
Abstract
Background
Femoral material harvested using the Reamer-Irrigator-Aspirator (RIA) system is an alternative source for autogenous bone material in the treatment of non-unions, especially in combination with bone morphogenetic proteins (BMP). So far, there is no in vivo evidence of BMP-7 interacting with mesenchymal stem cells (MSCs) from RIA material (RIA-MSCs) and iliac crest autogenous bone (BMSCs). The aim of this study was to compare their osteogenic potential when stimulated with BMP-7 in vivo.
Methods
RIA-MSC and BMSC from 11 donors were isolated and the character of MSCs was investigated in vitro. Constructs consisting of MSC, β-tricalcium phosphate and 2 concentrations of BMP-7 (0.1 µg/mL and 1 µg/mL) were implanted in mice for 8 weeks. Bone formation in the constructs was analyzed quantitatively and qualitatively.
Results
All cell populations used were determined to be MSCs. The qualitative in vivo analysis showed formation of bone tissue. With regard to quantity, bone formation was significantly higher in RIA constructs without or with stimulation with 0.1 µg/mL BMP-7, compared with BMSC constructs. We found no significant differences between constructs stimulated with 1 µg/mL BMP-7. In the RIA group, we observed a significant increase in bone formation after stimulation with 0.1 µg/mL BMP-7. No significant change could be found using a higher concentration. In the BMSC group, we detected a significant increase when using 0.1 µg/mL and 1 µg/mL BMP-7.
Conclusions
RIA material is a source of MSCs with high osteogenic potential. Our results showed that stimulation by BMP-7 leads to an increased osteogenic potential of MSCs. In this respect, RIA-MSCs reacted more sensitively than BMSCs.
Keywords
Introduction
Bone fractures are the most common consequences of trauma. During the healing process, failure to consolidate and the development of non-unions occurs in 5%-10% of cases; in high-risk groups, the rate is as high as 30% (1). Consequently, there are high costs for medical treatment, unemployment and rehabilitation. Therefore, the development, establishment and evaluation of new therapeutic options belong to the most significant areas of research in trauma surgery (1, 2).
The “diamond concept” describes essential therapeutic elements, including a cell population capable of osteogenic differentiation and growth factors (3, 4). In terms of cell harvesting for the therapy of non-unions, the gold standard is an autogenous bone graft from the iliac crest, containing mesenchymal stem cells (MSCs; bone marrow MSCs or, specifically, MSCs from iliac crest autogenous bone [BMSCs]) (5). However, the disadvantages of these are their limited availability, great individual differences in biological activity and often extensive donor site morbidity (5, 6). As a result, reaming material from the femur is used with increasing demand as a source of osteoinductive material (7), which is rich in MSCs (Reamer-Irrigator-Aspirator [RIA]-MSCs), osteoprogenitor cells and growth factors. This seems to be a comparable alternative to the gold standard (8–9–10–11).
The clinical results of non-union therapy are still in need of improvement; for this reason, biological growth factors such as bone morphogenetic proteins (BMPs) are increasingly more common as a therapeutic option (2, 5, 12–13–14). BMPs belong to the transforming growth factor β (TGF-β) family, conducting their osteoinductive effects mainly via the Smad signaling pathway (15). The application of synthetically produced recombinant human BMP-7 (rhBMP-7) is licensed for use in non-unions of the tibia (2, 16, 17). The combination with autogenous bone grafts results in improved local adhesion and cellular environment as well as higher rates of consolidation (5, 18), yet so far there are no in vivo investigations concerning the interaction of BMPs with either RIA-MSCs or BMSCs (13).
Our study focused on the comparison of human RIA-MSCs and BMSCs in vivo, their osteogenic potential and their response to stimulation with 2 concentrations of BMP-7 in an ectopic animal model.
Material and methods
Patients
Reaming material from the femur and aspirate from the iliac crest were obtained from 11 patients between 2012 and 2013. The reaming material was harvested using the Reamer-Irrigator-Aspirator (RIA) system (Synthes Inc., West Chester, PA, USA) (7). Consent was granted by all patients and by the ethics committee of the Ruprecht-Karls University Heidelberg (reference number S-355/2010). The patient collective cohort consisted of 4 males and 7 females, with mean age of 55.5 years (range 20-79 years). To improve the transferability to clinical situations, we did not match the donor collective cohort based on comorbidities and possible risk factors for non-unions (4, 19).
Isolation and cultivation of MSCs
The isolation and cultivation of MSCs from iliac crest aspirate was performed following established protocols published previously (11, 20). RIA material was transferred into a sterile petri dish, washed in phosphate buffered saline (PBS; PAA, Pasching, Austria), and 0.8-1.2 g was seeded in a gelatin-coated flask containing embryonic stroma cell (ES) medium and cultivated as described before (11). The following list are the components of ES medium: Dulbecco's modified Eagle's medium (DMEM) high glucose supplemented with 12.5% fetal calf serum (FCS), 2 mM L-glutamine, 1% nonessential amino acids, 50 μM β-mercaptoethanol (all Lifetechnologies, Darmstadt, Germany), 100 units/mL penicillin, 100 μg/mL streptomycin and 4 ng/mL basic fibroblast growth factor (bFGF) (Active Bioscience, Hamburg, Germany). The solid tissue was removed after 10 days.
Initially, the cells were stored in liquid nitrogen using freezing medium, containing 50% ES medium, 40% FCS and 1% dimethyl sulfoxide (Sigma-Aldrich, Steinheim, Germany). After thawing, the cells were cultivated and used in passage 2.
Flow cytometry
Surface antigens from all cell populations were characterized using fluorescence-labeled antibodies. 200,000 cells were resuspended in 100 µL MACS Auto Buffer (Miltenyi Biotec GmbH, Bergisch Gladbach, Germany). Subsequently, they were incubated with 5 µL of the following antibodies (10 minutes, 4°C): CD90-FITC, CD73-APC, CD105-PerCP-Cy5.5, CD34-PE and CD45-Vioblue (BD Biosciences GmbH, Heidelberg, Germany). Further, we performed control stainings without any antibodies and with 5 µL mouse anti-human IgG2 kappa (Thermo Scientific, Roskilde, Denmark) to exclude nonspecific binding of the antibodies used. The cells were analyzed by MACS Quant™ Analyser (Miltenyi Biotec GmbH, Bergisch Gladbach, Germany).
Trilineage differentiation in vitro
The potential for trilineage differentiation of the cell populations used was analyzed with induction and proof of adipogenic (oil red O staining), chondrogenic (Safranin O/Fast Green staining) and osteogenic (alizarin red S staining, activity of alkaline phosphatase [ALP] activity, analyzed after 1 and 21 days) differentiation as published before (11).
Production of β-tricalcium phosphate constructs
To analyze the osteogenic potential of MSCs in vivo, constructs colonized with MSCs were fabricated and implanted for 8 weeks subcutaneously in immunodeficient mice as published before (11, 20). Two constructs of each tissue source were created without BMP-7, 2 with 0.1 µg/mL BMP-7 (Olympus Biotech Europe, Lyon, France) and 2 with 1 µg/mL BMP-7. Furthermore there were controls without any MSC seeding. β-Tricalcium phosphate (β-TCP) granulate (10 mg; RMS Foundation, Bettlach, Switzerland) with a granulate size of 0.5-0.7 mm and a porosity of 60% (20) were transferred into a 1.5-mL tube and mixed with 1 × 106 cells and BMP-7 (dissolved in 2 µL sterile distilled water) when indicated. Afterwards 20 µL of fibrin/thrombin-tissue glue (Baxter Deutschland GmbH, Unterschleißheim, Germany) was added to form a stable construct (approximately 3 mm3).
Surgical Procedure
Female severe combined immunodeficiency (SCID; CB17/Icr-Prkdcscid/Crl) mice were used as hosts to reduce the risk of rejection. Consent was given by the animal welfare committee (9185.81/G-251/12). The procedure complied with European Laboratory Animal Science Guidelines.
The mice were anaesthetized using medetomidine/ketamine, and 4 constructs per mouse were implanted subcutaneously into paravertebral pouches (2 each above shoulders and hips). After 8 weeks, the mice were euthanized by cervical dislocation and constructs were explanted from the subcutaneous pouches (11). All efforts were made to reduce suffering of the animals.
Histological analysis
The explanted constructs were prepared for histological analysis as described previously (11). Hematoxylin-eosin (HE) staining was performed for quantification of bone formation following established protocols (11), and for qualitative analysis, hematoxylin-eosin-saffron (HES), Safranin O/Fast Green and immunohistochemical anti-BMP-7 staining were done.
Safranin O/Fast Green staining
Slides were stained in Safranin O for 20 minutes and in Fast Green for 20 seconds.
HES staining
in addition to the hematoxylin staining, the slides were acidified and incubated for 4 minutes in alcoholic eosin (2%). After washing the slides in 100% isopropanol, they were stained for 2 minutes in alcoholic Masson's saffron (Waldeck GmbH, Münster, Germany).
Immunohistochemical anti-BMP-7 staining
After the usual preparations, the peroxidase activity in the constructs was inhibited using peroxidase blocking solution (5 minutes). The slides were incubated with a BMP-7 antibody (sc-9305; Santa Cruz Biotechnology, Heidelberg) for 12 hours at 4°C. A secondary antibody conjugated with biotin was added for 30 minutes. Then, avidin-biotin complexes loaded with horseradish peroxidase were admixed, which were able to bind to biotin of the secondary antibodies. After several washing steps, diaminobenzidine was added, which was oxidated by the peroxidase and consequently developed a reddish color.
Histomorphometry
HE-stained slides were photographed under a microscope, and the total area of the construct and the area of new bone were marked in 2 different colors using Adobe Photoshop (Adobe Systems Inc., USA). Using Image J (National Institutes of Health, Bethesda, MD, USA) the percentage of the bone was calculated and referred to the total area of the construct (11, 20).
Statistical Analysis
Statistical analysis was performed with SPSS 21.0 (IBM Corp., Chicago, IL, USA) using the Friedman and Wilcoxon tests (nonparametric tests) for the in vivo results. The in vitro results were analyzed by the t-test. A p value <0.05 was considered significant.
Results
Characterization of surface antigens
All cell populations used in the study showed positive expression patterns for the antigens CD73, CD90 and CD105 – i.e., >95% expressed these antigens on their cell surface. Less than 2% of the cells expressed CD45 and CD34, and these were consequently labeled as negative.
Trilineage differentiation in vitro
Adipogenic differentiation
All cell populations used in this study were capable of adipogenic differentiation. The oil red O staining showed orange lipid vacuoles. The amount of bound oil red O was measured to estimate the lipid concentration. The mean concentration of oil red O was 0.47 µg/mL for the cells from RIA material and 0.49 µg/mL for cells of the iliac crest. There was no statistically significant difference (Fig. 1).
Oil red O staining of cell layers from a representative donor, stained on day 14: (
Chondrogenic differentiation
The chondrogenic differentiation was shown with Safranin O/Fast Green staining. Safranin O binds glycosaminoglycans, which are essential components of cartilage tissue (Fig. 2). All cells from RIA material were able to differentiate; in the iliac crest group, differentiation could be observed in 10 of 11 donors.
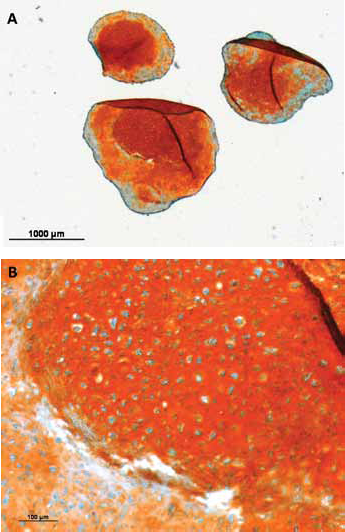
Safranin O/Fast Green staining of chondrogenic spheroids: representative staining of chondrogenic spheroids from cells of one donor (magnification A: ×1.25, B: ×10). Safranin O stains sour glycosaminoglycans orange-red in cartilage tissue. Stained glycosaminoglycans were visible in spheroids from both mesenchymal stem cells from Reamer-Irrigator-Aspirator material (RIA-MSCs) and MSCs from iliac crest autogenous bone (BMSCs), and in consequence, the formation of cartilage tissue could be assumed for both tissue sources.
Osteogenic differentiation
In the analysis of all cell populations used, we observed significant increases of ALP activity (in relation to total protein concentration) and extracellular calcium deposits over the observation period of 21 days (Fig. 3). The difference between ALP activity of RIA-MSCs and BMSCs was merely significant on day 1 (RIA-MSC: 0.06 mL/min; BMSC: 0.03 mL/min; p = 0.033). Concerning the extracellular calcium, the differences between the 2 groups were not significant at any point of measurement.
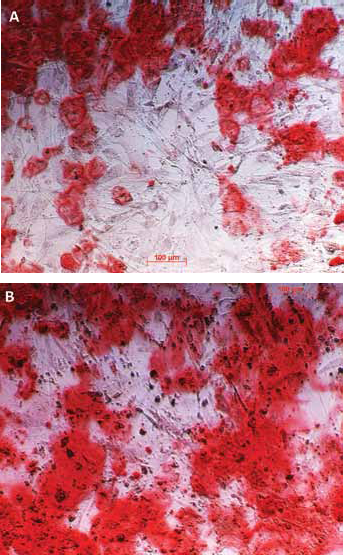
Alizarin red S staining: of cell layers of mesenchymal stem cells (MSCs) for osteogenic differentiation on day 21: (
Osteogenic differentiation in vivo
Generation of new tissue
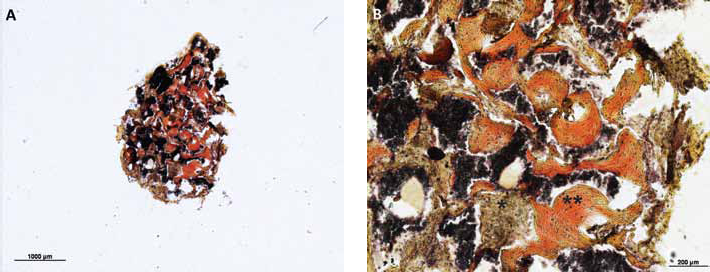
HES staining allowed the differentiation between hard tissue (bone or cartilage tissue, red) and soft fibrous tissue (brown). In the histological slides of the control constructs without MSCs, we could only detect β-TCP and fibrous soft tissue (Fig. 4). In the constructs seeded with MSCs from all 11 donors, we observed the generation of hard tissue (Fig. 5).
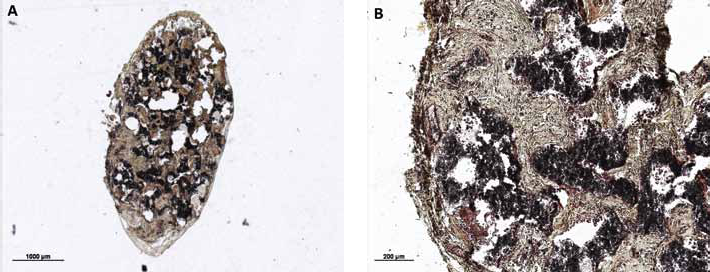
Control constructs (hematoxylin-eosin-saffron [HES] staining) produced without mesenchymal stem cells (MSCs); histological analysis showed only β-tricalcium phosphate (β-TCP; black) and fibrous tissue (brown) (magnification A: ×1.25 and B: ×5). Thus, no hard tissue was generated in the constructs in the absence of MSCs.
(
Safranin O/Fast Green staining
This staining was performed for further analysis of the hard tissue to differentiate between bone and cartilage. In the histological slides of our constructs, we only detected tissue, which was stained by Fast Green. The newly generated tissue did not contain glycosaminoglycans, which would have been stained orange-red by Safranin O (Fig. 6).
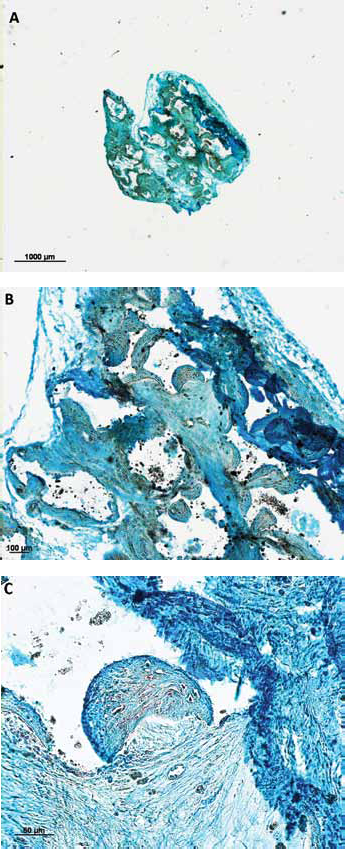
Safranin O/Fast Green staining of representative construct: no orange-red tissue cartilage tissue could be detected (magnification A: ×1.25, B: ×5, C: ×20). In conclusion, it could be assumed that there was no cartilage formation in the constructs.
Immunohistochemical anti-BMP-7 staining
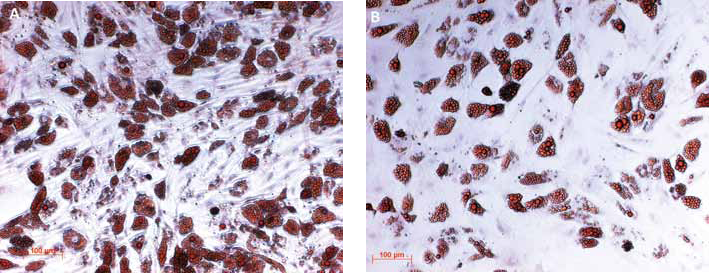
The staining was performed on slides of representative donors. Existence of BMP-7 (indicated by red staining) was detected in MSC-seeded constructs after explantation. High concentrations showed in the fibrous tissue surrounding the newly formed hard tissue and in the fringes of the same (Fig. 7).

Immunohistochemical anti-BMP-7 staining (×5). BMP-7 (detected by red staining) is shown in high concentration in fibrous tissue surrounding the newly formed hard tissue. Red staining is also detected in border areas of the hard tissue while the centers of the same showed no stained BMP-7.
Quantitative comparison of osteogenic potential in vivo
First, the osteogenic potential of MSCs without stimulation was compared between groups. Regarding RIA constructs, the percentage of newly formed tissue in relation to the complete area reached mean percentages of 5.06%, which was significantly higher than in the BMSC group (RIA-MSC: 5.06%; BMSC: 2.57%; p = 0.015) (Fig. 8A).
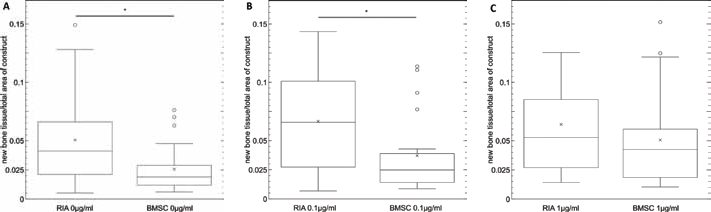
Comparison of osteogenic potential in vivo. The tissue source is plotted on the x-axis, while y-axis shows percentage of new bone tissue. Differences were statistically significant in the group without stimulation (
RIA constructs stimulated by BMP-7 at a low concentration showed an average percentage of newly formed tissue of 6.65%. In the BMSC group, the mean value was 3.71%, significantly lower compared with the RIA group (*p = 0.009) (Fig. 8B). Regarding the constructs stimulated with 1 µg/mL BMP-7, the difference in the mean values was not statistically significant (RIA-MSC: 6.39%; BMSC: 5.06%; p = 0.394) (Fig. 8C).
Further, we analyzed the differences in osteogenic potential within 1 MSC group (RIA-MSC and BMSC) after stimulation by BMP-7 (Fig. 9). The mean percentage of bone tissue in the RIA group increased significantly when stimulated by 0.1 µg/mL BMP-7 (+1.59%; p = 0.049). In comparing the values of constructs with 0.1 µg/mL BMP-7 and 1 µg/mL BMP-7, no significant differences were found (-0.26%; p = 0.639). The constructs with 1 µg/mL BMP-7 showed no significantly higher values than constructs without simulation (+1.33%; p = 0.106). In the BMSC group, the values increased after stimulation by 0.1 µg/mL BMP-7 (+1.14%; p = 0.031). The increase between constructs with 0.1 µg/mL and 1 µg/mL BMP-7 was not statistically significant (+1.35%; p = 0.205). Comparing constructs without BMP-7 and with 1 µg/mL BMP-7, we observed in the latter significantly higher values (+2.49%; p = 0.012).
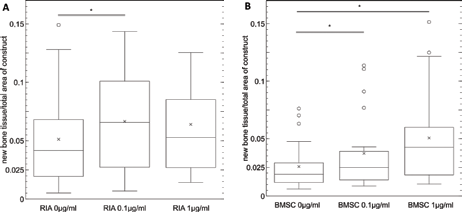
Influence of BMP-7 on osteogenic potential. Comparison of mean values of (
Discussion
The aim of this study was to compare the osteogenic potential of RIA-MSCs and BMSCs as well as their response to stimulation by BMP-7, to evaluate new approaches for treating non-unions. Strengths of the study were firstly the use of human MSCs and the comparison of cells from tissue sources of one and the same donor. Secondly the potential of the cells was analyzed in an in vivo study, whereas the majority of previous results have been only in vitro. A weakness was the limited transferability of animal models to therapy of human patients.
Characterization of the studied cell population
In 2006, the International Society of Cellular Therapy (ISCT) published criteria necessary to define a cell population as MSCs (21). Previous studies have already described the successful isolation of cells that meet MSC criteria from iliac crest aspirate and RIA material by using the isolation and cultivation methods described in our study (11).
The cells used in this study fulfilled the criteria of plastic adherence as it was a requirement for successful isolation and cultivation. For cells from both tissue sources, the required expression pattern of surface antigens could be shown. Moreover, trilineage differentiation could be observed in vitro. The cells of all donors and both tissue sources showed the ability for adipogenic differentiation. Regarding the amount of generated lipid, no difference between the 2 cell groups could be found, confirming the results of previous in vitro investigations (11). In the chondrogenic induction medium, both RIA-MSCs and BMSCs formed 3-dimensional spheroids with cores of cartilage tissue; the medium for RIA-MSC contained BMP-6, which was proven to be necessary for the chondrogenic differentiation of these cells (11). Osteogenic differentiation could be proven for all cells by analyzing ALP activity and the amount of extracellular calcium. There were no significant differences between the parameters of the 2 cell groups, which was also consistent with previous results (11). Consequently, the cells isolated from reaming material and iliac crest aspirate could both be characterized as MSCs.
Analysis of the newly formed tissue
As a carrier for MSCs in this study, β-TCP granulate with a diameter of 0.5-0.7 mm was used. The successful osteogenic differentiation of MSCs and formation of new bone tissue with this carrier system has already been shown in multiple studies (11, 22). Qualitative stainings showed that hard tissue was generated in the constructs that could clearly be differentiated from surrounding fibrous tissue in HES-stained slides. The Safranin O/Fast Green staining helped to exclude the formation of cartilage tissue, as the correlates to the hard tissue from HES staining did not contain glycosaminoglycans. In conclusion, the formation of bone tissue could be assumed. Additionally, we detected the expression of BMP-7 in the fibrous tissue and in border areas of the hard tissue in explanted constructs. Former studies have shown that the expression of BMP-7 increases in tissues undergoing osteogenic differentiation (23). The concentration in differentiated bone tissue, however, is low, as it can also be observed in the central areas of the newly formed hard tissue in our constructs.
A possibility for further analysis of the newly generated tissue would be gene analysis of cells extracted from the explanted constructs. Further studies should be conducted on this basis.
Comparison of osteogenetic potential in vivo
Clinically, the use of RIA material has certain advantages compared with iliac crest autografts: Significantly higher volumes can be harvested with the RIA system (24), furthermore the rate of donor side complications is lower (25) and the harvesting can be repeated after several months (26).
Our results showed that in the nonstimulated groups, the percentage of new bone was significantly higher in the RIA group with a mean value of 5.06% compared to 2.57% in the BMSC group. Results of previous studies indicated that RIA material is an alternative source for MSCs and that its use is at least equal to the gold standard in non-union therapy (8, 11).
Influence of BMP-7 on osteogenic potential of MSCs in vivo
Our results demonstrated the increase in the osteogenic potential of MSCs in vivo through stimulation by BMP-7, concerning both RIA-MSCs and BMSCs. The osteoinductive effect of therapeutic BMP-7 has already been shown in vitro in the admission study (16) and was confirmed by numerous other studies (2, 5, 12, 17). In a recent study, Moghaddam et al (13) analyzed cytokine expression patterns of non-union patients compared with patients with successful fracture healing and non-union patients treated with BMP-7. Results indicated that BMP-7 induces an expression of cytokines, which are associated with fracture healing (TGF-β, PDGF, bFGF) (27), similar to expression patterns of patients with successful fracture healing, whereas non-union patients showed a significantly different expression (13).
With regard to autogenous bone from the iliac crest, it has been documented that the combination of BMP-7 with autogenous bone leads to higher success rates in non-union treatment (18). The combination of BMP-7 with MSCs from reaming material has so far not been investigated in vivo.
The addition of high concentrations of BMP-7 had a stimulating effect on the osteogenic potential of MSCs from both tissue sources without a significant difference between the RIA and the BMSC group. After stimulation using a lower concentration of BMP-7, we observed a more pronounced effect of the growth factor on constructs colonized with RIA-MSCs, suggesting that RIA-MSCs react more sensitively to BMP-7 compared with BMSCs.
An alternative source of growth factors for clinical use is platelet-rich plasma (PRP) (3, 28). PRP can be produced in a simple centrifugation procedure from the patient's own blood and contains thrombocytes at a high concentration. These thrombocytes produce cytokines and growth factors, which are released from their granules after cell activation (29). Furthermore, PRP is produced from the patient's own blood and therefore has no incompatibility issues and could be an alternative to the use of rhBMP-7; for example, in combination with an autogenous bone graft (30), especially as it contains a combination of various growth factors (e.g., TGF-β1, PDGF, VEGF, IGF-1) (9). The application of multiple growth factors might be advantageous; however, the yield of growth factors in PRP is low compared with autogenous bone or reaming material (9), and the clinical success rates are variable (31, 32). This is most likely due to the individual constitution of the patient – e.g., chronic diseases, hematological conditions and recent blood loss.
Considering the high costs of a therapy with rhBMP-7, which is currently not available for clinical use, and the risk of heterotopic ossifications especially when high dosages are used (33), the alternative application of PRP has become even more interesting. The results of our study indicate that RIA-MSCs respond already to lower concentrations of BMP-7, and therefore especially the combination of PRP with RIA material could lead to successes in non-union therapy.
So far, there have been no studies concerning the comparison of BMP-7 with other clinically used differentiation factors such as BMP-2 and insulin-like growth factor-1 (IGF-1). Like BMP-7, BMP-2 is processed during physiological fracture healing (34) and has a positive effect in clinical applications as described (35). The essential role of IGF-1 in bone metabolism and its stimulating effect on fracture healing have been shown as well (36).
Scaffold materials are one other central part of the diamond concept. So far, there is no in vivo evidence about interference from multiple scaffold materials concerning the interaction of cells, scaffold surface and differentiation factors. While β-TCP shows limited osteoinductive capabilities, new materials such as bioactive glasses seem to be superior in terms of osteoinductivity. A combination of differentiation factors and osteostimulative scaffold materials could further improve therapeutical outcomes in non-union treatment (37).
Furthermore, there have been no in vivo investigations yet concerning the process of bone formation by MSCs. As demonstrated in a recent study, micro-CT analysis is a reliable alternative to histological evaluation that could make it possible to observe the development of new bone tissue in a living animal model (20).
In conclusion, the results of our study showed that MSCs from reaming material are superior compared with BMSCs with regard to osteogenic potential in vivo. Moreover, RIA-MSCs respond more sensitively to stimulation by BMP-7, and for that reason they could lead to successful treatment in combination with the patient's own PRP. Further experimental and clinical studies should be planned and conducted to investigate these approaches.
Footnotes
Acknowledgement
The authors thank RMS Foundation in Bettlach, Switzerland, for providing the β-tricalcium phosphate, and Olympus Biotech Europe, Lyon, France, for providing BMP-7. Furthermore they thank Christopher Child from the Heidelberg Trauma Research Group (Department for Trauma Surgery, University of Heidelberg) for his support in statistical analyses, as well as Tyler Swing for linguistic support.
Financial support: No grants or funding have been received for this study.
Conflict of interest: The authors declare they have no conflicts of interest.