture in an anatomically accurate manner. It was located lateral to the conoid tubercle and through the trapezoid line, as would occur with a torn conoid ligament and partially ruptured trapezoid ligament.
In addition, a series of 5 computed tomography (CT) scans of lateral clavicle fractures were reviewed, from our orthopedic unit patients and this prompted the creation of a third small fragment from, and localized inferior to, the lateral fragment. This type of fragment is often seen in lateral clavicle fractures because of anterolateral forces causing the fracture. (Fig. 1). Positioning of plates, screws and load transfers were standardized on the CAD image file.
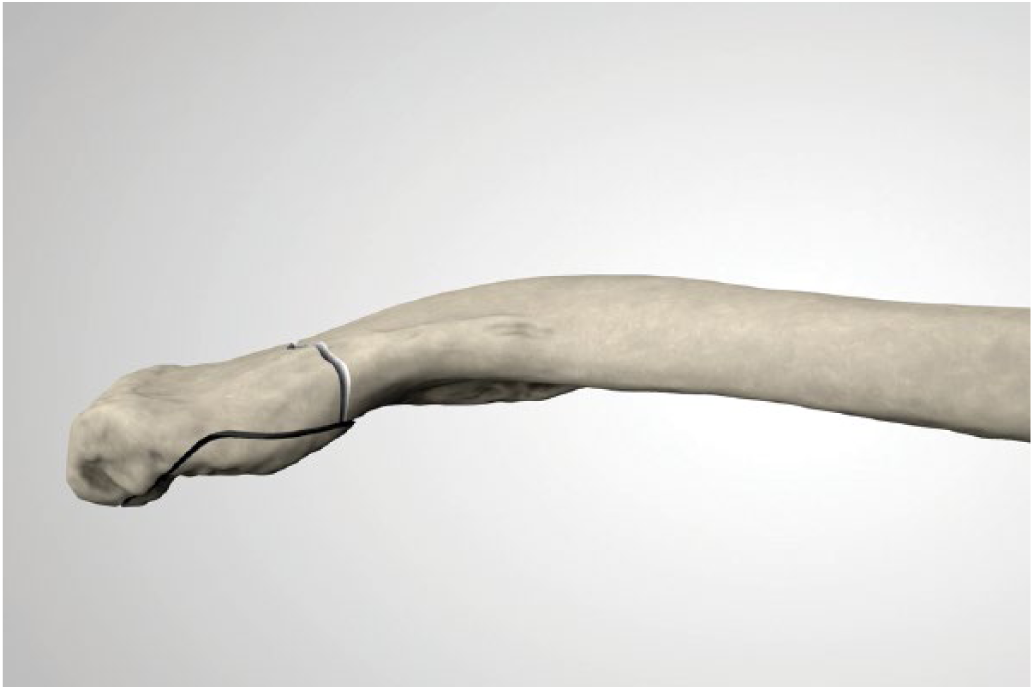
Computer-aided design depiction of a newly developed standardized lateral clavicle fracture in a model bone.
A construction assistant was also created with CAD, to make assembly relatively easy and to minimize the chances of performance bias.
Several studies (21, 22) have found that current synthetic bones have similar mechanical characteristics to cadaveric bones. In addition, regarding experiment design and reproducibility, the use of synthetic bones composition is more consistent and allows for lower standard deviations than cadaveric bone. It is also difficult on testing to judge the actual difference between cadaveric bones and bones in vivo. Hence for this study, synthetic bones were used. The fractures created on CAD were then produced as glass-fiber reinforced polyamide fragments (1by1; Dornbirn, Austria) as described in previous studies (23).
For both techniques, the plates were applied according to the manufacturers’ instruction manuals, which are available online. The single plate technique was performed with a superior anterior clavicle locking compression plate (LCP) with lateral extension (Synthes, Oberdorf, Switzerland). Three angle-stable bicortical screws of Ø 3.5 mm were used in the medial fragment. The lateral fragment was fixed with 6 angle-stable bicortical screws of Ø 2.7 mm.
The double plate technique was performed using a locking T-plate (A-4655.16) and a locking, straight 8-hole plate (A-4655.08). Both of these were originally indicated for ORIF of metacarpal and carpal fractures (Medartis, Basel, Switzerland). The T-plate and straight 8-hole plate were each attached with 6 bicortical locking screws Ø 2 mm, with 3 screws in each fragment for both plates.
A (superior-inferior) cantilever bending test was used to examine biomechanics. This test simulates in vivo forces on the clavicle and is quite accurate regarding fixation of the medial end of the clavicle through the sternoclavicular joint (24, 25).
A mounting block for the medial fragment was already assigned on CAD, to allow attachment to a bench vice. Point of load application was placed on a small block very much distal on the lateral fragment.
Testing was carried out on a servo-electric load frame (Thelkin, Winterthur, Switzerland) with a 2 kN load cell (Burster, Gernsbach, Germany). Loadframe SX software (Version 1.5.0) was used (Fig. 2).
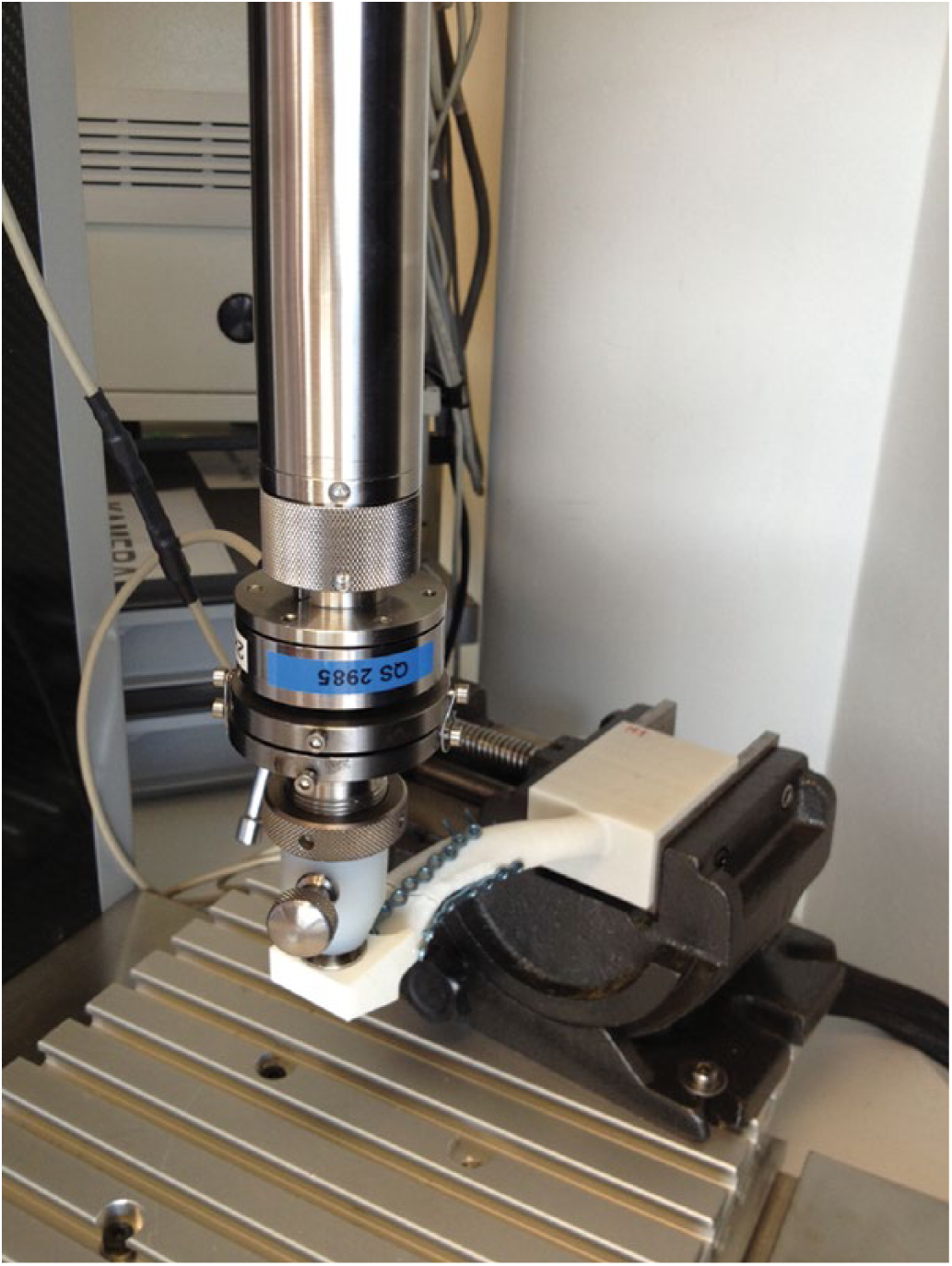
Test setup with mounted sample during testing.
It appears that the greatest forces on a repaired clavicle occur within the first 6 to 12 weeks after ORIF. The implant is most loaded at the beginning of the healing process as the broken bone does not contribute to load sharing. As the healing process of the bone progresses, load will be shared increasingly between plate and bone. This process was simulated inversely in the loading regime.
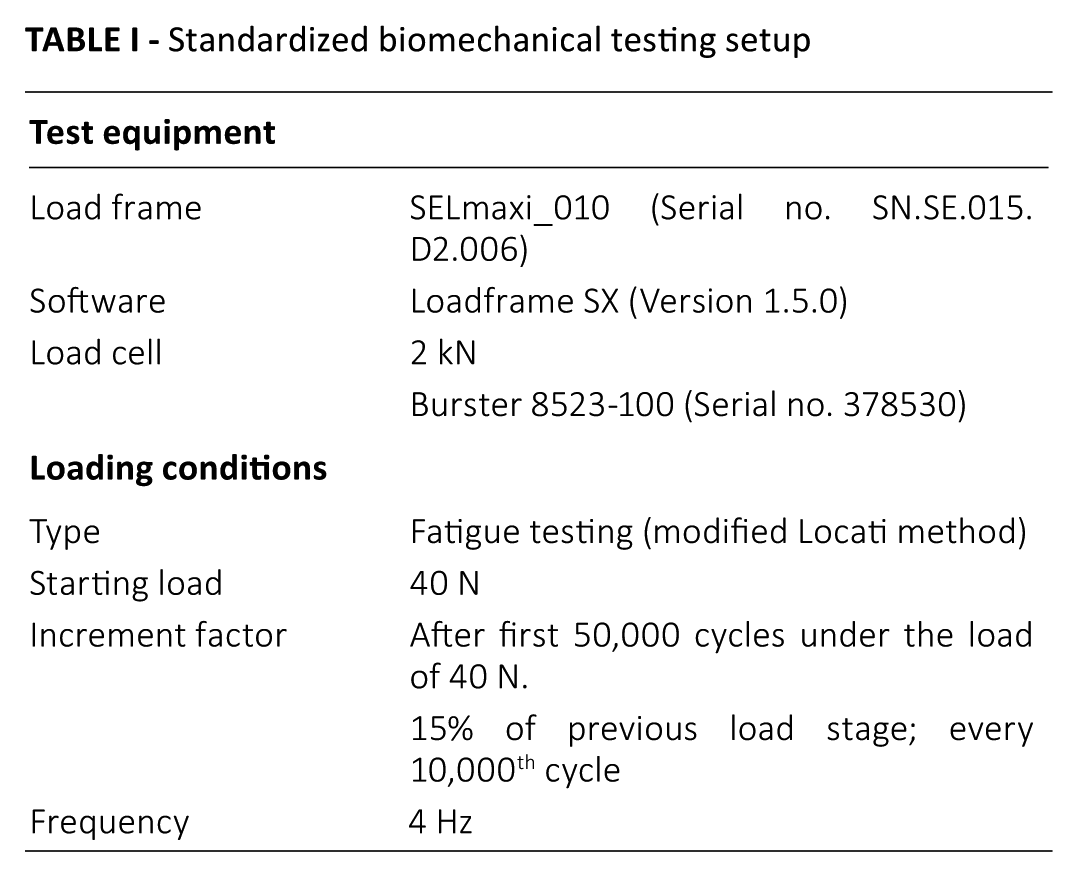
After 12 weeks at the latest, the bone should be united. Assuming there are approximately 500-1,000 stresses per day, plates must overcome a maximum of 100,000 stresses until bone union occurs. This estimate of 500-1000 stresses is based on the assumption that the fractured clavicle will not move most of the time, due to the pain associated with movement; movement therefore occurs during controlled training (physiotherapy), which typically does not exceed 1 hour per day. If a single exercise takes 5-10 seconds, roughly 500 repetitions (i.e., loading cycles) may be performed per day. Therefore, to evaluate fixation technique thresholds during fatigue testing, failure should occur around the 100,000th cycle. To achieve failure at this point, a modified Locati method was used for the loading regime (26) (Tab. I).
Standardized biomechanical testing setup
This modified Locati method works well with other approaches as well, because it always leads to failure, and thus, a relatively large amount of information can be yielded from a few specimens (26, 27) (Fig. 3).
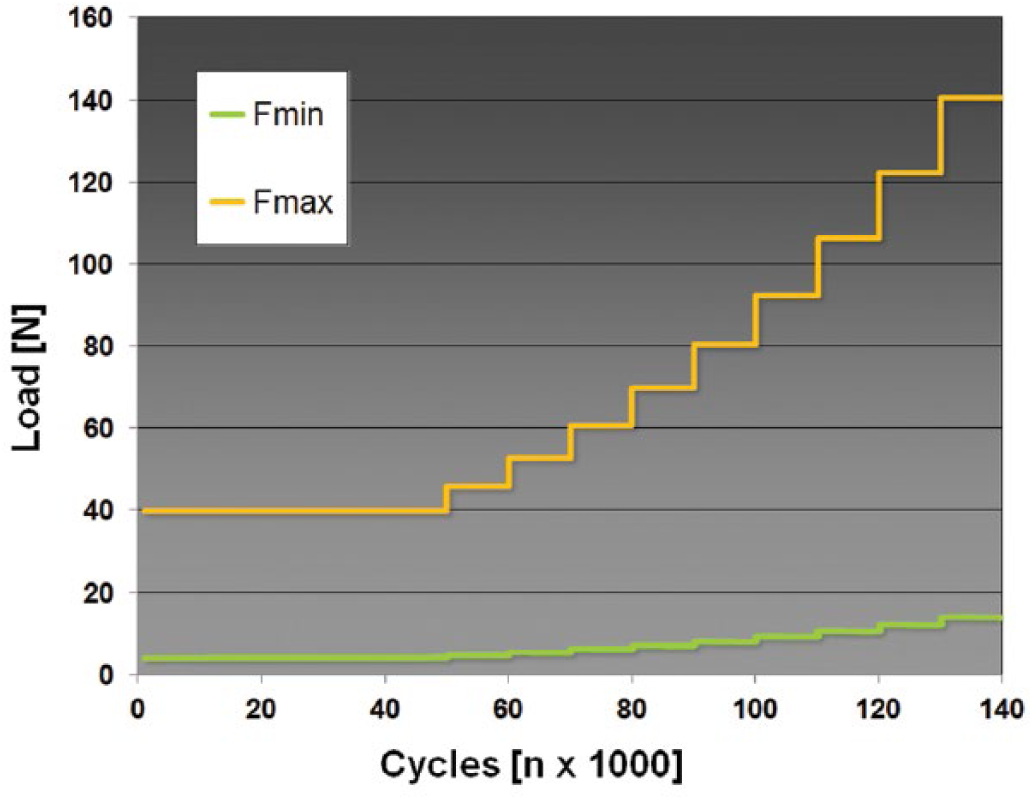
Visualization of modified Locati method as loading regime, with a starting load at 40 N. F = force.
No standardized loading forces were available for this type of biomechanical study for lateral clavicle fractures. Minimal data were available regarding physiological loading of the clavicle (24), and other biomechanical tests of the lateral clavicle have had different test designs or setups (7, 8). Thus, the starting load needed to be determined through a pretest.
The pretest provided a starting load of 40 N at 4 Hz. The first 50,000 cycles were run under a load of 40 N. Subsequently 15% of the previous load stage was added to the load after every 10,000th cycle, to accomplish failure after approximately 100,000 cycles (Fig. 3).
For the final testing, 12 synthetic bones, with 6 specimens for each technique, were used. Statistical analysis of failure load, cycles undergone and stiffness (N/mm) at the point of failure was performed using the Wilcoxon rank sum test. Statistical significance level was determined as a p value <0.05.
Results
All 12 specimens were successfully tested, and failure was reached in a standardized manner with the cantilever bending test (Tab. II).
Mean results of cantilever bending test
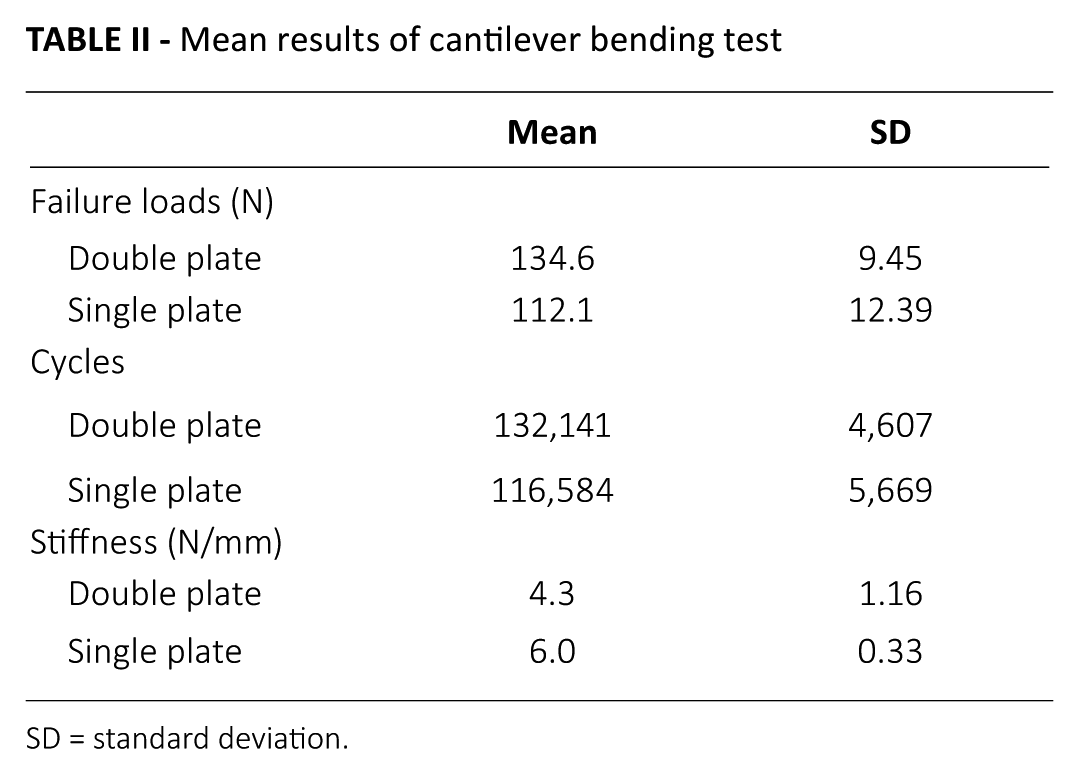
SD = standard deviation.
Compared with those with a single plate, specimens with the double plates underwent significantly more cycles until failure (p<0.001), and also withstood significantly higher loads at failure (p<0.01) (Figs. 4 and 5). Specimens of both techniques outlasted 100,000 cycles, which represent the first 5 to 6 weeks after ORIF. At the point of failure, the single plate specimens were significantly stiffer at the point of failure than those with 2 plates (p<0.05). Throughout the testing, single plate specimens were stiffer than double plate specimens at each loading stage, as they had shorter testing periods overall.
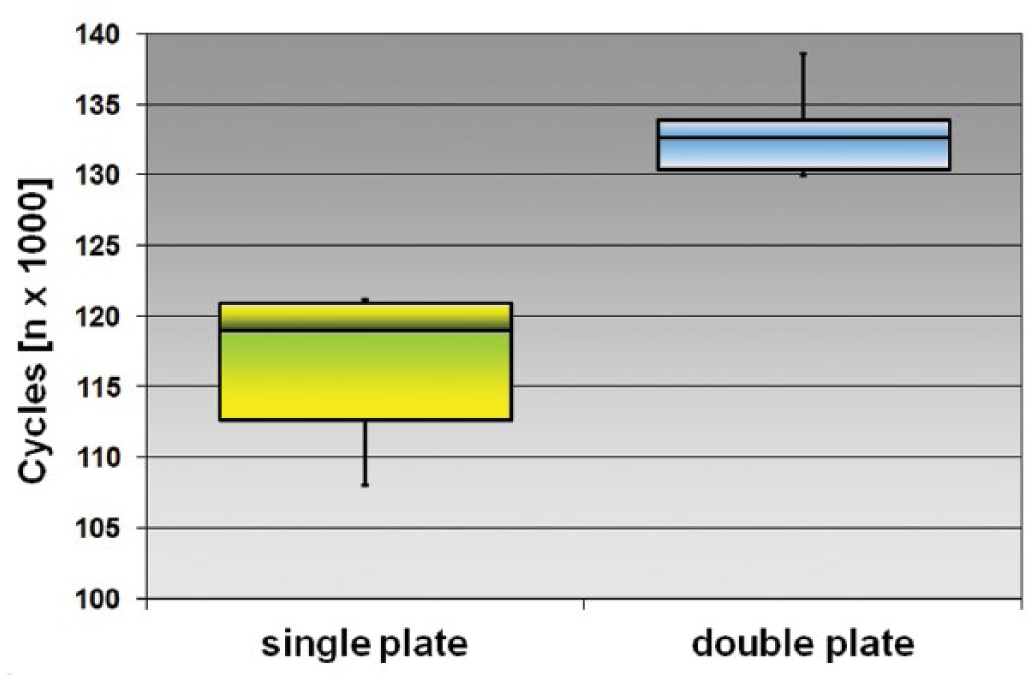
Box plot of cycles undergone until failure: double versus single plate technique.
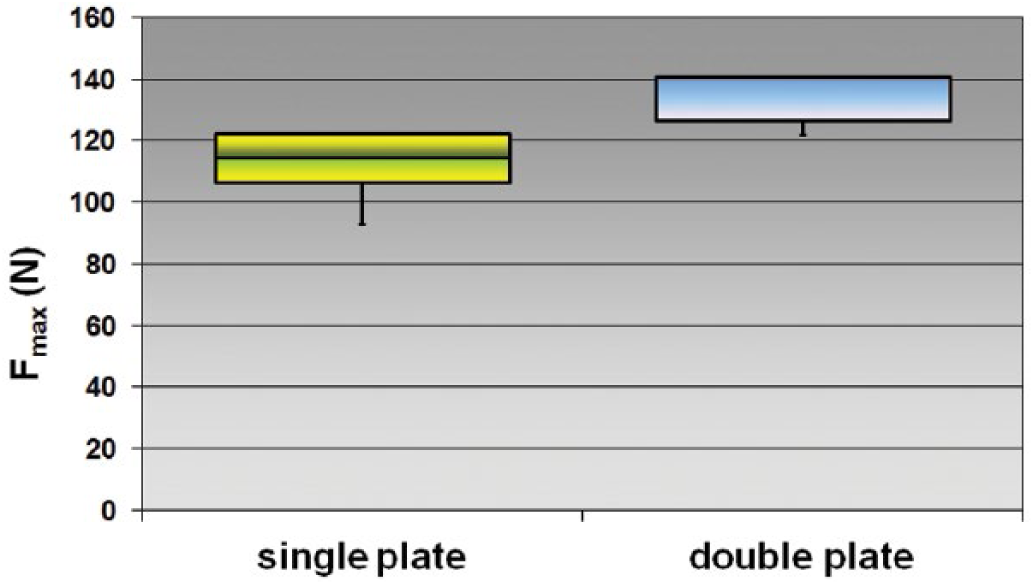
Box plot of load failure: double versus single plate technique. F = force.
The mode of failure was comparable for all single plate clavicles. The most medial locked screw appeared to have a predetermined breaking point. A new fracture was induced near the most medial screw in every single plated specimen (Fig. 6). There were 2 modes of failure for the double plated clavicles. In 3 cases, the superior T-plate failed (Fig. 7A). For the other 3 cases, the clavicle failed adjacent to the medial clamping block (Fig. 7B).
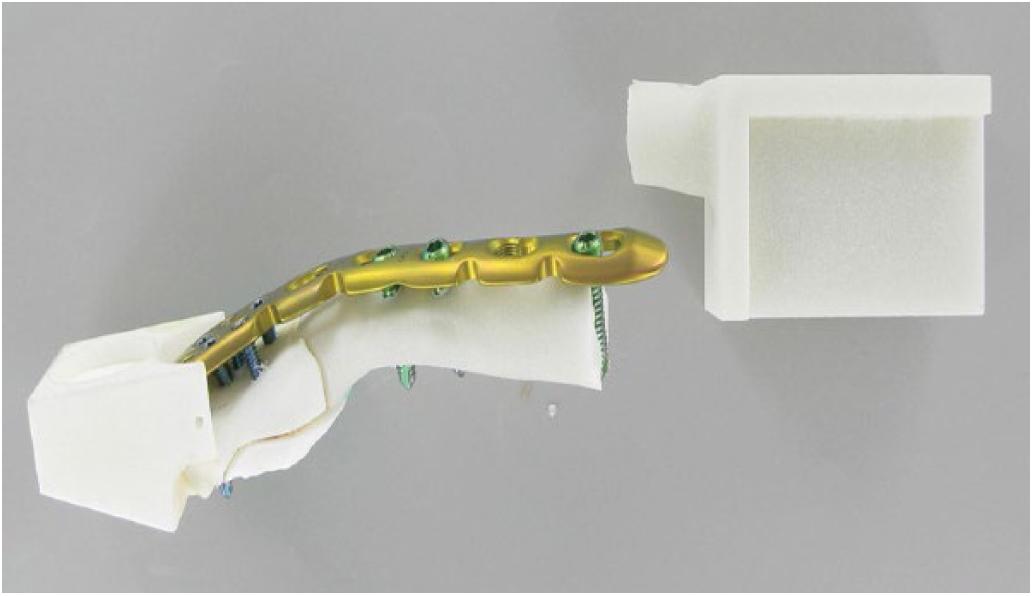
Photograph showing mode of failure with the single plate technique.
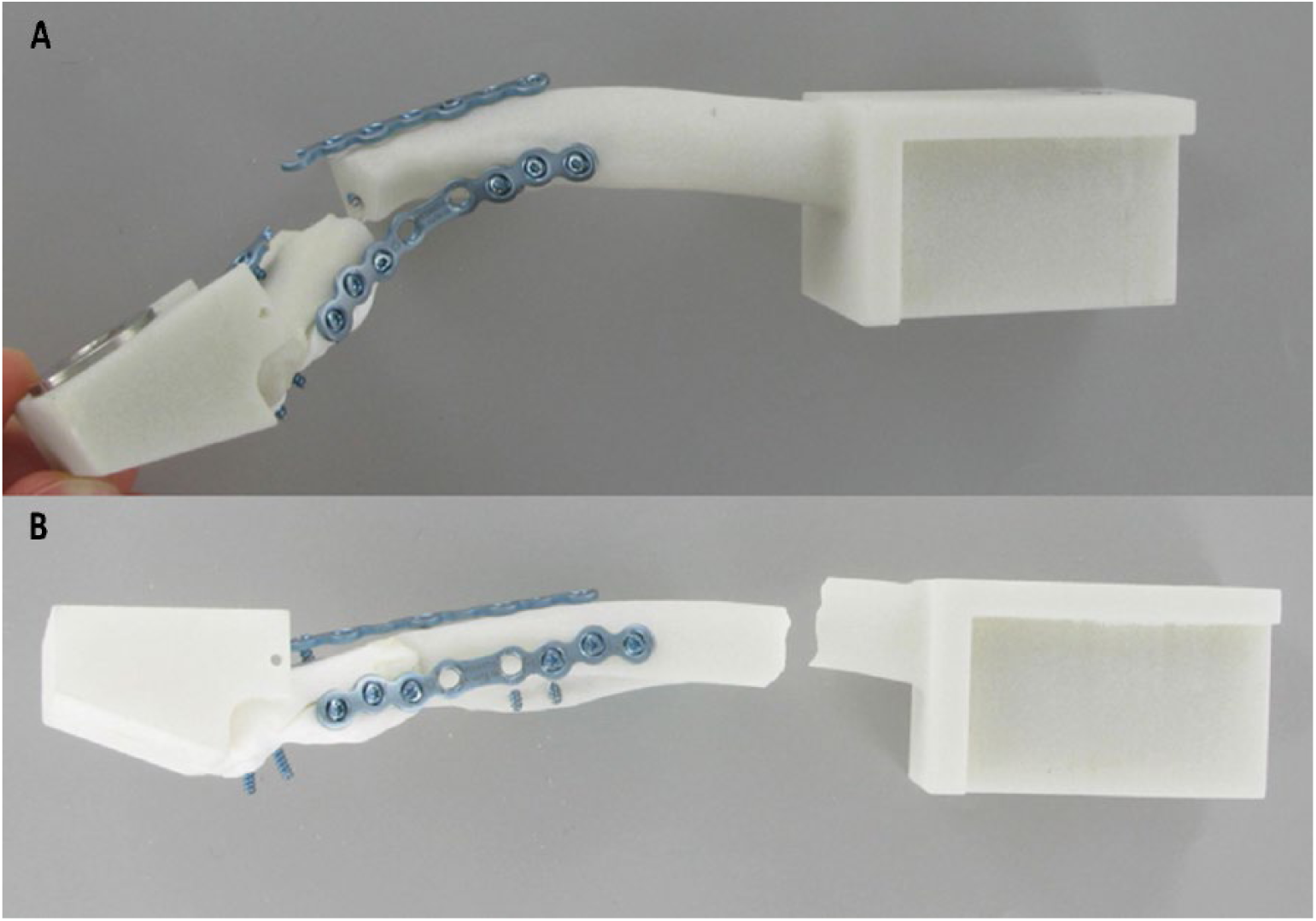
(
Discussion
The new modified standardized testing setup produced reproducible fixation failures for both clavicle fracture fixation techniques. Both techniques withstood at least 100,000 cycles, which is comparable to the loads experienced during the first 6 to 12 weeks after surgery. Therefore, under circumstances as demanding as the load regime used in this study, both techniques should sufficiently stabilize Neer type IIB fractures until bony union is attained.
The stiffer single plate does not lead to plate failures, but instead to periimplant clavicle fractures at the weakest point with the longest lever arm: the region of the most medial screw. This manner of failure is consistent with the results in many other biomechanical studies on the clavicle comparing LCP with different internal fixation techniques (8, 21, 25, 28, 29). Although this manner of failure is not as common as the axial pull-out of the superior LCP, it has also been described in case reports (30, 31).
Therefore, it is questionable whether the double plate technique is actually more resilient against failure. This is also because the manner of failure described in this and many other biomechanical studies, is not what is seen most frequent clinically. Nevertheless, this standardized test setup did show that double plate fixation also provides sufficient stabilization for severe distal clavicle fractures in the first 12 weeks until bony union is reached.
In the end, the double plate specimens endured an average of 16,000 cycles more than the single plate clavicles. Considering the failure load, the double plate technique was also superior to the single plate technique, bearing an additional 22.4 N on average.
In summary, considering the mechanical properties of the 2 techniques for treating lateral clavicle fractures, the double plate technique appears to be better.
There are very few published data regarding the treatment of lateral clavicle fractures, and no biomechanical study with a similar test setup is available. The few biomechanical studies investigating lateral clavicle fractures that are available either did not use a cantilever bending test and/or they used a different type of loading regime (7, 8).
According to the available literature, this type of biomechanical study should be performed using a bending test, since there are many biomechanical studies of midshaft fractures using this type of test. Many of these studies are carried out with a 3-point bending test (21, 29, 32). However, this approach seems nonphysiological, as there is no anatomical structure under the clavicle serving as a thrust block as there is in a 3-point bending test. Therefore, the cantilever bending test seemed more appropriate for our purpose, and has been supported also by other authors (24, 25).
Another biomechanical study (33) investigating the forces acting on a healthy clavicle during abduction and internal/external rotation showed that the greatest force comes in the form of axial compression during arm abduction, supporting the idea of testing a clavicle through axial compression. It would be interesting in the future to compare double versus single plate technique for compressive failure load as well.
This is one of the limitations of this study: that only one form of biomechanical testing was carried out. Another limitation is the use of artificial bones. Although artificial bones are preferable to cadaver bones regarding reproducibility, they are still not the same material.
This is the first biomechanical study regarding this topic to define and validate the testing procedure with a new standardized testing setup. The next step will be the evaluation of cadaver specimens.
Another aspect of the 2 plating techniques presented in this study is the cosmetic one. In many cases the single plate technique will quite obviously mark the treated clavicle, as the plate is bulkier. The double plate technique offers a more discreet solution. On the other hand, using 2 plates also requires broader denudation of the fracture site, as both the superior and anterior facets of the clavicle must be exposed. This does offer the surgeon more ease in reaching anatomic reduction under direct visualization (20).
Conclusion
The new modified standardized testing setup used in this study produced reproducible fixation failures for both clavicle fracture fixation techniques. The double plate technique seemed to be mechanically superior to the single plate technique.
Further upcoming biomechanical tests on lateral clavicle fractures are desirable, especially with cadaver bones and/or testing axial-compressive failure loads.
Footnotes
Disclosures
Financial support: The study was financially supported by Medartis AG, Switzerland.
Conflict of interest: None of the authors has any financial interest related to this study to disclose.