
Abstract
Background
Metallic ball heads for total hip replacement (THR) bearings with ceramicized surfaces were introduced in orthopedics during the second half of the 1980s, with the aim of decreasing the wear of polyethylene cups.
Methods
An analysis was made of the literature regarding outcomes for metallic ball heads with ceramicized surfaces now in clinical use (TiN, TiNbN, ZrN, monoclinic ZrO2), as well as carbon coatings (pyrolytic carbon, diamond-like carbon) and silicon nitride as coatings in ball heads for THR bearings.
Results
Notwithstanding the diffusion of ceramicized ball heads in THRs, there are few reports about their clinical outcomes in hip arthroplasty. In addition, several clinical studies and some registry data are putting under scrutiny the clinical advantages of ceramicized ball heads over cobalt chrome (CoCr) alloy and ceramic ball heads.
Conclusions
The wear of THR bearings with ceramicized ball heads looks like it depends more on the behavior of the polyethylene cups than on the treatment of the ball head surface. The risk of coating damage and of its consequences has to be taken into account in selecting this type of bearing.
Introduction
After the practical abandonment of metal-on-metal bearings in hip arthroplasty, 3 main bearing options are available today for total hip replacement (THR): ceramic-on-ceramic (CoC), ceramic-on-polyethylene (CoP) and metal-on-polyethylene (MoP) bearings. Although there is evidence for the excellent reliability and clinical wear behavior of the present generation of CoC and of CoP THR bearings (1–2–3–4), polyethylene acetabular components coupled to metallic ball heads (MoP) are the bearing used in a number of patients. Several developments have been implemented to improve the wear behavior of these hard-on-soft bearings. On the acetabular side, several successive generations of cross-linked polyethylenes (XLPEs) have been developed (5), doped by the antioxidant alpha-tocopherol in the latest generations (VitE-XLPE) (6). On the ball head side, the surface of the metallic head has been improved by applying ceramic coatings.
The development of ceramicized ball heads can be traced back to the 1980s. Besides the advantage in bearing wear due to the increase in hardness and in scratch resistance of the metallic surface, this technique was applied in arthroplasty to overcome the problems posed at that time by the brittle fractures of alumina ceramic heads, an issue now outdated because of the introduction of tough alumina-zirconia composites (e.g., ZTA, ATZ, AMC) (7). Moreover, the coating applied to the metallic implant allows the protection of hypersensitive patients from the metal ions that are released by orthopedic alloys (8–9–10).
The aim of this work was to review the outcomes for ceramicized ball heads in clinical settings. We analyzed the literature in the Pubmed database reporting clinical results of hip replacements with ceramicized ball heads. Consequently, this review encompassed not only the nitrogen-based coatings that are the ones more widespread in hip replacement bearings, but also the nonnitrides used as coatings, such as diamond-like carbon (DLC) and monoclinic zirconium dioxide (ZrO2).
Nitride coatings
Nitrogen has long been used to improve the hardness of metals. In orthopedics, the first mention made was to a patent assigned to Steinmenan in 1972 (11) referring to a nitride layer to prevent corrosion and fretting of titanium alloy implants. Further reports of early studies on titanium nitride (TiN) were published in the second half of the 1980s (12–13–14–15). Several studies were carried out investigating the feasibility of TiN coatings by ion implantation, as reported by, e.g., Boampong et al (16). This technology has been abandoned in favor of physical vapor deposition (PVD) which is today the standard technology to obtain TiN and titanium niobium nitride (TiNbN) coatings (17–18–19).
Whatever the process used, it is necessary to control the effects of the residual stresses in the coating, which depends on the deposition process parameters, such as reaction with the environment, presence of impurities, rate of formation and angle of deposition. Such stresses may reach the level of several gigapascals (20) and – if tensile – may lead to the spallation of the surface layer under appropriate conditions due to the relatively low coating adhesion to the substrate. It is then relevant that residual stresses are compressive to avoid the delamination of the surface scale. Increase in temperature during coating deposition, which leads to some diffusion bonding, or the deposition of several layers with graded behavior (a multilayer approach), has proven effective in improving the coating characteristics (21). These coatings are made of several layers, the first one having a chemical composition similar to that of the substrate, while the composition of the successive layers is selected to grade the transition in elastic properties between the “soft” base metal and the hard surface layer. It is noted that a further reason for coating failure is corrosion through local defects (i.e., micro-droplets, pinholes or other point defects) that are inherent to the PVD process (22, 23). Because of the random distribution of defects in each layer, multilayer coatings may be preventive of the corrosion of the substrate (24).
The hard surface also provides protection from wear due to third bodies – e.g., polymeric or cement debris – and the improved surface scratch resistance prevents implant damage (25–26–27). A further advantage of the ceramicized surface is the better wettability compared with bare CoCr. In this way, the lubrication is improved while decreasing the coefficient of friction and wear (27). In hip simulator studies, ultra high molecular weigth polyethylene (UHMWPE) cups have been shown to undergo up to 98% less wear against TiN ceramicized heads than against CoCr heads (28).
Titanium nitride: clinical results in THR bearings
TiN coatings are applied to hip, knee, ankle and shoulder replacements, but in spite of their extensive use, little exists in the literature concerning their clinical outcomes. Notwithstanding that TiN has long been in clinical use, there are only a few reports about the clinical outcomes for these bearings in total hip arthroplasty. The comprehensive review of TiN coatings by van Hove et al (29) reports only 7 clinical studies on TiN-coated implants since 1992, (2 on ankle replacements, 2 on THR, 2 on total knee replacements (TKR), and 1 on hip resurfacing). Sparse reports are putting in question the damage resistance of TiN coatings in clinical applications (30). The analysis of retrieved THR heads (31) shows extensive abrasion of the coating: in the case of a high-demand patient, the damage was extended to about 70% of the articulating surface.
The first clinical study of TiN in THR was by Massoud et al (32), who reviewed a cohort of 76 patients who underwent hip arthroplasty using the Capital THR. This implant – now withdrawn from clinical use – was a modification of the Charnley low friction arthroplasty. TiN-coated ball heads were used in 16 implants, while the remaining 60 received CoCr-alloy heads, all coupled with UHMWPE cups. At a mean 26 months of follow-up (range 10-37 months), 44% of the stems with TiN-coated heads were loose, while loosening was observed in 21.5% of the stems with a CoCr-alloy ball head.
Buechel et al (33) reported the clinical results for 130 consecutive hip arthroplasties performed in 11,777 patients from 1990 to 1999. All of the implants were cementless devices with the femoral head made of titanium alloy coated with a polished 6- to 10-µm-thick layer of TiN applied by the PVD process. Survivorship of the implants was 95.5% at 11.2 years. The analysis was carried out using as endpoints: (a) revision of any implant component for any reason, (b) clinically poor hip score, (c) radiographic evidence of failure (radiolucency >2 mm in all zones surrounding an implant) or (d) gross implant migration. Although radiolucent lines were observed in Gruen zones 1 to 14, there was no osteolysis around acetabular or femoral components of the implants. One patient showed asymptomatic femoral stem subsidence, and one acetabular component was revised for reported loosening.
Less favorable results were reported by Barouk et al (34), who investigated a series of 52 titanium alloy ball heads, TiN coated by ion implantation. Thirteen prostheses were revised for aseptic loosening, while revision for the same reason was needed for only one in the 118 prostheses making use of different types of ball heads (stainless steel, chromium-cobalt, alumina or zirconia). Besides aseptic loosening, the implants with TiN-coated ball heads showed a high incidence of polyethylene wear, metallosis and modifications of the head surface (disappearance of the coating, scratch marks etc.). Table I summarizes the clinical results of TiN coatings reported in the literature thus far.
Clinical reports of the outcomes of THRs with titanium nitride–coated ball heads
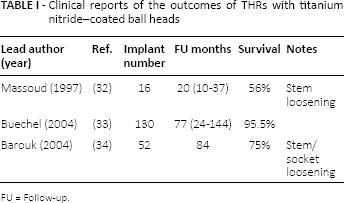
FU = Follow-up.
Other nitride coatings in THR bearings
Zirconium and chromium nitrides
Extensive hip simulator studies were completed for chromium nitride (CrN) and chromium carbon nitride (CrCN)–coated THR bearings (35), but these devices were not introduced into clinical use.
Wear simulator tests performed on a unicompartmental knee implant with zirconium nitride (ZrN) surface were reported by Affatato et al (36). The coating of this device was obtained under nitrogen atmosphere by a proprietary PVD process making use of a series of sputtering targets. The result was a coating formed by a thin Cr bond layer, 5 layers of CrN–CrCN and a final layer of ZrN, with total thickness between 3.5 and 5 μm. The aim of the gradient layers of CrN–CrCN is to bridge the high difference in hardness and stiffness between the mild CoCrMo substrate and the final ZrN coating, assuring in this way the mechanical integrity of the coating system. In addition, this system forms a barrier for ion diffusion from the substrate to the surrounding tissue (37). ZrN is used clinically in at least 1 knee replacement device, but there are no reports on its clinical outcomes so far.
Silicon nitride coatings
Silicon nitride (Si3N4) ceramics have long been used clinically in interbody fusion devices for spinal surgery (38). Their application in neurosurgical and maxillofacial devices is especially attractive for the lack of artefacts in nuclear magnetic resonance imaging (39). The potential of bulk Si3N4 in the production of ball heads and inserts for THRs has been investigated for some time (40, 41), and a clinical trial of Si3N4 ball heads manufactured by a US company is presently in progress (42). For an exhaustive review of the application of Si3N4 ceramics, the reader may refer to the work of Sonny Bal and Rahaman (43).
Amorphous or nanocrystalline Si3N4 coatings can be obtained by PVD or chemical vapor deposition (CVD) (44, 45). The coating composition can be tailored in terms of silicon to nitrogen ratio and in concentration of additives such as carbon, oxygen or fluorine. Si3N4 coatings on cobalt-chromium alloy are presently under development in the framework of an EU-funded project (46, 47) for application in hip or knee prosthesis bearings. Si3N4 ball heads and liners are also used as a substrate for nanocrystalline diamond (NCD) coating (48–49–50).
Zirconium dioxide coatings
ZrO2 coating has the largest body of literature about its clinical outcomes. In orthopedics, this technology is proprietary, belonging to Smith & Nephew (Memphis, TN, USA). It is not strictly a coating, because it is a 5 μm-thick surface scale of blue-black oxide formed by high temperature oxidation. For a comprehensive review of the behavior of zirconium oxides, the reader may refer to the work by Hobbs et al (51).
Papers by Davidson et al (52) and Hunter et al (53) give a comprehensive overview of the process to obtain the blue-black monoclinic ZrO2 surface layer on Zr-2.5Nb alloy (ASTM B531) as well as improvements in coating quality. The work by Hunter et al also discusses the optimization of the layer thickness in view of the control of residual stresses arising due to the difference in density and in thermal expansion coefficients between the oxide and the metal substrate. Briefly, intensity and direction (tensile-compressive) of the stresses depend on the oxidation temperature and on coating thickness, then the coating process has to control these parameters in a way that residual stresses become compressive.
The US Food and Drug Administration approved oxidized zirconium (OxZr) for clinical use in 1995. By 2012, about 350,000 TKRs and about 150,000 THAs were performed worldwide using OxZr components.
Zirconium dioxide: clinical results in THR bearings
Studies performed in hip simulators under standard conditions on artificially damaged head surfaces show that OxZr – in comparison with CoCr components – is superior, or at least equivalent, in its wear behavior (54–55–56–57). Nevertheless, such in vitro results are not confirmed by a growing body of clinical evidence (58–59–60–61–62–63–64–65–66) that is putting into question the advantages of OxZr over CoCr ball heads in hip replacements. For a summary of these studies, see Table II.
Clinical reports of outcomes for THRs with oxidized zirconium ball heads
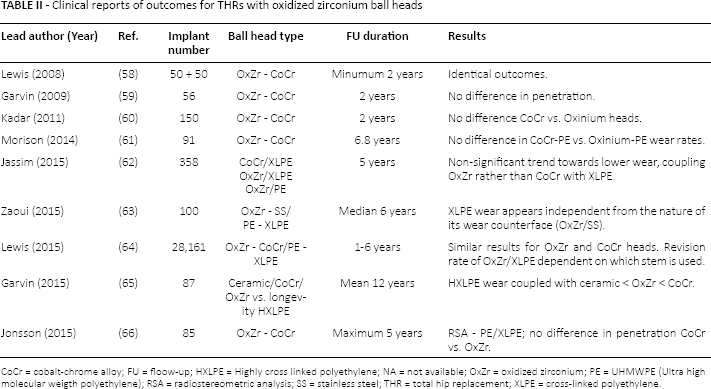
CoCr = cobalt-chrome alloy; FU = floow-up; HXLPE = Highly cross linked polyethylene; NA = not available; OxZr = oxidized zirconium; PE = UHMWPE (Ultra high molecular weigth polyethylene); RSA = radiostereometric analysis; SS = stainless steel; THR = total hip replacement; XLPE = cross-linked polyethylene.
A study by Kadar et al (60) may be taken as an example of the doubts raised about the benefits of OxZr femoral heads in the clinical setting. This randomized study evaluated the wear and migration of 5 different cemented THRs. They enrolled 150 patients who received (a) a Charnley femoral stem with a 22.2-mm head coupled to a γ-sterilized Ogee cup; or (b) a Spectron EF femoral stem with a 28-mm head used with either EtO-sterilized polyethylene (Reflection All-Poly) or highly cross-linked (Reflection All-Poly HXLPE) cups, combined with either CoCr or Oxinium femoral heads. After 2 years, in the Spectron group, there was no significant difference in wear for OxZr versus CoCr ball heads. The EtO-sterilized UHMWPE cups had more than 4 times higher proximal penetration than the highly cross-linked polyethylene (HXLPE) cups, irrespective of the head used. The Charnley/Ogee system “was not outperformed” in the trial.
The largest study of OxZr bearings so far was by Jassim et al (62). They enrolled 400 patients undergoing hip arthroplasty in 4 hospitals, comparing wear, functional outcomes and complications. Randomized groups of patients received (a) a CoCr femoral head and XLPE liner, (b) OxZr femoral head and XLPE liner, or (c) OxZr femoral head and conventional UHMWPE liner. There were no statistically significant differences in clinical scores of the 368 patients available at 5-year follow-up. Penetration was significantly higher in the UHMWPE liner group compared with both XLPE liner groups, but no significant difference was noted between CoCr and OxZr articulating with XLPE.
Also the results presented by Zaoui et al (63) show that in the clinical setting, XLPE wear appears to be independent from the nature of surface of the metallic the ball head. One hundred patients were randomized to receive cemented Charnley stems (22.25-mm bearings) with either OxZr or stainless steel (SS; M30NW) femoral heads. UHMWPE was used in the first 50 patients, whereas XLPE was used in the next 50 patients. All other parameters were identical in both groups. At a median 6-year follow-up (range 4-8 years) Merle d'Aubigné scores among the 4 groups were similar. Apart from the SS-UHMWPE group, all of the other groups had a steady-state penetration rate well below the osteolysis threshold set by Dumbleton et al (67).
A study by Garvin et al (59) is presently the one with the longest follow-up for OxZr (mean follow-up 12 years, range 9-14 years). The study was carried out retrospectively on the records of 87 patients 50 years old or younger (96 hips) who had undergone hip arthroplasty in the authors’ hospital from 1999 to 2005. All of the implants had the same XLPE acetabular component coupled to 2 different stems (tapered press fit or porous coated). Femoral heads were made out CoCr (n = 19), ceramic (n = 34) or OxZr (n = 43), and different bearing diameters were used (φ26 mm, n = 14; φ28 mm, n = 71; φ32 mm, n = 11). At the follow-up, none of the hip radiographs showed evidence of loosening or osteolysis. The authors reported that linear and volumetric wear of XLPE coupled with 28-mm ceramic heads were much lower than with OxZr and on CoCr, notwithstanding the differences in pathology among patients and in stem types, bearing materials and diameters among implants.
A further body of literature reports cases of damage to OxZr ball heads following dislocation of the joint during handling in the operating room. Cases of severe OxZr scale damage have been reported since 2007 (68–69–70–71–72–73–74). The thin, hard oxide surface scale applied onto the soft substrate can be severely scratched in the case of contact with a hard surface (e.g., intraoperatively), in contacts with the socket rim in cases of joint instability or by interposition of third bodies in the bearing gap.
This problem was shown in the retrieval analysis of OxZr femoral heads performed by Moussa et al (75) in the Hospital for Special Surgery, New York, USA. They analyzed 59 OxZr retrieved ball heads explanted for recurrent dislocation. Eighteen heads showed gross visual evidence of substantial surface damage, disruption of the OxZr layer exposing the metal alloy underneath. The case reported by Cassar-Gheiti et al (76) shows the relevance of the problem. They treated a patient 10 years postoperatively who at the age of 35 had received a bilateral THR, with OxZr/XLPE bearings. After revision due to pain, both implants showed radiographic evidence of XLPE wear and extensive osteolysis. Magnetic resonance imaging (MRI) and computerized tomography showed catastrophic wear of the ball head and of the socket (XLPE insert and metal shell), cortical expansion and large cystic lesions. The patient underwent 2-stage revision surgery, with the implantation of a spacer with antibiotics, followed by the implantation of a tumor prosthesis.
Carbon coatings
Diamond-like carbon (DLC) coatings
Diamond-like carbon (DLC) refers to a class of carbon-based materials with process-dependent characteristics and behavior. The structure of DLC films may be described as a dispersion of diamond “nodules” in a graphite matrix. It is inherently metastable, and may transform to graphite at high temperatures. Their characteristics are often described by the ratio sp3/sp2 – for example, the concentration of diamond-type bonds vs. the graphite ones, a ratio that depends on the film deposition conditions. The biocompatibility of DLC coatings is a well-documented behavior (77–78–79–80). As in other coatings, the main problem with DLC coatings as well is the adhesion to the substrate, as the interfacial residual stresses may reach very high values within the 1- to 2-µm-thick coating layer. Several comprehensive reviews (81–82–83–84) were published in recent years about the potential application of DLCs in medical devices, and the development of nanocrystallyne diamond coatings (NCD) may offer new opportunities.
A number of experimental works have aimed to assess the wear behavior of DLC with regard to its use in THR bearings. The results have been confounded because these studies have been carried out on a number of different materials (different process parameters and different manufacturers). In addition, wear tests have been made with different experimental configurations and different environments. The results of hip simulator tests were controversial: e.g. Mishra and Davidson (83) measured wear rates of UHMWPE cups similar for alumina and DLC coated heads. Nevertheless, the same cups had lower wear rates if coupled with CoCr ball heads (83). Affatato et al (36) measured similar wear in UHMWPE cups against DLC-coated and uncoated CoCr heads, both values higher than the wear of the same cups against alumina heads.
Only a few attempts at clinical use of DLCs in joint replacement bearings have been reported so far, and at least 3 cases of clinical failure are described in the literature. The one involving the most patients was that of the knee replacement Diamond Rota Gliding, implanted in about 200 patients in Switzerland, which was withdrawn from the market in 2001 due to some cases of failure shortly after implantation, for delamination of the coating and high polyethylene wear (85). A French company made a further attempt with DLC coated components for shoulder replacements and ankle joints, but soon left the market (86). Taeger et al (87) reported the results of a clinical prospective study comparing the survivorship of 202 hip athroplasties with DLC-coated/UHMWPE either alumina/UHMWPE bearings, carried out by the same surgeonover a 2 years period. Survivorship analysis for aseptic loosening at a mean 7.5 years postoperatively demonstrated a significant difference between the 2 groups (54 % survival for DLC/UHMWPE vs. 88 % for Al2O3/UHMWPE bearings). No correlation with variables such as age, sex or bodyweight could be detected. Scanning electron microscopy (SEM) analysis detected a number of small pits in the diamond-carbon layers on the surfaces of 19 DLC heads retrieved in revision for aseptic loosening. Debris due to delamination of the DLC layer caused high UHMWPE wear and - in some cases - the metal heads too were worn out. Failures of DLC coated THR ball heads were also reported by de Thomasson et al (88).
An interesting approach now under development consists of the application of NCD coating on Si3N4 (89). NCD coatings can be obtained by CVD from hydrocarbon gases like methane at temperatures in the range 500°C-800°C. Si3N4 is the preferred substrate, because of the chemical bonds assuring the good adhesion of NCD coatings. Wear tests of ceramic–ceramic bearings with NCD coatings applied on Si3N4 ball heads and liners gave promising results (90, 91). Also, testing of multilayer NCD coatings on titanium or CoCr alloys is reported in the literature (92, 93), but information about clinical studies are missing so far.
Pyrolytic carbon coatings
Pyrolytic carbon (PyC), also known as low temperature isotropic (LTI) carbon, is a form of elemental carbon with a structure composed of disordered graphite-like layers randomly oriented. This gives PyC isotropic physical and mechanical properties.
PyC has long been in clinical use in cardiovascular implants, especially in heart valves or cardiovascular stents. It is also used in interphalangeal joints, but discussions about the advantages of PyC implants are still ongoing (94–95–96–97). PyC has been investigated for use in hip replacements since the 1980s (98), but only a few papers deal with the results obtained by in vivo tests in the clinical setting. Rettig et al (99) made mention of experimental PyC hip replacements in beagles without reporting the outcomes of these experimental implants. Jung et al (100) evaluated hemiprostheses made of PyC-coated graphite in rabbits, observing degenerative damage of the cartilage 12 weeks postoperatively in histologic sections. So far, the only clinical results reported in the literature are from Bernasek et al (101), who carried out a prospective pilot study that included 17 patients treated with unipolar hemiarthroplasty due to either femoral neck fracture or osteonecrosis. Patients received a titanium alloy stem with a graphite modular femoral head with the articular surface coated with PyC. Results were not satisfactory; the authors did not recommend the use of PyC-coated heads in hip hemiarthroplasty.
Discussion
The application of ceramic coatings on metallic ball heads was introduced in hip arthroplasty to improve the wear behavior of metal–polyethylene bearings. Taking into account that the main wear mechanisms of polyethylene in THR bearings are abrasive wear and adhesive wear, the objective of any surface treatment is (a) to minimize the abrasive wear, improving the scratching resistance of the surface, and (b) to minimize adhesive wear, e.g., by improving the wettability of the surface.
The development of this technology can be traced to the second half of the 1980s. Early studies focused especially on TiN and on different carbon coatings. Nevertheless, the number of clinical reports dealing with the outcomes for THR with ceramicized ball heads of these types is small, as reviewed by van Hove et al (29). The few papers reporting clinical outcomes for TiN-coated ball heads (30, 31) show contradictory results. This may depend on the technologies used to obtain the coatings. The use of “graded” coatings formed by several layers of different materials, as in the new coatings reported in papers by Reich et al (37) and Thomsen et al (102) looks promising, but reports on their clinical use in hip replacements – if any – are still missing.
PyC coatings (e.g., LTI/ULTI carbon and vitreous carbon) were also developed in the 1980s, but after a few attempted uses in hemiarthroplasty, today the use of these coatings seems limited to small joints. Investigations into DLC coatings have long in progress, but attempts at clinical applications in joint replacement have led to failures so far (85–86–87). The development of NCD coatings or of Si3N4 coatings for THR bearings presently in progress (46, 45, 89, 90, 93) may open new perspectives to this technology in arthroplasty, but its effectiveness still needs to be demonstrated in the clinical setting.
In contrast with the situation described above, there are a rather large number of papers reporting clinical outcomes for THR bearings with OxZr ball heads, although the effectiveness of this technology in terms of wear reduction and in cost to benefit ratio is controversial. This is exemplified by, e.g., the comparison between the results recently reported by Karidakis and Karachalios (103), which showed a reduction in wear using OxZr/XLPE bearings vs. ceramic/XLPE bearings, and those reported by Garvin et al (65) showing that ceramic/XLPE bearings had much lower wear rates than CoCr/XLPE or OxZr/XLPE. The lack of advantages in wear with OxZr over CoCr was also remarked on by several other authors (58–59–60, 63), who noted that the decrease in wear of the bearings was likely due to the cross-linked polyethylene liners, rather than to the ball head surface. Also data in the Australian Orthopaedic Association National Joint Replacement Registry (104) show that the revision rate for loosening or lysis is greater depending on the type of polyethylene (cross-linked or non-cross-linked) used rather than on the type of ball head (OxZr or CoCr). In addition, the reduction in revision rates for loosening or lysis observed in some OxZr/XLPE bearings may depend on the stem type used, not on the wear debris released by the bearing (64).
Cases of damage of the surface of ceramicized ball heads leading to an increase of bearing wear were reported for TiN-coated ball heads (30, 31, 34), and especially for OxZr ball heads (65–66–67–68–69–70–71). The scratching resistance of an oxidized zirconium surface is rather low (105). Damage of the oxide scale after luxation of the joint has been reported (68, 69, 72–73–74–75–76). This is a relevant complication, because it has the potential to increase the wear of polyethylene liners, when revision in case of luxation has to be considered. Moreover, cases of damage of the OxZr surface by third bodies, as well as of accidental contacts with metallic surfaces during ball head insertion or by contacts with metallic instruments during surgery, have been reported, highlighting the need for special care in using ceramicized components.
Conclusions
The potential advantage of ball heads with ceramicized surfaces in hip replacement bearings lies in the decrease of polyethylene wear, and the development of ceramicized ball heads is still in progress. While nonarticular ceramicized surfaces can be very effective in avoiding allergic reactions in patients sensitized to metallic ions, the debate on the effectiveness of ceramicized ball heads to decrease wear in THR bearings is still open whatever the coating type.
The debate is keep alive especially because there are few reports about clinical outcomes for THR bearings, and most of the results of the studies published so far raise doubts regarding the effectiveness of this technology in hip arthroplasty.
Besides the poor clinical results of PyC- or DLC-coated ball heads in joint replacement bearings, the results of the few clinical studies on nitride coatings are also controversial, indicating a need for further investigations. More studies are reporting outcomes for THR with OxZr ball heads, but the advantages of OxZr over CoCr alloy in decreasing the wear of the polyethylene counterface is still in question. Several studies show that the wear of the bearing looks more depending on the use of cross-linked polyethylene liners than on the treatment of the ball head surface.
As a general conclusion, it can be noted that the integrity of the surface layer and its adhesion to the metal substrate in the clinical setting remain the key points, whatever the surface treatment of the ball head. The survival and effectiveness of the joint replacement system depends on the stability of the ceramic layer throughout the service life of the implant. If damage of the surface ceramic layer occurs, then all of the system fails. The risks of damage to the articulating surface have to be carefully taken into consideration – and patients informed about them – while selecting the most appropriate hip replacement system.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has any financial interest related to this study to disclose.