
Abstract
Background:
Previous studies have revealed a conflicting relationship of xeroderma pigmentosum group G (XPG) gene polymorphism with gastric cancer (GC) risk. To our knowledge, this is the first meta-analysis to investigate the association between rs751402 mutation located on the XPG promoter region and GC risk.
Methods:
We undertook a meta-analysis by identifying relevant articles from the PubMed, Web of Science and China National Knowledge Infrastructure (CNKI) databases on February 28, 2017. By pooling 9 eligible studies, 3,539 GC cases and 3,948 controls were included. The pooled odds ratios (ORs) with 95% confidence intervals (95% CIs) were calculated using the fixed-effects or random-effects model depending on the existence of heterogeneity across studies. The population attributable risk (PAR%) was estimated to better understand the public health risk.
Results:
All included studies had been conducted in China. Significant associations were found between the XPG rs751402 polymorphism and the risk of GC (TT vs. CC: OR = 1.43, 95% CI, 1.11-1.84; CT vs. CC: OR = 1.15, 95% CI, 1.04-1.26; dominant model: OR = 1.17, 95% CI, 1.07-1.29; recessive model: OR = 1.30, 95% CI, 1.05-1.62; T vs. C: OR = 1.18, 95% CI, 1.06-1.32). The estimated PAR% was about 4.9%-8.8%. Funnel plots did not reveal any potential publication bias. The sensitivity analyses showed that the results were relatively robust.
Conclusions:
This meta-analysis indicates that the XPG rs751402 polymorphism may be a risk factor for GC in the Chinese population.
Introduction
Gastric cancer (GC) is one of the most common cancers, with 952,000 people diagnosed each year worldwide, according to the Globocan 2012 (1). Worldwide, in 2015, GC was reportedly the fourth (in order of frequency) most common type of cancer, and it caused 754,000 deaths (2). Many patients are inoperable at diagnosis. Despite the fact that some comprehensive treatments are available, the 5-year survival rate of GC remains less than 35% (3). The median survival is around 1 year for metastatic GC (4). GC’s global burden of disability-adjusted life years remains heavy, and it causes a large burden on society and the economy (4). The most important etiology of GC is Helicobacter pylori infection. Other pathogens involve Epstein-Barr virus, lifestyle (e.g., diet with high salt or low fiber), environmental factors (e.g., smoking) and genetic factors (4, 5).
Mutations in the genes responsible for cell multiplication and repair result in defects in DNA repair mechanisms, and are thereby related to GC (6). Nucleotide excision repair (NER) is known as one of the primary and important DNA repair mechanisms in humans (7). Xeroderma pigmentosum group G (XPG), also known as endonuclease excision repair cross-complementing complementation group 5 (ERCC5), plays a critical role in the dual-incision that determines the NER pathway (8). This protein, encoded by the XPG gene, is a structure-specific endonuclease to cut DNA lesion on the 3’ side. Afterwards, XPG participants in the 5’ incision as a nonenzymatic scaffolding by the XPF/ERCC1 heterodimer. These simultaneous incisions can cause the instantaneous release of the damaged oligonucleotide to ensure the proper repair of damaged DNA (8, 9).
The region containing the XPG promoter and 5’-untranslated region potentially has a high rate of genomic recombination (10). A common polymorphism (rs751402 C>T) is reported to be located in the promoter region and to control XPG expression. The rs751402 is found as a cis-acting genetic variant site and influences biological aspects of XPG transcript regulation in normal human cells, including allele-specific expression at exon 2 and possibly start site usage (11). Since transcription of XPG is correlated with altered transcription domain–associated repair capacity (12), this promoter mutation seems to be associated with cancer. Studies have estimated the association between XPG genetic polymorphism (rs751402 C>T) and risk of GC (13-21). However, their conclusions remain conflicting.
To investigate this further, we performed a systematic review of published documents and a meta-analysis of case-control studies to evaluate the association between the XPG rs751402 polymorphism and GC risk.
Materials and methods
Search strategy
A comprehensive literature search of the PubMed, Web of Science and China National Knowledge Infrastructure (CNKI) databases was performed on February 28, 2017. The following keywords and the Chinese equivalent terms were searched: “gastric”, “stomach” “cancer”, “tumor”, “neoplasm”, “carcinoma”, “xeroderma pigmentosum group G”, “XPG”, “endonuclease excision repair cross-complementing complementation group 5”, “ERCC5” and “rs751402”. Meanwhile, citations in the identified articles were also scanned to find other potential studies.
Selection criteria
The inclusion criteria in this meta-analysis were as follows: (i) studies estimating the relationship between the ERCC5/XPG rs751402 mutation and GC risk; (ii) designed as population-based case-control studies; (iii) numbers of carriers of mutation and nonmutation in both groups were available; (iv) original research articles published in English or Chinese; (v) the genotypic distribution in the control group was in accordance with the Hardy-Weinberg equilibrium (HWE). No restriction regarding ethnicity was imposed. Reports of conferences and reviews were excluded. Overlapping data that were derived from the same population were also excluded.
Data abstraction
Two independent reviewers (C.Z. and Y.-Y.X.) used a standardized spreadsheet to extract information. The following data were collected: first author, publication year, mean age, sex, genotypic distribution of case and control group, type of Lauren classification, TNM stage, tumor site and, if any, result of HWE assessment. Discrepancies were resolved by discussion.
Statistical analysis
All statistical tests in this meta-analysis were performed using RevMan 5.0 software. A p value of <0.05 was considered significant unless otherwise mentioned.
The association between the XPG rs751402 polymorphism and GC risk was assessed using odds ratios (ORs) with 95% confidence intervals (95% CIs). The pooled ORs were estimated for codominant model (TT vs. CC and CT vs. CC), dominant model (TT + CT vs. CC), recessive model (TT vs. CT + CC) and additive model (T vs. C). Heterogeneity within studies was estimated by the I-squared (I 2 ) statistic and Q-test. Homogeneity was indicated when the p value of the Q-test was more than 0.1 (22). Meanwhile, I 2 values of <25%, 25%-50% and >50% were interpreted as low, middle and high heterogeneity, respectively. A random-effects model was employed if heterogeneity was detected; otherwise, a fixed-effects model was used. For better understanding the public health risk, the population attributable risk (PAR) was calculated as PAR% = Pe(OR−1)/[Pe(OR−1) + 1] × 100, where Pe was the mutation proportion of the control group (23). Sensitivity analyses were performed by removing a specific single study. Potential publication bias was evaluated by Begg’s funnel plots.
Results
Study characteristics
A total of 67 studies were initially identified. After reviewing titles and abstracts, 27 studies that did not met the eligibility criteria were excluded. For the remaining 40 records, some studies were excluded for duplication (n = 19), irrelevance (n = 11) or overlapping result (n = 1). Finally, 9 articles were included in the meta-analysis (Fig. 1). Unexpectedly, all studies had been conducted in China. A total of 3,539 GC cases and 3,948 controls were involved. Of note, the largest study, that from Hua et al, had recruited 1,142 cases and 1,173 controls (14), which accounted for nearly one third of the total participants. The main characteristics of the 9 articles are summarized in Table I.
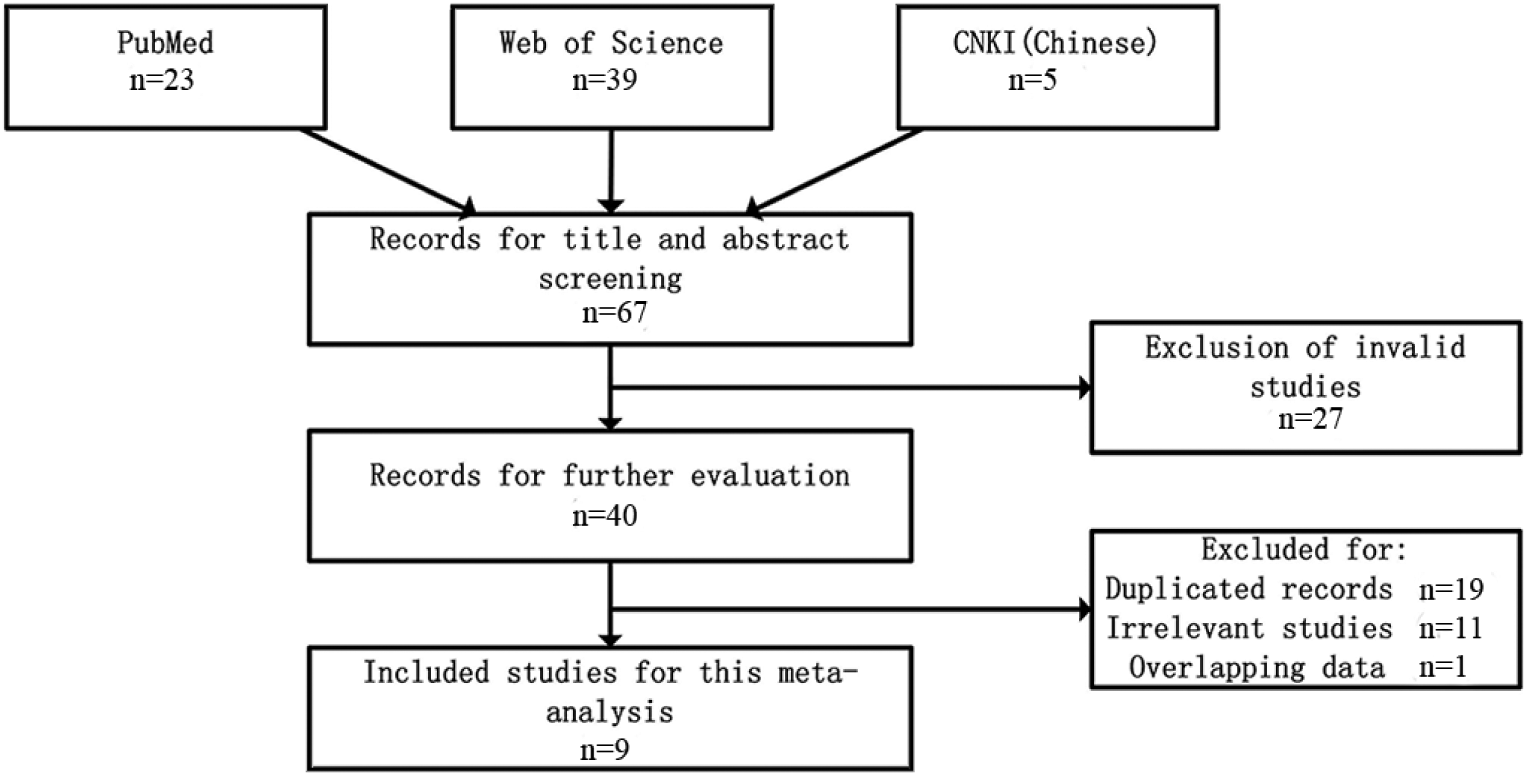
Flow chart for selection of studies. CNKI = China National Knowledge Infrastructure.
Characteristics of studies included in the meta-analysis
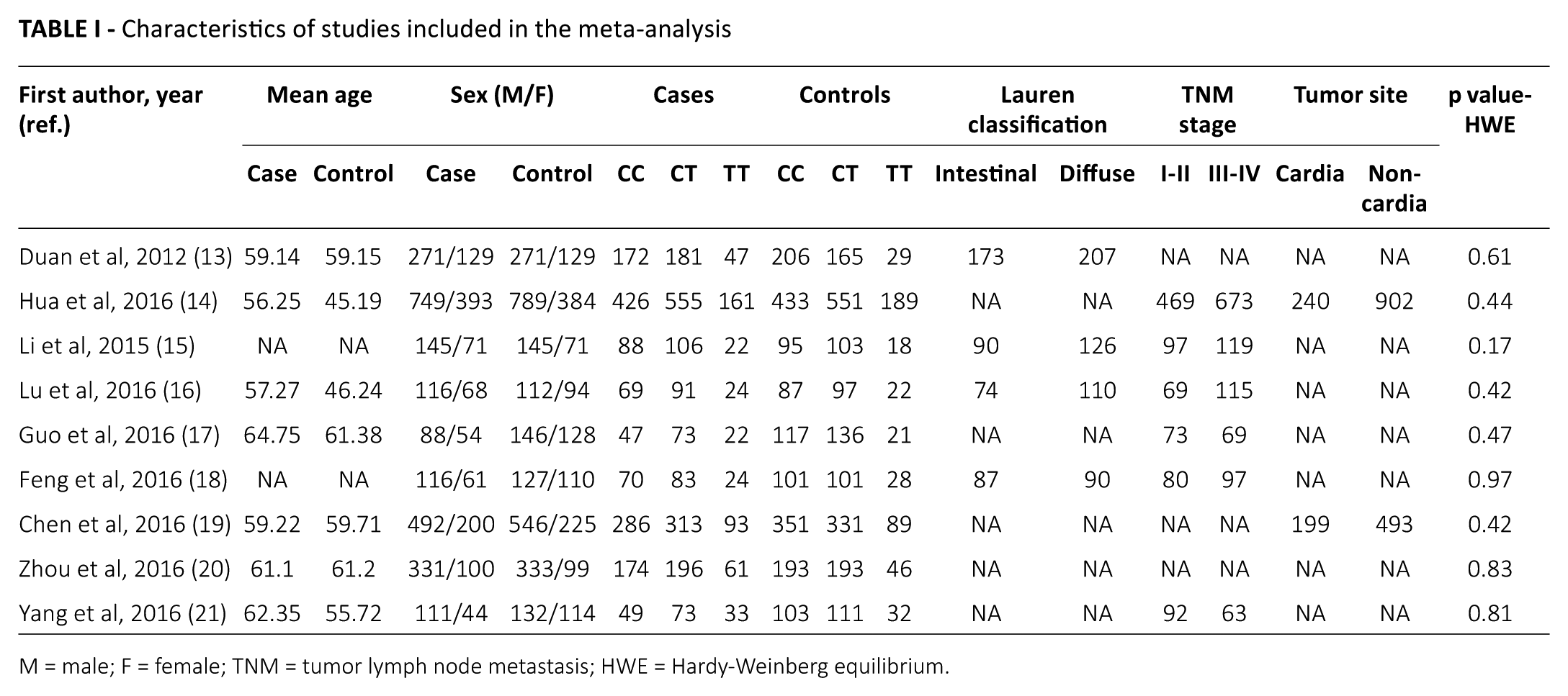
M = male; F = female; TNM = tumor lymph node metastasis; HWE = Hardy-Weinberg equilibrium.
Association between XPG rs751402 polymorphism and GC
Compared with CC genotype carriers, study participants with TT genotype were significantly associated with an increased risk of GC (OR = 1.43, 95% CI, 1.11-1.84). A high degree of statistical heterogeneity was observed (I 2 = 59%, p = 0.01) (Fig. 2A). The estimated PAR% was 4.9%. Further, individuals with CT genotype had a statistically greater GC risk (CT vs. CC: OR = 1.15, 95% CI, 1.04-1.26) with low heterogeneity (I 2 = 0%, p = 0.89) (Fig. 2B). The PAR% was 6.3%.
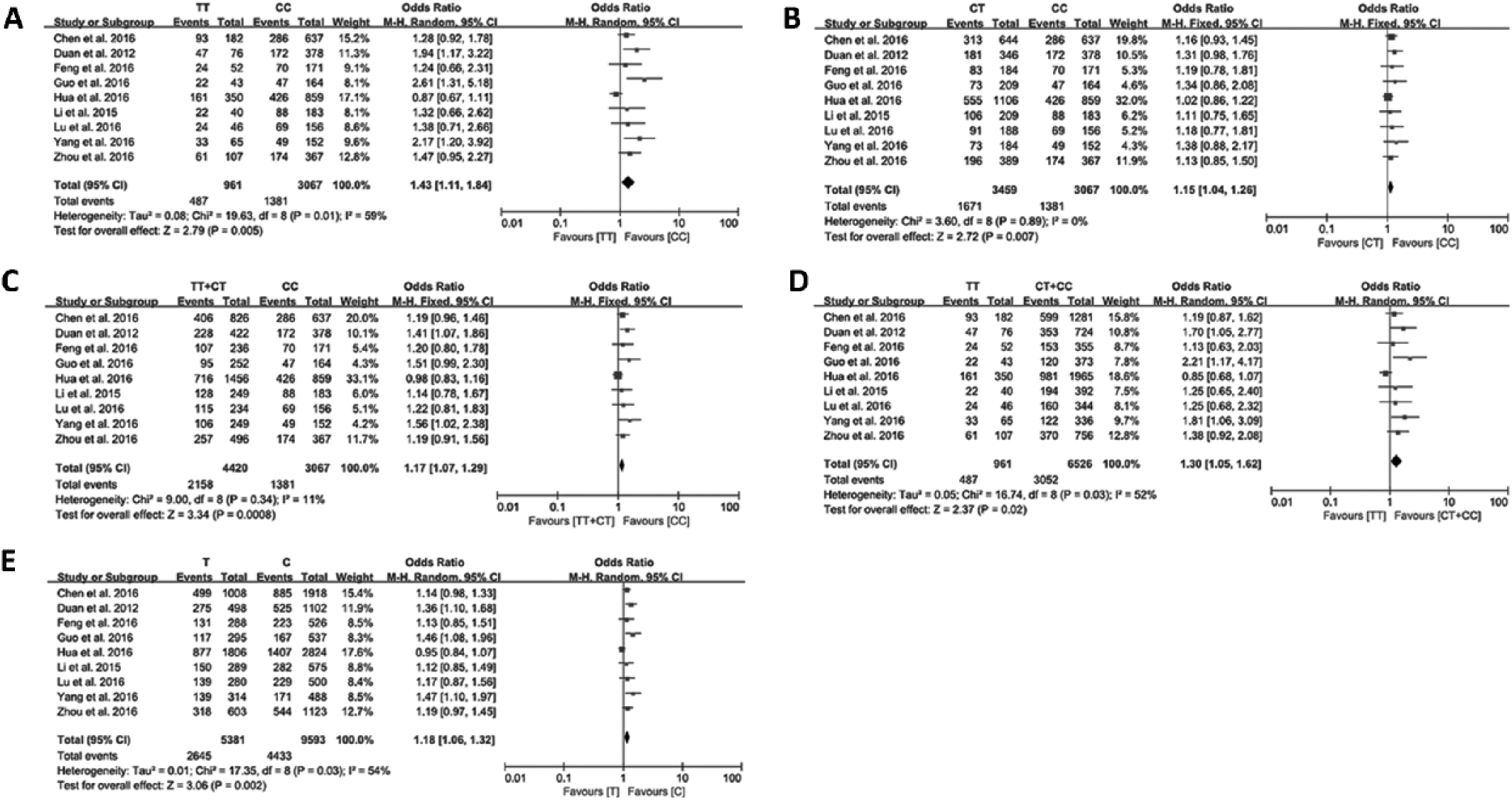
Forest plots illustrating the association of gastric cancer risk and rs751402 polymorphism in different models: (
Regarding the dominant and recessive models, the pooled ORs were 1.17 (95% CI, 1.07-1.29; I 2 = 11%, p = 0.34) (Fig. 2C) and 1.30 (95% CI, 1.05-1.62; I 2 = 52%, p = 0.03) (Fig. 2D), respectively. The PAR% was 8.8% and 4.9%, respectively. The presence of the T allele also significantly increased GC risk (OR = 1.18, 95% CI, 1.06-1.32) with high heterogeneity (I 2 = 54%, p = 0.03) (Fig. 2E). The PAR% was 5.9%.
Sensitivity analysis and bias
The sensitivity analyses demonstrated that our results were generally robust because pooled ORs were not significantly influenced by excluding any single study (Tab. II). When the largest study, that from Hua et al (14), was omitted, we observed that the risks from all models were slightly higher. In fact, the study by Hue et al reported no significant associations in any models, regardless of adjustment for crucial variables such as age, smoking and alcohol consumption (14). The only exception to the sensitivity analyses showing results were stable was observed in TT vs. CC comparison when the study by Chen et al (19) was removed, and a null result (OR = 1.48, 95% CI, 0.95-2.27) was yielded. The shape of the funnel plots did not show asymmetry, indicating no publication bias was detected (Fig. 3).
Sensitivity analyses by excluding any single study
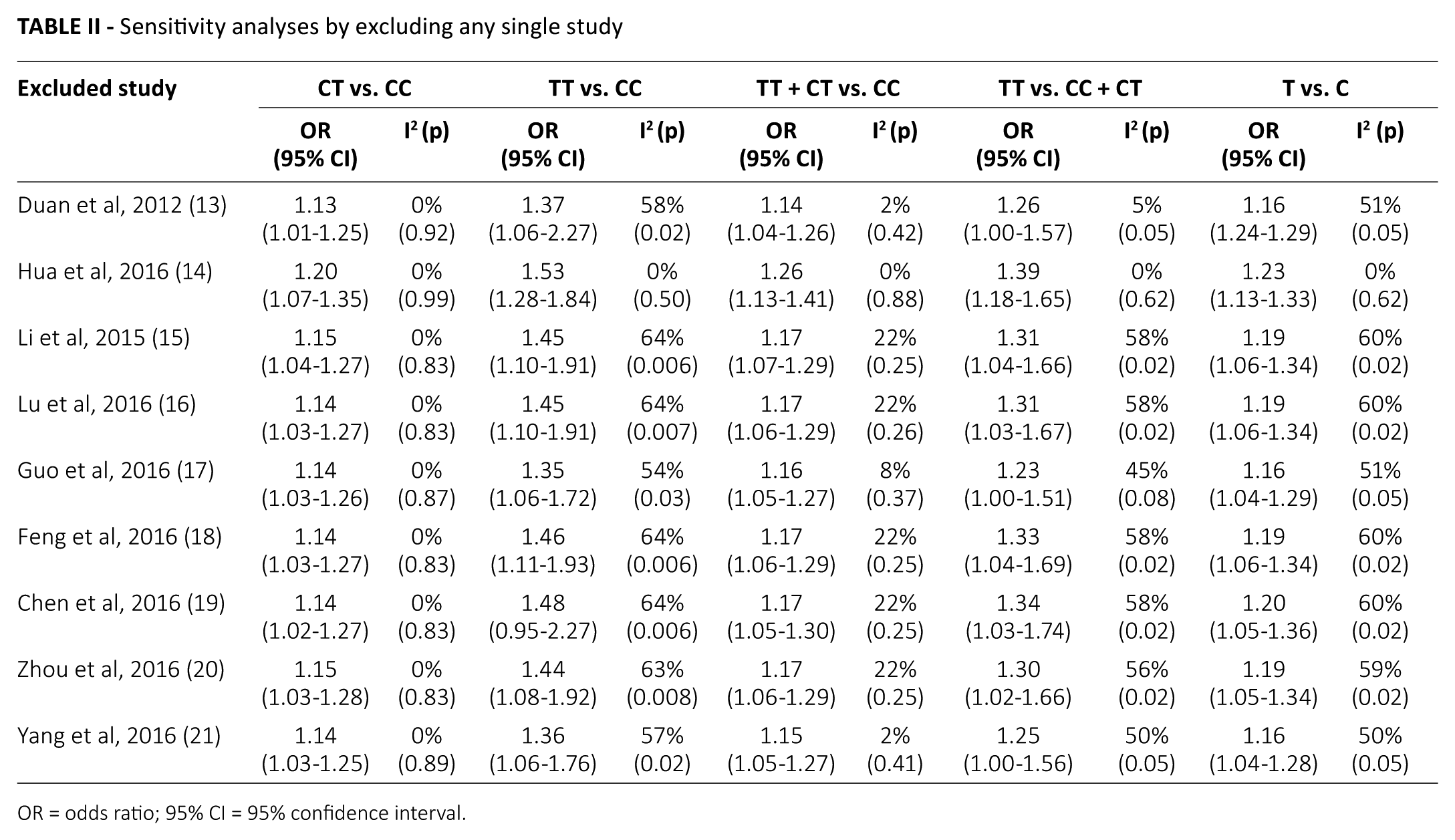
OR = odds ratio; 95% CI = 95% confidence interval.

Begg’s funnel plots to detect potential publication biases in all models. OR = odds ratio; SE = standard error.
Discussion
Since GC is one of the most common cancers and the effectiveness of therapy remains disappointing, it is important to identify novel candidate biomarkers which would be crucial for risk screening and early diagnosis. Single nucleotide polymorphisms (SNPs) are recognized as important contributors to variation of protein function, thereby causing GC (24). Using integration analysis of SNPs with gene expression profile, several SNPs have been successfully identified as GC risk loci (24). However, the results from basic medical research need to be confirmed by population studies. In recent years, some articles (13-21) have investigated the correlation between rs751402 mutation and GC risk among populations, but the results have been controversial. A possible explanation is that most of these studies have had small sample sizes. To overcome this obstacle, performing a meta-analysis that utilizes all of the available data is warranted to draw a safer conclusion. This was to our knowledge the first study that conducted a comprehensive literature review to estimate the relationship between XPG gene rs751402 polymorphism and GC risk.
This meta-analysis involved 9 case-control studies (3,539 patients and 3,948 controls), which were all conducted in China, and suggested that TT, CT and TT + CT genotypes increased by approximately 15%-43% the risk of GC in comparison with the wild-type genotype. Individuals with T allele suffered from a greater risk of GC (18%), compared with individuals with C allele. All estimated PAR% were about 4.9%-8.8%.
Based on recent evidence, populations with specific characteristics are at increased risk of GC. For instance, when the 5 possibly functional SNPs of XPG gene were combined, the carriers of 3-4 higher-risk genotypes had a significantly higher likelihood of GC (32%) than carriers of 0-2 higher-risk genotypes (14). Among the carriers of 3-4 higher-risk genotypes, those who were older than 58 years or were male were at greater risk (90% and 50%, respectively) (14). In line with these data, previous studies have suggested that individuals with the XPG rs751402 T alleles appear to be exposed to higher risks for other types of cancer as well, including hepatocellular carcinoma (25), breast cancer (26), salivary gland tumors (27) and oral squamous cell carcinoma (28). These similar observations call for delicate studies to investigate the possible molecular mechanism that links XPG polymorphism with cancer risk. Gene mutations in multiple biological pathways including DNA repair, have been reported to link XPG polymorphism with GC (29).
The DNA repair system plays an important role in maintaining DNA integrity and stability (30). Insufficient DNA repair capability in cells would increase DNA mutation accumulation and then the risk of carcinoma development. The NER pathway consists of 8 key genes – namely, XPA to XPG and ERCC1 (14). This pathway involves multiple processes in a defined order (31). First, the XPC protein works as a DNA damage sensor and XPA/XPE verifies the damage. The NER mechanism is initiated, and their proteins are recruited. Second, XPB and XPD proteins unravel the DNA double helix around the damage. Third, XPG cuts the DNA lesion on the 3’ side at the exact position, and then acts as a nonenzymatic scaffolding for subsequent 5’ incision by the XPF-ERCC1 complex (9). Finally, the DNA lesion–containing oligonucleotide is removed, and the gap is filled with a new oligonucleotide. Therefore, XPG is an indispensable part of the NER mechanism. Notably, the rs751402 gene is located in the promoter region of XPG, and its variance controls the protein expression, thus influencing the DNA damage repair capacity (25). The rs751402 polymorphism was associated with XPG transcript regulation (11) and RNA polymerase II (32), which might be the biological mechanism of higher GC risk conferred by rs751402 mutation.
There were some limitations in our study. First, all of the 9 identified studies were conducted in China. Through database searches, we even failed to obtain an exploratory investigation in other ethnic groups. So these results should be treated with caution, because they cannot be directly extrapolated to other ethnicities. Second, we could not perform stratification analyses based on patients’ sex, GC subtype of Lauren classification and TNM stage, because relevant information from the identified 9 studies was unavailable. Only Hua et al (2016) (14) performed stratified analysis based on sex and TNM stages. However, they did not find any significant relationship between any variant and GC risk in subgroup analyses. Although 4 studies (13) reported the numbers of individuals with diffuse-type GC and intestinal-type GC according to the Lauren classification, only the study by Duan et al (13) investigated any relationship of the diffuse-type GC risk with rs751402 (CC + CT) genotype (OR = 1.44, 95% CI, 1.02-2.02). Two studies (14, 20) made stratification analysis based on age. Hua et al (14) did not find a relationship between rs751402 and GC in subjects <58 or >58 years old. Zhou et al (20) observed that rs751402 T allele and TT genotype enhanced GC risk in individuals ≤61 years old (OR = 1.30 and 1.77, 95% CI, 1.00-1.76 and 1.12-3.30, respectively), but not in the >61-year-old subgroup. Because age was categorized differently in the 2 studies, we could not utilize these data and perform analyses stratified by age.
Finally, several studies suggested that genetic effects of rs751402 mutation on increased GC susceptibility might be enhanced by environmental factors including H. pylori infection, smoking and drinking, or might be interacting with other XPG polymorphisms such as rs2296147 C>T and rs873601 G>A (13, 14). We were unable to validate these observations in the present study due to insufficient data.
Conclusions
In conclusion, this meta-analysis indicates that the XPG rs751402 polymorphism is likely to be a genetic risk factor for GC in the Chinese population. However, taking its limitations into consideration, additional studies, especially ones conducted in other populations, are warranted to verify our findings.
Footnotes
Disclosures
Financial support: This project was funded by the Research Project of Hefei Fourth People’s Hospital (2017003).
Conflict of interest: No conflict of interest existed.