
Abstract
Hepatocellular carcinoma (HCC) has one of the highest death rates of any cancer in the world, and its incidence is increasing worldwide. Early-stage diagnosis of HCC is thus crucial for medical treatment. Detection of tumor biomarkers is one of the main methods for the early diagnosis of HCC. At present, α-fetoprotein (AFP) is the most practical serum biomarker for HCC diagnosis. However, the diagnostic accuracy of HCC with serum AFP exhibits both sensitivity and specificity far below satisfaction, especially with small sizes of HCC. As a result, the discovery of new biomarkers and/or their combination to enhance both the sensitivity and specificity for laboratory diagnosis of HCC is a crucial goal. With the development of new technology and advances in research, a number of new and specific biomarkers of HCC have been discovered. These biomarkers and their applications for the diagnosis, treatment monitoring and prognosis prediction of HCC, are reviewed in this article.
Introduction
As reported by the World Health Organization, nearly 1 million people die from liver failure or liver cancer caused by HBV infection every year. Among cancer-caused deaths in China, hepatomas account for a third of deaths in males and are the second leading cause in females (1). Hepatocellular carcinoma (HCC) represents more than 90% of primary liver cancers, and is thus the fifth most prevalent cancer in the word and the third leading cause of cancer-related mortality. Furthermore, its incidence is increasing in various countries (2-4). Clearly, in the early diagnosis, treatment monitoring and prognosis predictions of HCC, the detection of cancer biomarkers has a pivotal role to play. It is the subject of this review.
Biomarkers in the detection of HCC
Classical biomarkers in the diagnosis of HCC
α-Fetoprotein
α-Fetoprotein (AFP) is the most practical serum biomarker for HCC diagnosis. However, a meta-analysis of AFP for HCC surveillance found that it displayed a sensitivity of 39%-65% and a specificity of 76%-94% (5), indicating its unsatisfactory role in HCC diagnosis. Serum AFP can be elevated in patients with HCC, gastric cancer, lung cancer, pancreatic cancer, bile duct cancer, testicular cancer or other diseases under pathological conditions (6). It was reported that serum AFP can also be increased in patients with cirrhosis (11%-47%) and chronic hepatitis (15%-58%), further evidence of the low specificity of serum AFP for HCC diagnosis. Moreover, in 80% of HCC patients bearing small sizes of tumor, serum AFP was not increased significantly; the sensitivity of AFP was 52% and 25% for HCC patients with tumors >3 cm or <3 cm in diameter, respectively (7-9).
Lens culinaris agglutinin-reactive AFP
Lens culinaris agglutinin-reactive AFP (AFP-L3) is one of the AFP isoforms, and the percentage ratio of serum AFP-L3 to total AFP has been used as an index for early diagnosis of HCC. AFP-L3 is somewhat unique in HCC cells; previous research has shown that serum levels of AFP-L3 of HCC patients were higher than those of patients with chronic liver diseases. The sensitivity and specificity of this index for the diagnosis of HCC were 72% and 97%, respectively (10). An increase of AFP-L3 can be detected in the sera of approximately one third of patients with small HCC (<3 cm) when cutoff levels are set at 10%-15%. At higher cutoff levels of >15%, the percentage ratio of AFP-L3 to total AFP displays a sensitivity of 75%-97% and specificity of 90%-92% for the diagnosis of HCC (11, 12). In fact, AFP-L3 was formally approved as a biomarker for the detection of HCC by the US Food and Drug Administration in 2005. However, some reports have not been consistent about the significance of AFP-L3 in the diagnosis of HCC. A meta-analysis of data from 12 articles indicated that AFP-L3 had better specificity but lower sensitivity than AFP for the diagnosis of HCC (13). Our own results (14) showed a sensitivity, specificity and area under the curve (AUC) from receiver operating characteristic (ROC) curve analysis for the diagnosis of HCC with AFP-L3 to be 60%, 91% and 0.745, when the cutoff level for the percentage was set at 15%, and 62%, 93% and 0.816 for small HCC with negative AFP, respectively (15). These results with 15% as the threshold indicated that AFP-L3 is a promising biomarker superior to AFP for the diagnosis of HCC, especially for HCC with low levels of AFP and small sizes of carcinoma.
Des-γ-carboxyprothrombin
Des-γ-carboxyprothrombin (DCP) is an abnormal prothrombin protein, also known as prothrombin induced by vitamin K absence II. It is produced as a result of an acquired defect in the posttranslational carboxylation of the prothrombin precursor in malignant cells; the gene responsible for this carboxylation is γ-carboxylase (16). In several studies, serum DCP was found to display poor diagnostic sensitivity (48%-62%), but good specificity (81%-98%) for HCC (16, 17). A study comparing the performance of AFP, DCP and AFP-L3 in the diagnosis of HCC found that DCP was significantly better than the other biomarkers, with sensitivity and specificity up to 86% and 93% to differentiate HCC from cirrhosis (18). DCP has been approved by Japan, South Korea and India as an effective biomarker for the diagnosis of liver cancer (19), especially for judging intrahepatic metastasis and prognosis (20, 21). However, there have been conflicting results when the tumor size was less than 2 cm or 3 cm, because the diagnostic sensitivity in those cases was only 47% or 62%, respectively. Meanwhile, the diagnostic sensitivity of AFP under the same conditions was 65% or 67% (22). These results indicated that DCP was not superior to AFP in the early detection of HCC, and not even a useful biomarker for the diagnosis of HCC (22, 23). We found that the sensitivity and specificity with DCP were just 44% and 91% for the diagnosis of HCC, showing no superiority to AFP (14). For small HCC with negative AFP, however, the diagnostic sensitivity and specificity of DCP were 56% and 93%, respectively (15). Therefore, DCP still has some clinical significance in the diagnosis of small HCC with negative AFP.
New biomarkers in the detection of HCC
An ideal biomarker of HCC would have high specificity to distinguish among liver cirrhosis, hepatitis and HCC, have high sensitivity for the early diagnosis of HCC, and be easily quantified with noninvasive specimens. In recent years, with the development of genomics and proteomics, some new representative biomarkers have been discovered, and these are reviewed in this paper.
Golgi glycoprotein 73
Golgi glycoprotein 73 (GP73) is a transmembrane Golgi glycoprotein with 400 amino acid residues (24). Serum GP73 was elevated significantly in HCC patients (25). Although the levels of GP73 in hepatitis and fatty liver were also somewhat elevated (26, 27), they were much lower than in patients with HCC (28), indicating that GP73 may be a more valuable biomarker than AFP for early diagnosis of HCC (29, 30). However, the potential advantages of GP73 over AFP in diagnosis of HCC remain controversial because there have been some reports that have shown the sensitivity and specificity of GP73 for diagnosis of HCC to be by no means an improvement over those of AFP (31, 32), and a few studies even indicated that serum GP73 was not related to HCC (33). Our results supported both the significance of serum GP73 in the detection of HCC and its role as an auxiliary diagnostic biomarker of HCC bearing low levels of AFP and/or small sizes. The sensitivity and specificity of serum GP73 for HCC were 72% and 95%, respectively, indicating its superiority to the respective 52% and 92% with AFP (14). The sensitivity and specificity of GP73 were 72% and 94% for the diagnosis of small HCC with negative AFP, supporting the idea that it is a superior biomarker to aid in the diagnosis of small HCC (15).
Glypican 3
Glypican 3 (GPC3) is a cell-surface heparan proteoglycan which is not expressed in healthy adult livers (21); its serum level in HCC is significantly higher than those in other benign liver diseases (34-36). Currently, the sensitivity of GPC3 for the diagnosis of HCC has been found to range from 36% to 65%, and its specificity ranges from 65% to 100% (21, 37-40). Furthermore, GPC3 is more sensitive than AFP for the detection of smaller HCC (38, 41). GPC3 may be useful for early diagnosis of HCC and the diagnosis of malignant and benign liver tumors (21, 39). However, there have also been some reports indicating that GPC3 as a biomarker was not superior to AFP, and even not useful for the diagnosis of HCC (42). We found the levels and positive rates of GPC3 for HCC were significantly higher than those for other diseases, indicating that GPC3 had a certain clinical significance in the diagnosis of HCC. Unfortunately, its diagnostic sensitivity and specificity were just 42% and 96%, showing no superiority to AFP (14). Fortunately, for small HCC with negative AFP, the diagnostic sensitivity and specificity of GPC3 were 52% and 98%, supporting its diagnostic value for small HCC with negative AFP (15).
Transforming growth factor-β1
Transforming growth factor-β1 (TGF-β1) is a cytokine with multiple biological functions. It has a vital role in the regulation of growth and differentiation of normal and transformed cells, angiogenesis, extracellular matrix formation, immunosuppression and carcinogenesis (16, 43). It has been reported that TGF-β1 and TGF-β1 mRNA levels were significantly higher in the serum of patients with HCC compared with patients with nonmalignant chronic liver diseases and a healthy control group (16, 43, 44). Using a cutoff level of 1.2 μg/L for the diagnosis of HCC, the sensitivity was 89% and the specificity was 94% (43). Similarly, there have also been some reports indicating that TGF-β1 has a sensitivity of 78% and a specificity of 29% for the diagnosis of HCC with a threshold of 64.3 ng/mL (45). This biomarker is up-regulated in extrahepatic tumors, wounds, angiogenesis and fibrosis tissues, indicating a lack of disease specificity of TGF-β1 (44, 46).
Insulin-like growth factor-II
Insulin-like growth factor-II (IGF-II) is a kind of mitogenic polypeptide that can stimulate cell proliferation and the growth and differentiation of tissues and organs. Circulating free IGF-II levels were significantly higher in HCC than those in chronic liver disease. It is abnormally expressed during HCC development (47). These clinical studies have suggested that the detection of IGF-II can aid in the diagnosis and prognosis prediction of HCC, but few diagnosis data with clinical specimens were reported.
Hepatocyte growth factor
Hepatocyte growth factor (HGF) is a kind of polypeptide growth factor which is produced by many kinds of human organs and has many kinds of biological activity. In a prospective study, blood samples were collected from 99 patients with chronic hepatitis, cirrhosis and HCC. Serum HGF levels were significantly elevated in HCC patients compared with patients with cirrhosis or chronic hepatitis but no malignancy (48). All patients with a serum HGF concentration of >0.6 ng/mL had HCC, irrespective of their AFP or DCP levels. Furthermore, the detection of HGF has a certain significance for early diagnosis, observation of curative effects and prognosis predictions of HCC (49, 50). It has been used as a prognostic marker in HCC to predict early tumor recurrence and metastasis. However, in addition to liver cancer, there are other nonmalignant diseases causing an increase in serum HGF levels, including esophageal squamous cell carcinoma, lymphoma, coronary syndrome (51), aortic dissection, pulmonary embolism (52), cerebral infarction and sepsis (53-55). Therefore, further studies are needed to confirm that a higher level of HGF is associated with inflammatory changes or malignancy.
Vascular endothelial growth factor
Vascular endothelial growth factor (VEGF) is an endothelial cell mitogen that promotes neovascularization and endothelial cell proliferation. Serum VEGF levels in HCC patients were significantly higher compared with control individuals, and were correlated with venous invasion and advanced tumor stage (56). Furthermore, the expression of VEGF in HCC tissues was related to invasiveness and metastasis of HCC (57, 58). High serum levels of VEGF indicate poor HCC prognosis (59). Therefore, it can be used as a prognostic marker in HCC to predict the development of HCC, recurrence and metastasis. VEGF is also related to tumor growth and may also be increased in other cancers, and thus its specificity for the diagnosis of HCC is not sufficient and its value for early diagnosis of HCC is also unclear (60).
Heat shock protein
Serum heat shock proteins (HSPs) are potential tumor markers for HCC evaluation. They are stress-induced proteins that are expressed under nonspecific stress stimuli, including carcinogenesis (61). In particular, HSP70 has been identified as a potentially sensitive marker to differentiate early HCC from precancerous lesions (62). In HBV-infected patients, the expression levels of GRP78, GRP94 or HSP90 have been significantly correlated with vascular invasion and intrahepatic metastasis. HSP27 has been detected in 90% of HCC patients' sera and 2 HBV patients' sera, but in none of normal sera (63). The optimized diagnostic threshold for HSP27 for HCC was 456.5 pg/mL, giving a sensitivity of 70% and a specificity of 73%, with an AUC of 0.749 (64).
Squamous cell carcinoma antigen
Squamous cell carcinoma antigen (SCCA) is a member of the serpin (serine protease inhibitor) family, it is physiologically active in a layer of the squamous epithelium and its overexpression has been associated with tumorigenesis (65). It has also been reported to be overexpressed in HCC tissue and in sera of HCC patients (66). Further investigation of serum SCCA levels for diagnosis of HCC using a similar method gave sensitivities ranging from 18% to 84% and specificities ranging from 27% to 73% (66-70). While serum SCCA-IgM may prove to be a more promising biomarker for HCC diagnosis, using an ELISA technique, SCCA-IgM produces sensitivities ranging from 52% to 89% and specificities from 49% to 100% (67, 71-74).
Dickkopf-related protein 1
Dickkopf-related protein 1 (DKK1) is a promising diagnostic biomarker for HCC, especially for patients with AFP-negative and early stage HCC (75). In addition, serum levels of DKK1 decrease after surgery, indicating that this protein may be a useful surveillance marker to assess the therapeutic response of HCC patients. Nevertheless, DKK1 seems to be not very specific for HCC, because a recent study reported that serum DKK1 was also elevated in patients with intrahepatic cholangiocarcinoma (76, 77), so its predictive ability for the diagnosis of HCC needs to be further investigated.
Osteopontin
Osteopontin (OPN) is an integrin-binding glycophospho-protein expressed in several cell types – e.g., in particular transformed malignant epithelial cells – and is involved in many cellular functions, such as regulating the survival, migration, invasion and metastasis of tumor cells (78). In cancer, overexpression of OPN has been widely documented (79). OPN plasma levels were significantly elevated in HCC patients compared with in those with chronic liver diseases. Its specificity and sensitivity were 92% and 26% for the diagnosis of HCC, and its expression level was independent of the concentration of AFP in serum (80, 81). The correlation between the OPN and AFP levels was not significant. Similarly, increased plasma level of OPN has been suggested as a promising biomarker for early stages of liver disease (82).
Circulating genetic and cell biomarkers
Circulating RNA in the blood of HCC patients, such as AFP mRNA, TGF-β1 mRNA and IGF-II mRNA, have been used to monitor the distant metastasis or postoperative recurrence of HCC (83). MicroRNAs (such as miR-21, miR-122 and miR-223) steadily expressed in serum and urine can be new noninvasive biomarkers for early detection and prognosis of HCC (84). In a recent study, regardless of the stage of HCC, a miRNA panel that included miR-122, miR-192, miR-21, miR-223, miR-26a, and miR-801 effectively identified patients with HCC from healthy individuals and those with cirrhosis or chronic HBV (AUC = 0.89 with a specificity of 84% and a sensitivity of 82% for the validation set) (85). Moreover, circulating tumor cells (CTCs) can reflect tumor aggressiveness and serve as promising candidates for predicting tumor recurrence and metastasis (86). Sun et al reported that epithelial cell adhesion molecule (EpCAM)–positive CTCs may serve as a prognostic marker in HCC after curative resection (87). But their clinical effectiveness still needs to be evaluated. Further, circulating cell-free DNA (cfDNA) is a new tool for the detection and surveillance of many cancers, including HCC (88, 89). Qualitative and quantitative analyses of cfDNA are potential methods for the detection of HCC. Many studies have evaluated these approaches, but the results have been variable. The results from a meta-analysis suggested that cfDNA has potential value for HCC diagnosis (90). However, it could not be recommended for independent use, because the assays of cfDNA lacked robustness. After combining with AFP, the diagnostic performance of cfDNA is improved. Further investigation with more clinical data is needed (90).
Future prospects of biomarkers in the detection of HCC
Combined tests of biomarkers
To improve their diagnostic sensitivity and specificity, combined tests of several related biomarkers are often applied in clinical practice. The combined detection of AFP, AFP-L3 and DCP improves their diagnostic value for HCC, with a sensitivity of 94% and specificity of 86% (91). The combination of DCP and AFP increases the sensitivity and specificity for the diagnosis of HCC to 61% and 83%, respectively (22). In addition, the combined detection of AFP with GGT, AFP with AFU and AFP with GPC3 all improves their diagnostic value for HCC (92-94). In our own study of 50 patients with HCC, 60 patients with non-HCC digestive system disorders and 40 healthy controls (14), the levels of 8 biomarkers, including GP73, DCP, GPC3, AFP-L3, AFP, CA199, FER and CEA, were detected to reveal that combined tests of GP73 with DCP, GPC3 or AFP-L3 all improved their sensitivity and specificity for the diagnosis of HCC. Notably, the combination of 8 biomarkers together increased their sensitivity and specificity to 82% and 91% (Tab. I and Fig. 1A). In addition, in 50 patients with small HCC (a single lesion ≤3 cm without vascular involvement or metastasis and negative serum “AFP), 60 patients with non-HCC digestive system disorders and 40 healthy controls (15), the detection of their serum biomarkers revealed that the combined detection of GP73 and other tumor biomarkers effectively reduced the rate of missed diagnosis (Tab. I and Fig. 1B).
Comparison of diagnostic values for individual and combined tests of GP73 and other biomarkers for diagnosis of hepatocellular carcinoma (HCC) and small HCC
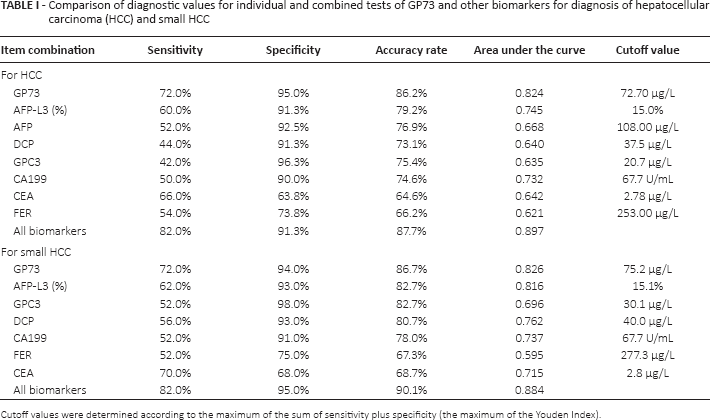
Cutoff values were determined according to the maximum of the sum of sensitivity plus specificity (the maximum of the Youden Index).
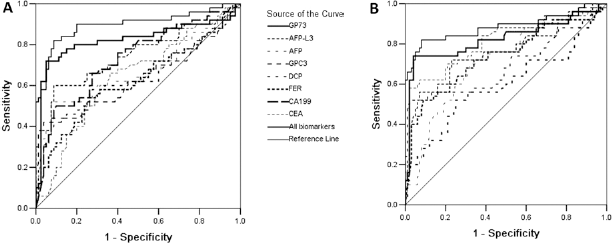
Receiver operating characteristic (ROC) curve analysis of individual and combined biomarkers for diagnosis of hepatocellular carcinoma (HCC) (
Although the combined test of multiple biomarkers effectively improves the diagnostic sensitivity and specificity of liver cancer, the relationship between combined detection and the early diagnosis and prognosis of HCC remains to be further studied.
Proteomic analysis of biomarkers for the detection of HCC
In the past 10 years, proteomics technology has been developed and widely used for the detection of new biomarkers for HCC. Through hepatic tissue protein mass spectrometry analysis, the pathogenesis of HCC can be better understood at different stages of disease. Seven groups of proteins were selected to make up an artificial neural network model, and evaluate 435 serum samples of HCC using surface-enhanced laser desorption ionization time of flight mass spectrometry; the sensitivity and specificity reached to 84% and 81%, respectively. Proteomic analysis of biomarkers is considered to be a new and accurate method for the diagnosis of HCC (95). However, to date, few such candidate molecules have been validated in clinical practice.
In addition to proteomics, there has been some progress in defining the serum biomarker spectrum in the early stage of liver cancer by using bio-photon technology to mine medical information (such as vibrational spectroscopy). Fourier transform infrared spectroscopy, as a high-throughput, rapid and minimally invasive method, was used to distinguish liver cirrhosis and HCC patients successfully by Zhang et al (96). Notably, such techniques have low cost and high efficiency. With the continuous progress of methods and technologies, there will be more and more effective tools in future to realize the goals of early diagnosis, early treatment and good prognosis of liver cancer.
Biomarkers of liver cancer with targeted therapy and personalized therapy
Molecular targeted therapy of liver cancer refers to treatment aimed at cell signaling pathways and/or other similar biological pathways involved in the development of liver cancer; its advantages of high specificity and efficacy open up a new direction in the treatment of advanced liver cancer (97, 98). The targets of molecular targeted therapy of liver cancer include epidermal growth factor receptor, VEGF receptor, platelet-derived growth factor receptors and the signaling pathways of Ras/R//MEI//ERK and PDK/AKT/mTOR, etc (49, 99). Based on the inhibition of functions of the above-mentioned targets, some targeted therapy drugs have been developed to prevent the growth of liver cancer, including sorafenib and bevacizumab. Sorafenib inhibited VEGF receptor and platelet-derived growth factor receptor, and targeted the tumor cell and tumor vasculature (100-102). Bevacizumab is a drug that is anti-VEGF and its receptor. Sorafenib is the first and only molecule that can prolong survival of patients with advanced liver cancer, as confirmed by global phase III international multicenter randomized controlled trials (101). Targeted therapy drugs have some side effects. For instance, sorafenib has some liver toxicity, and requires the liver function of any patient being treated to be Child-Pugh A grade; thus the dynamic changes of liver function need observing when sorafenib is used.
Personalized therapy of HCC based on genotyping is not yet mature. In clinical practice, it is desirable to observe different biological markers in different clinical stages of patients through studies of gene expression profiling, and then to formulate individualized treatment programs according to molecular typing or genotyping for the different clinical stages of HCC. The molecular features of HCC can be classified by profiles of gene expression, miRNA expression, genome and/or proteome information. Several laboratories are decoding the molecular characterization and molecular classification of HCC based on different whole genome sequencing or microarray platform technologies (103). Studies have suggested that patients with lower expression of miRNA-26 are more suitable for postoperative adjuvant therapy with interferon, but this also needs validation through prospective research (104).
The telomere length of patients infected with HBV may be related to the risk and prognosis of HCC (105); inactivated mutant of ARID2 as a tumor suppressor gene was detected in liver cancer subtypes infected by HCV (106). Based on the presence of individual differences and genetic polymorphisms, actively looking for molecular biomarkers that can predict different molecular targeted drug efficacies and implementing individualized treatments of specific HCC patients are the future direction of the treatment and diagnosis of HCC.
Conclusions
HCC is a complex disease with multiple pathogenic mechanisms caused by a variety of risk factors, and it is thus difficult to characterize HCC with a single biomarker. The screening and optimization of combined tests of tumor biomarkers may be more valuable for the early diagnosis, staging and prognosis prediction of HCC. With the development of genomics and proteomics, there will be more new biomarkers to diagnose different stages of HCC. In the near future, the identification of new noninvasive biomarkers for early diagnosis and personalized treatment of HCC will be one of the most promising fields of biomarker research.
Footnotes
Financial support: This work was supported by the Science and Technology Project of Qinhuangdao, China (201602A108).
Conflict of interest: None of the authors has any financial interest related to this study to disclose.