
Abstract
Purposes
The aim of the present study was to evaluate the importance of isolated microorganisms according to the Gram stain and the type of antibiotic received on the outcome of early prosthetic joint infection (PJI) treated with debridement, antibiotics and implant retention (DAIR).
Methods
From January 1999 to December 2009, all patients with an early PJI were prospectively registered in a database and they were retrospectively reviewed for this study.
Results
During the study period, 160 patients met the inclusion criteria of the study. After a mean (SD) post-debridement follow-up of 5.2 (2.5) years, 117 patients (73.1%) were considered to be in remission and 43 (26.9%) were classified as failure. Variables associated with failure were liver cirrhosis (66.7% vs. 22.8%, p=0.001), diagnosis within the first 30 days from arthroplasty (30.4% vs. 8.0%, p=0.020), C-reactive protein (CRP) >12 mg/dl (46.7% vs. 21.2%, p=0.005), microorganism isolated in all deep samples (31.1% vs. 16.0%, p=0.047) and Gram-negative (GN) infection not treated with a fluoroquinolone (57.1% vs. 20.0%, P=0.004). Gram-positive (GP) infection not treated with rifampin was close to be statistically significantly associated with failure (34.4% vs. 19.2%, p=0.067). A multivariate analysis identified liver cirrhosis (OR: 12.4 CI95%: 3.1-49.7, p<0.001), CRP-value (OR: 1.06 CI95%: 1.0-1.11, p=0.049), and when a GN-infection was not treated with a fluoroquinolone (OR: 6.5, CI95%: 1.8-23.8, p=0.005) as independent predictors of failure.
Conclusion
The remission rate of PJI treated with DAIR after 3 years of follow-up was 73%. The main predictors of failure were liver cirrhosis, the selected antibiotic most specially fluoroquinolones for GN and rifampin for GP infections, the C-reactive protein and the number of samples culture positive as a potential surrogate markers of bacterial density.
Introduction
Early prosthetic joint infection (PJI) is an uncommon but severe complication after joint arthroplasty. Debridement and prosthesis retention is an accepted therapeutic approach when the infection is diagnosed within the first 90 days from arthroplasty and there are no radiological signs of loosening (1, 2). The most frequently isolated microorganisms are Gram-positive (GP) cocci, including Staphylococcus aureus and coagulase-negative staphylococci (CNS) (3, 4), however, Gram-negative (GN) microorganisms are increasing and they are frequently resistant to antibiotics (5-7).
For staphylococcal infections, observational studies (8-10) and one randomized study (11) have described the outcome and risk factors associated with failure. The importance of microbial etiology, including Gram-positive and Gram-negative microorganisms and the type of antibiotic used, however, has not been previously described in large case series of early PJI treated with debridement, antibiotics and implant retention (DAIR). The aim of the present study was to evaluate the importance of isolated microorganisms according to the Gram stain and the type of antibiotic received on the outcome of early PJI treated with DAIR.
Material and Methods
From January 1999 to December 2009, all patients with a PJI (hip hemiarthroplasty, total hip and knee arthroplasty) were prospectively registered in a database and retrospectively reviewed for this study. Relevant information about demographics, co-morbidity, type of implant (hip or knee prosthesis), clinical manifestations, leukocyte count and value of C-reactive protein (CRP) at the moment of admission for infection, surgical treatment, isolated microorganism, antimicrobial therapy, and outcome were recorded. For the present study, only those cases with an early PJI with at least 3 years of follow-up were included and retrospectively reviewed. Early PJI was defined by the presence of local inflammation of acute onset (<15 days of symptoms duration) during the first 90 days after joint arthroplasty, macroscopic evidence of extension of the infection through the capsule during debridement, and isolation of microorganisms in deep samples.
In terms of debridement, pre-existing incisions were always used, necrotic tissue was excised, and the joint was washed with 6 L to 9 L of sterile water. The components were left in situ after confirming that no signs of loosening were present at the time of surgery. In total hip and knee arthroplasties, the polyethylene and modular components were exchanged. Three or more deep samples of synovial fluid and periprosthetic tissue were submitted to the microbiology laboratory. In addition, blood cultures were performed for patients who presented with fever at the moment of admission for infection. An antibiogram for all the isolates was performed by microdilution method. After debridement, a broad-spectrum intravenous antimicrobial regimen including vancomycin (1 g/12 h) plus ceftazidime (2 g/8 h) was started and maintained until definitive microbiological results were obtained. The protocol of our hospital recommends 10 days of intravenous antibiotics. The duration of oral antibiotics was not standardized and it was decided by a member of the team (A.S.) in each case according to the clinical manifestations and the CRP value. After being discharged, patients were followed-up monthly when they were receiving treatment, every 3 to 6 months during the first year after finishing the therapy, and once per year afterwards. Failure was considered when inflammatory signs and high CRP remained during treatment and the patient needed a second debridement, or when signs and symptoms re-appeared after completing antibiotic treatment (relapse or re-infection depending on the microorganism isolated), or when death was related to the infection. The need of implant removal due to aseptic loosening, defined as negative intraoperative cultures, was not considered as failure.
Statistical analysis
The variables analyzed were age, sex, co-morbidity (having or not having one of the following entities: hypertension, ischemic heart disease, diabetes mellitus, malignancy, liver cirrhosis, chronic renal failure, rheumatoid arthritis, corticotherapy, senile dementia, or chronic obstructive pulmonary disease), site of arthroplasty (hip or knee), type of previous surgery (primary or revision), age of implant, presence of fever, leukocyte count, CRP value, positive blood cultures, number of positive cultures out of those obtained, type of microorganisms isolated, and days antibiotic therapy. For the statistical analysis, continuous variables were compared by Student's test and categorical variables were compared by the Chi-square test or Fisher's exact test when necessary. The Kaplan-Meier survival method was used to estimate the cumulative probability of treatment success of the whole cohort from debridement. Log-Rank test was applied to compare survival curves. A forward, stepwise, logistic regression model to identify independent predictors of failure was performed. The validity of the model was assessed by estimating the goodness-of-fit to the data with Hosmer-Lemeshow test. Statistical significance was defined as a two-tailed p<0.05. The analysis was performed using SPSS, version 15.0 (SPSS, Inc., Chicago, IL, USA).
Results
During the study period, 160 patients with early PJI met the inclusion criteria of the study. The mean (SD) age of cohort was 71.4 (10.3) years; 72 were male (45.0%), 70 infections (43.8%) were on a hip prosthesis and 90 (56.3%) on a knee prosthesis. In 135 (84.4%) cases the infected prosthesis was a primary arthroplasty and in 25 (15.6%) a revision arthroplasty. The mean (SD) age of prosthesis at the moment of infection diagnosis was 24.2 (20.4) days, and it was <15 days, 16 to 30 days or >30 to 90 days in 54, 81, and 25 cases respectively. Fever was present in 30 patients (18.9%) and the pre-operative mean (SD) leukocyte count was 9233 (4080) cells/mm3. The pre-operative mean (SD) CRP was 7.4 (7.8) mg/dl, and it was <5 mg/dl, 5-12 mg/dl or >12 mg/dl in 77, 41, and 30 cases, respectively. The most frequently isolated microorganisms were coagulase-negative staphylococci (66 cases, 41.3%), S. aureus (59 cases, 36.9%), Enterococcus spp (29 cases, 18.1%), Escherichia coli (25 cases, 15.6%), Pseudomonas aeruginosa (17 cases, 10.6%), Enterobacter cloacae (13 cases, 8.1%), and Proteus spp (12 cases, 7.5%). PJI was polymicrobial in 65 cases (40.6%), and in 62 cases (38.8%) at least one GN microorganism was isolated. Seven patients (6.6%) had bacteremia. After a mean (SD) follow-up from debridement of 5.2 (2.5) years, 117 patients (73.1%) were considered to be in remission and 43 (26.9%) were classified as failure.
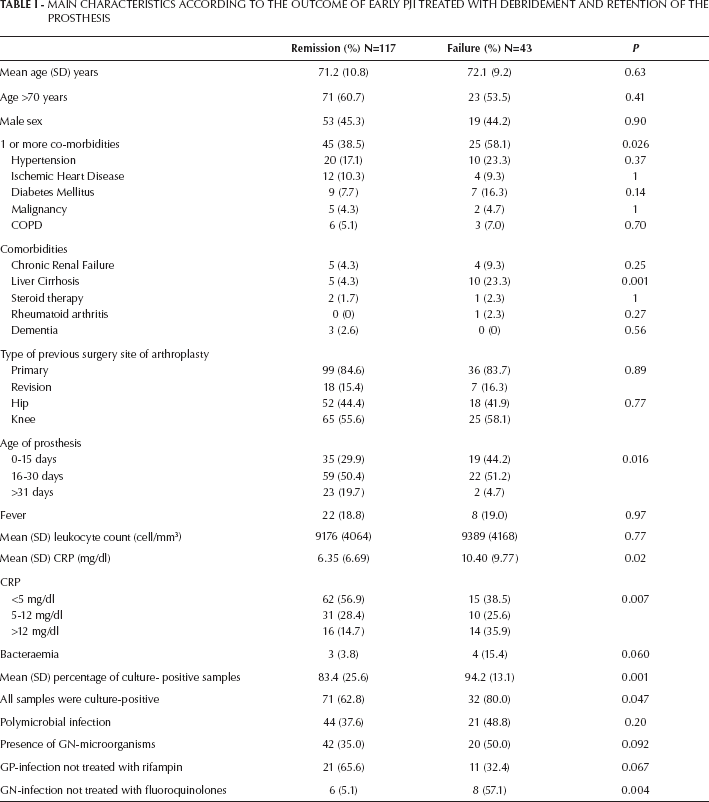
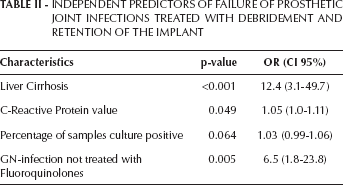
Characteristics of patients according to the outcome are shown in Table I. Patients without co-morbidities had a significantly lower failure rate than patients with one or more co-morbidities (20.0% vs. 35.7%, p=0.026). Individually, only liver cirrhosis was significantly associated with failure (66.7% vs. 22.8%, p=0.001). Patients diagnosed within the first 30 days from arthroplasty had a higher failure rate than those treated beyond the first 30 days (30.4% vs. 8.0%, p=0.020). Patients with a pre-operative CRP value >12 mg/dl had a higher failure rate (46.7% vs. 21.2%, p=0.005). Mean (SD) percentage of samples culture positive was significantly higher in patients who failed (94.2 (13.1) vs. 83.4 (25.6), p=0.001), and those patients in whom a microorganism was isolated in all deep samples had a significantly higher failure rate (31.1% vs. 16.0%, p=0.047). The presence of a GN was associated with a higher failure rate and a higher cumulative probability of failure after 3 years of follow-up (Fig. 1) but the difference did not achieve statistical significance. In order to identify the importance of antibiotic treatment, we decided to evaluate the most relevant antibiotic for GP and GN infections according to the previous literature. According to this, two new variables were created, patients with a PJI due to a GP receiving rifampin and patients with a PJI due to a GN receiving a fluoroquinolone. The cumulative probability of failure among GP infections was higher when rifampin was not given, although the difference was not statistically significant (Fig. 2). On the other hand, the cumulative probability of failure was statistically significantly higher among those GN infections that did not receive a fluoroquinolone (Fig. 3). A multivariate analysis, including these two variables, identified liver cirrhosis (OR:12.4, CI95%:3.1-49.7, p<0.001), CRP-value (OR:1.06 CI95%:1.0-1.11, p=0.049), and when a GN-infection was not treated with a fluoroquinolone (OR:6.5, CI95%:1.8-23.8, p=0.005) as independent predictors of failure (Tab. II). The model included the percentage of culture-positive samples, although it was not statistically significant (OR:1.03, CI95%: 0.99-1.06, p=0.064) (Hosmer-Lemeshow goodness-of-fit statistic=4.0, p=0.86).
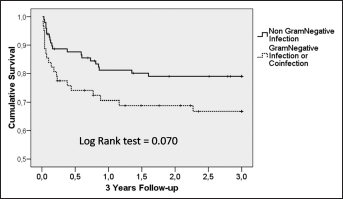
The cumulative probability of survival of the whole cohort after 3 years of follow-up according to the presence or absence of Gram-negative microorganisms.
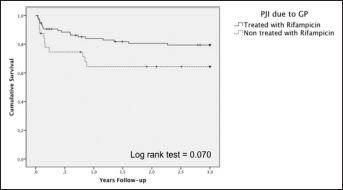
The cumulative probability of survival after 3 years of follow-up of prosthetic joint infections due to Gram-positive microorganisms treated with or without rifampin.
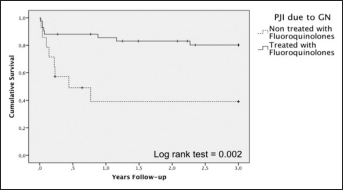
The cumulative probability of survival after 3 years of follow-up of prosthetic joint infections due to Gram-negative microorganisms treated with or without fluoroquinolones.
MAIN CHARACTERISTICS ACCORDING TO THE OUTCOME OF EARLY PJI TREATED WITH DEBRIDEMENT AND RETENTION OF THE PROSTHESIS
INDEPENDENT PREDICTORS OF FAILURE OF PROSTHETIC JOINT INFECTIONS TREATED WITH DEBRIDEMENT AND RETENTION OF THE IMPLANT
Discussion
Infection is a severe complication after arthroplasty that occurs in 1% to 3% of cases (12). In early acute infections, DAIR is an accepted therapeutic approach, however, it is associated with a wide variation in the success rate (9-11, 13-16). Reasons for this inconsistency could be related to host characteristics, surgical technique, etiologic pathogen, or antibiotic treatment. Host co-morbidity, including diabetes mellitus, has not been identified in previous series as an independent predictor of failure (9, 10, 17). In our cohort, diabetes mellitus or other co-morbidities were not associated with failure except liver cirrhosis. There were 15 cases and their failure rate was significantly higher (23%), therefore, it is necessary to carefully select these patients for arthroplasty. Aspects related with surgical technique include an extensive debridement but also the exchange of modular components. A recent large case series of PJI due to S. aureus has demonstrated that the exchange of modular polyethylene liner is an independent variable associated with success (16). This variable was not analyzed in our series because this procedure is included in the protocol of our institution and exchange was performed in all patients. As regards the etiology, previous experience has shown that cases due to methicillin-resistant staphylococci have been associated with a higher failure rate (18-21), however, the majority of these patients were mainly treated with intravenous vancomycin, an antibiotic with a poor activity against bacterial biofilms (22). More recent experience using rifampin combinations did not find significant differences in the outcome of patients with PJI due to methicillin-susceptible or resistant strains (9, 16, 23). Although the difference was not statistically significant (Fig. 2), there was a trend toward a better result in GP infections when rifampin was included in the antibiotic regimen. Experience in PJI due to GN managed with DAIR is scarce but suggests that it is associated with a worse outcome than in GP infections (24). However, some authors have demonstrated that when fluoroquinolones are included, the treatment success rate is higher than 80% (5, 25). The present study clearly supports this concept (Fig. 3) and indeed, treating with a fluoroquinolone GN infections was an independent predictor for success. These results suggest that more than the type of microorganism causing the infection, what determines the outcome of the patient is the selected antibiotic, being particularly important to choose agents with high activity against biofilms like rifampin for GP (21) or fluoroquinolones for GN (26).
Interestingly, a high CRP at the moment of diagnosis and a high percentage of deep samples (obtained during debridement) that were culture positive were independent predictors of failure. Recently, Bouaziz et al (27) in a cohort of PJI due to S. aureus found that when suction samples or all samples during surgery were culture-positive the outcome was significantly worse. CRP and the number of positive samples are probably good markers of bacterial density and the deleterious effect of high bacterial density on the effectiveness of antibiotics is well described (28). In the future, besides new anti-infective and osseointegrating biomaterials helpful to prevent infection, laboratory and microbiological markers could be useful to identify patients requiring more aggressive antimicrobial therapy (29-32).
In conclusion, the remission rate of PJI treated with DAIR after 3 years of follow-up was 73%. The main predictors of failure were liver cirrhosis; the selected antibiotic was most often fluoroquinolones for GN and rifampin for GP infections; and C-reactive protein and the number of culture-positive samples were both potential surrogate markers of bacterial density. In the future, it is necessary to investigate alternative antibiotics or antibiotic combinations that could be used in cases that are resistant to rifampin or fluoroquinolone microorganisms.