
Abstract
The study was carried out to explore the biomechanical properties of embracing and non-embracing rib plates. Forty-eight adult cadaver rib specimens were divided randomly into six groups: three fixation model groups were made using embracing plates (two pairs of equals on both sides of the broken end), and the other three groups were fixed with a pre-shaped anatomical plate (three locking screws on each side of the end were equally spaced). The biomechanical properties of these models were analyzed using non-destructive three-point bending tests, non-destructive torsion experiments, and destructive axial compression tests. In this study, the gap of fracture ends was widened in embracing plate group in the non-destructive three-point bending experiment. No change in the fracture ends was detected in the pre-shaped anatomical plate group. The bending stress of the pre-shaped anatomical plate group was significantly enhanced at the 2–12 mm displacement points (p < 0.05). Moreover, there was no significant difference in torque noticed between the two groups in the torsion experiment (p = 0.082). In the destructive axial compression experiment, the load index of the two groups were higher than the normal physiological load, suggesting that both materials could provide sufficient strength for rib fractures. The pre-shaped anatomical plate displayed more reliable attachment in terms of stability, bending, and load. Our results indicated that the embracing plate has the advantage of fretting at the fracture end.
Introduction
Rib fracture resulting in flail chest is considered as an extremely severe and common blunt injury of the chest wall, which accounts for about 10% of all trauma cases. 1 Multiple rib fractures, especially the flail chest can induce a variety of adverse physical reactions, including severe pain, cough weakness, local abnormal respiratory movements, combined lung parenchymal injury, and blood pneumothorax. Eventually, these adverse reactions may further lead to pulmonary infection, acute respiratory distress syndrome (ARDS), and other complications. 2 In recent years, open reduction and internal fixation surgeries have been widely used for correcting rib fractures because of its advantages such as the early establishment of a stable thorax, effective relief of pain, promotion of lung expansion, reduction of pulmonary complications, and shortening of hospital stay.3,4 Up to now, the common internal fixation methods in the clinic mainly include the embracing rib plate (titanium alloy or titanium nickel memory alloy), pre-shaped anatomical plate (non-encircling type/intramedullary plate), and semi-encircling type (U-shaped) plate. And various internal fixation materials are expended in the way of force and stress characteristics of the ribs due to the special geometry of human ribs. 5 In this study, we performed a series of in vitro biomechanical tests of the two commonly used internal fixation materials, the embracing rib plate and the non-circumferential pre-shaped anatomical plate. The analysis of the biomechanical properties of the two materials may provide a reference for the clinical selection of surgical intervention.
Materials and methods
Materials and equipment
The embracing rib bone plate was obtained from Changzhou Huasen Medical Device (HS A 45 × 15 mm). Clamping pliers and a pre-shaped locking rib plate was purchased from American Johnson & Rhythm MatrixRrib Anatomic (six holes and eight holes). Locking screw, special accessory equipment, and Electroforce 3520-AT biomechanical experiment system were obtained from Bose Company (USA). Biomechanical analysis software, three-point bending, and torsion test mold were obtained in Institute of Orthopaedics (China). Electric drill, oscillating saw, type II denture base tooth powder, and self-setting tooth water were brought from Shanghai New Century Dental Materials Co., Ltd. (China).
Specimen preparation
This study was approved by Ethics Committee of the 3rd Hospital of Hebei Medical University, China (No.20120333). Informed consent was obtained from family members of all enrolled subjects, and the methods were performed following the relevant guidelines and regulations.
Six male cadaver specimens were collected from the 3rd Hospital of Hebei Medical University (China). A total of 48 ribs, including the left and right rib 5–8 of each corpse, were frozen and stored at −20°C. Before the experiment, the ribs were taken out from the refrigerator and thawed at room temperature (23°C). Muscles were removed from the ribs. Meanwhile, other soft tissues attached to rins were also removed gently by preserving the periosteum. The ribs were cut into pieces with a length of 20 cm with oscillating saw. Normal temperature saline solution was sprayed on the surface of the specimen to keep the ribs moist during the experimental interval. All experimental ribs were free from any reported deformities, trauma, tumors, and other pathological changes. The inferior and superior sections of the specimen were also measured and recorded. The model of the internal fixing material was determined based on the inferior and superior section data. All 48 rib specimens were randomly divided into six groups (eight samples in each group): three of the groups were fixed with an embracing plate (two pairs of equals on both sides of the broken end), and the other three groups were fixed with a pre-shaped anatomical plate (three locking screws on each side of the end were equally spaced). Three groups fixed with an embracing plate or a pre-shaped anatomical plate were divided into non-destructive three-point bending test group, non-destructive torsion experiment group, and destructive axial compression test group. After the ribs were sawed at the midpoint, the anatomical alignment was fixed.
Experimental steps
In the normal physiological breathing movement of the human body, the ribs were subjected to multi-directional forces such as bending, twisting, and axial expansion and contraction. Therefore, we performed three loading models to probe the force characteristics of rib as described in previous studies.6–8
(1) Non-destructive three-point bending test: after one set of the embracing plate specimen model (Figure 1(a)) and one set of the pre-shaped anatomical plate specimen model (Figure 1(b)) were placed on the three-point bending model, a non-destructive three-point bending test was performed by an MTS Tytron 250 (MTS, Eden Prairie, MN, USA). The setting parameters were listed as follows: loading span = 100 mm, displacement speed = 2.5 mm/min, and maximum displacement upper limit = 12 mm. The point at which the force was applied was the midpoint of the fracture line. The computer recorded the position of the point changes of the force center and the corresponding force. The corresponding force load (unit: N) was recorded when the displacement of the fixed point reached 2, 4, 6, 8, 10, and 12 mm.
(2) Non-destructive torsion experiment: The other two embracing plate specimens (Figure 2(a)) and one set of the pre-shaped anatomical plate specimens (Figure 2(b)) were fixed vertically to the torsion test mold box with denture tooth powder and self-condensing water. The specific parameters were listed as follows: loading span = 100 mm, rotation speed = 10°/min, and the corresponding torque (unit: N cm) was recorded when the rotation angle was 5°, 10°, 15°, 20°, 25°, and 30°.
(3) Destructive axial compression force test: the two groups of control specimens were again fixed vertically to the mold box with denture tooth powder and self-condensing water. The loading protocol mainly followed a previously published study. 9 The biomechanical machine pressure probe automatically bounced to indicate the end of the test. The morphological characteristics, load displacement, and ultimate failure load (unit: N) in the different groups of the rib specimens were recorded.

Non-destructive three-point bending test: (a) embracing plate specimen model and (b) pre-shaped anatomical plate specimen model on three-point bending mold.

Non-destructive torsion experiment: (a) an embracing plate specimen model and (b) a pre-shaped anatomical plate specimen model on the torsion test mold box.
Data processing
Data processing was performed using Statistical Product and Service Solutions (SPSS) software (version 19.0, SPSS Inc., Chicago, IL, USA). Measurement data were expressed as mean ± standard deviation (SD). The t-test analysis was performed between the groups. p < 0.05 indicated significant differences between the compared groups.
Results
Rib parameter measurement results
In this study, we had measured the length and inferior section of each rib. The results showed that the average inferior section midpoint of 48 ribs was 14.34 ± 0.86 mm, and the average superior section midpoint was 8.28 ± 0.77 mm. Therefore, we selected a 45 × 15 mm embracing model plate and a 10 mm length pre-shaped anatomical plate locking screw to perform further studies.
Non-destructive three-point bending test results
In this study, from the side view (Figure 3(a)) and positive view (Figure 3(b)), the embracing plate produced a 1–2 mm gap widening at the fracture end when it was compressed. The embracing plate could turn back to the original state when pressure was relieved. Meanwhile, it was difficult to detect the changes in the fracture space in the pre-shaped anatomical plate with the side view (Figure 3(c)) and positive view (Figure 3(d)). Figure 4 showed that the load was gradually increased as the displacement increased in both groups. The slopes of both groups were decreased at a displacement of 8 mm. When the displacement was 10 mm, the highest load reached 44.08 ± 1.71 N for the embracing plate, and 76.48 ± 3.63 N for the pre-shaped plate. After a statistical analysis, there were significant differences in the load of the six displacement points (2, 4, 6, 8, 10, and 12 mm) (p < 0.05). The pre-shaped anatomical plates showed high intensity load compared with the embracing plate.

Change of fracture end gap in the three-point bending experiment with two experimental models: (a) the side view of the embracing plate specimen model, (b) the positive view of the embracing plate specimen model, (c) the side view of the pre-shaped anatomical plate specimen model, and (d) the positive view of the pre-shaped anatomical plate specimen model.
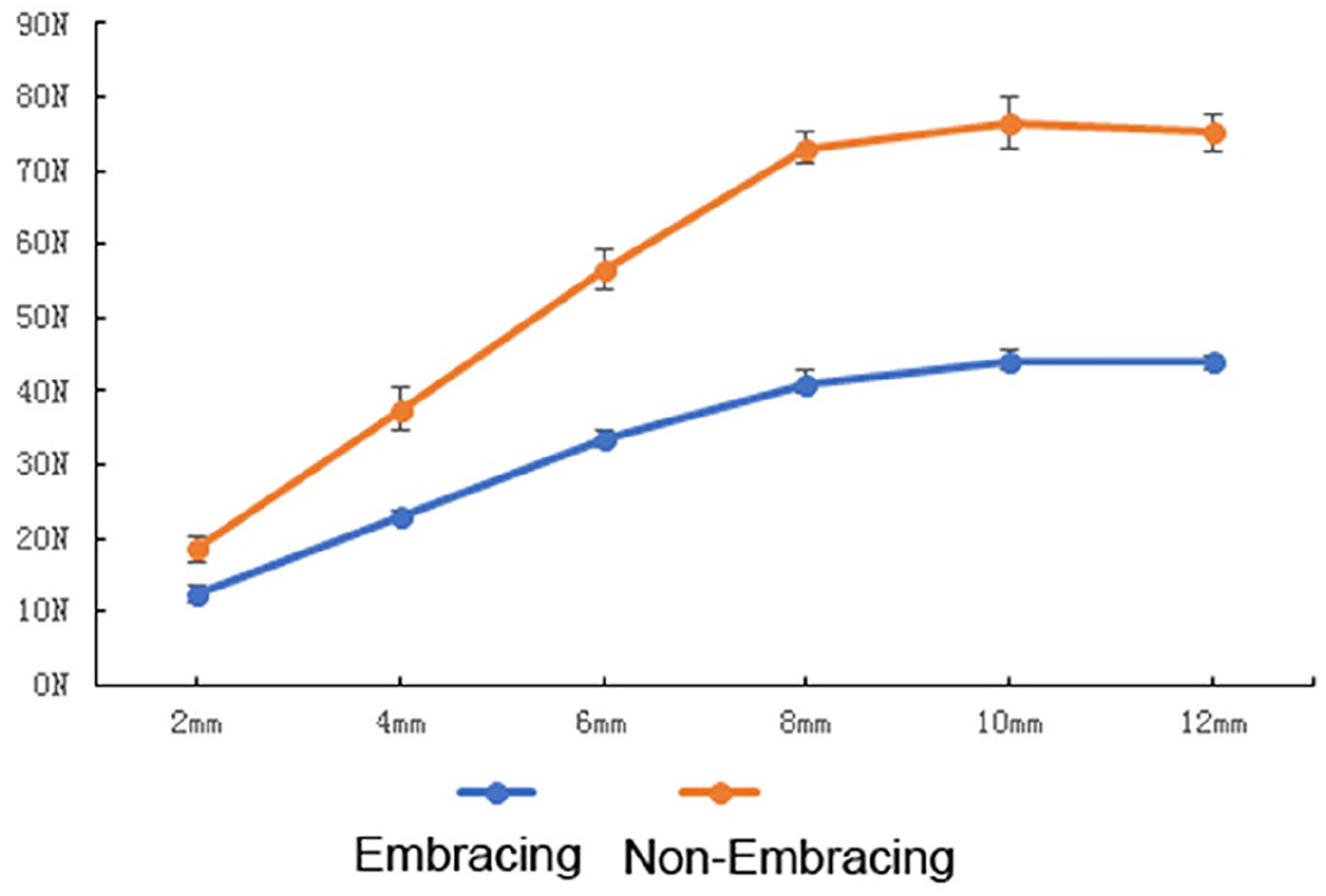
Relationships between displacement and load in three-point bending test with two experimental models.
Nondestructive torsion experiment results
Results in Figure 5 provided the evidence that the torque required for the two sets of specimens was increased along with an elevated torsional angle, but there was no statistical difference (p > 0.05). The graph also showed that the required torque of the embracing plate was generally higher than that of the pre-shaped plate before reaching 25°. The torque of the embracing plate was significantly reduced at 30°. However, the torque of the pre-shaped plate continuously rose. In addition, there was no significant difference in the loading torque of six angles of rotation (p = 0.082).

Relationships between angle and torque in torsion experiment with two experimental models.
Destructive axial compression test
Results in Figure 6 showed the rib fracture morphology details of the two groups. The results indicated that the damage point of the pre-shaped plate was mostly the new bone fracture around the locking screw. Meanwhile, the damage point of the embracing plate occurred in most parts of the surrounding claw. No displacement or deformation of the original fracture was observed in either group. The load required for axial compression of the two groups was 173.88 ± 5.85 N (the embracing plate) and 220.87 ± 42.26 N (the anatomical plate), respectively. The mean load value of the anatomical plate was significantly higher than that of embracing plate (p < 0.05), suggesting that the pre-shaped anatomical plate can bear a higher axial load than the embracing plate.

Destructive sites of two groups in destructive axial compression experiment: (a) an embracing plate specimen model and (b) a pre-shaped anatomical plate specimen model.
Discussion
The ribs are the most inevitable structures for co-ordination of activities such as breathing, coughing, and even resuscitation intervention in human. It is well known that the fracture healing characteristics of ribs are different from other bone tissues and they lack protection by physiological load. 10 Therefore, the multiple rib fractures need emergency care with effective stability treatment in order to promote the recovery of normal physiological functions of the ribs. Previous reports proved that the stability and strength of internal fixation are the most important biomechanic factors in clinical application. 11 Rehm placed six anterior ribs (1.5 cm gap) of adult patients with a bridge of a stress gage to test the bending, torsion, and axial stress loading of the ribs under spontaneous breathing. The highest bending stress is 39 N, the highest torsional stress is 18 N, and the highest axial stress is 7 N. 12 Helzel et al. 13 suggested that the rib bending stress of the human body can reach 92.4 N when human is coughing. In this study, the destructive experiments of the two groups showed that the required stress is 173.88 ± 5.85 N and 220.87 ± 42.26 N, respectively. The above parameters have exceeded the upper limit of stress in physiological activities, indicating that both materials can provide stable fixation of the fracture site with sufficient strength. Moreover, the regularity of the morphological destruction of the two models shows that the normal bone tissue at the location of the claw-shaped embracing fit and the locking screw is potentially destructive. This can result in a weak area that is sufficiently resistant to normal physiological stress, such as spontaneous breathing and cough. However, it is still not easy to rule out whether a new fracture in a weak area is developed, when the thorax is subjected to the external force.
Unlike other bone tissues of human body, the ribs have more complex geometric shapes, including the curvature of the two vector directions and the torsion. Meanwhile, the bending, torsion, and axial shear stresses under physiological conditions are more complex. 14 Therefore, evaluating the effectiveness of internal fixation requires consideration of multiple factors. In this study, the three-point bending test demonstrates the higher bending load of each displacement point of the pre-shaped anatomical plate compared to the embracing plate (p < 0.05). Therefore, the pre-shaped anatomical plate looks more reliable in terms of strength. Besides, the annulus plate model produces a 1–2 mm separation of the fracture gap under compression, which is restored toward the end of applying pressure. However, the pre-shaped anatomical plate shows no sign of fracture gap. It is indicated that the pre-shaped anatomical plate has advantages in terms of the absolute stability of the internal fixation. Previous studies have shown that axial micro-motion of fracture ends within a certain range can promote fracture healing. 15 Fracture-healing is a complex process that is modulated by the extent of vascularization at the site of the fracture. 16 Sarmiento and others who have demonstrated that some motion at the fracture cite is not only tolerable, but in fact, necessary, to enhance fracture healing. Therefore, as long as the fracture is fixed with sufficient stability to withstand physiological loading requirements during the healing process, the more flexible construct may be advantageous.17–19 Based on the conclusions mentioned above, the embracing plate seems to have more advantages, but this findings need to be further verified by conducting an in vivo study. The results of the torsion test curve shows that no significant difference can be detected in the torsional properties between the embracing plate and the pre-shaped anatomical plate fixation materials. The destructive axial pressure is related to the shear stress test. The pre-shaped anatomical plate group shows stronger anti-shearing ability than that of the embracing plate (p < 0.05).
At present, the widely accepted Arbeitsgemeinschaft fur Osteosythesefragen (AO) principle of fracture treatment revealed that the protection of blood supply cannot be ignored except for anatomical reduction and stable and firm fracture fixation. 20 The advantage of a memory alloy embracing device is that it can be fixed immediately and firmly and is relatively cheap. Meanwhile, other advantages include good biocompatibility, conformity to the physiological curvature of the rib along with the ability to completely attach to the rib surface, fix on the rib surface without removing the periosteum, avoid injury to the vascular nerve bundles at the lower edge of the rib, fix the fracture ends with sufficient length, and match the internal threads between bone fracture plates. 21 The disadvantage is that it inevitably destroys the blood supply of ribs and damages blood vessels and nerves, leading to poor bone healing and chest pain due to intercostal nerve entrapment or tight sensation at the internal fixation. 21 In this situation, screws cannot be easily prolapsed and the facility of displacing the implant after locking. The disadvantage is that the operation requires sufficient operating space. The angle of the screw and bone fracture plate should be maintained at 90°, otherwise, the screw may come out. 22 To avoid the intercostal neurovascular bundle damage at the lower edge of the rib, it is often necessary to free the periosteum at the lower edge of the rib during the embracing rib plate implantation. The pre-shaped anatomical plate does not require free periosteum. Therefore, a pre-shaped anatomical plate has certain advantages in terms of blood supply protection. However, the embracing panels are cheaper and more advantageous in terms of economic costs.
There are several limitations in this study. First, the sample size is limited. Second, we have conducted three-point bending tests; however, a four-point bending test may have been preferable, as it would have avoided contact between the test apparatus and the construct at the point of fracture. Third, this study was only done in vitro, and an in vivo study needs to be conducted to further verify this finding.
Conclusion
In summary, with the increasing recognition of internal fixation for rib fractures by thoracic surgery and traumatology surgeries, more and more internal fixation methods have been tested and applied in the clinic. For different fracture types and actual clinical needs, internal fixation materials with corresponding characteristics can be selected. This experiment preliminarily explored the biomechanical properties of the embracing and non-embracing fixation materials, which may provide a theoretical basis for scientists and engineers in field of surface morpho-logy and biodesign of metals with potential biomedical applications.
Footnotes
Author contributions
GH carried out the study concepts, study design, literature research, data acquisition, data analysis, statistical analysis, and manuscript preparation; JY was dedicated to the guarantor of integrity of the entire study, definition of intellectual content, clinical studies, manuscript editing, and manuscript review; GH, PL, and GL were involved in the experimental studies. All authors declare that they have read and approved this article.
Data availability statement
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the key research program of Hebei Provincial Health Department (No.20120333) and Hebei provincial government funded the training project of clinical medicine talents.