
Abstract
Background:
The most important adverse prognostic factor for laryngeal squamous cell carcinoma (LSCC) is the presence of cervical lymph node metastases. The supraglottic area of the larynx is richly supplied with lymphatics, and 25%-75% of supraglottic carcinomas metastasize in neck lymph nodes. Cortactin is a multidomain protein related to actin cytoskeleton regulation, podosome and lamellipodia formation, integrin signaling, axon guidance and extracellular matrix degradation. Cortactin is involved in metastasis formation because of its role in cell mobility. The present study focused mainly on the role of cortactin and phosphorylated cortactin (residues tyr421 and tyr466) expression and subcellular localization in primary supraglottic LSCCs and their cervical lymph node metastases.
Methods:
The immunohistochemical expression of cortactin, p-Y466-cortactin and p-Y421-cortactin was assessed in 38 primary supraglottic LSCCs and 10 lymph node metastases. The statistical approach included bootstrapping analysis.
Results:
Despite a significantly higher expression of cortactin in carcinoma cells than in adjacent normal laryngeal mucosa, no associations emerged between prognosis and the expression of cortactin or its isoforms in supraglottic LSCC. Statistical analysis found cortactin expression higher in less-differentiated LSCCs (p = 0.03). A significant direct correlation was found between cortactin and p-Y466-cortactin levels (p = 0.031), and between p-Y466-cortactin and p-Y421-cortactin levels (p = 0.001).
Conclusions:
Cortactin expression in carcinoma cells and its known involvement in the EGFR pathway suggest a role for this protein as a target for LSCC therapy. Further prospective studies are needed to investigate the potential of cortactin, p-Y466-cortactin and p-Y421-cortactin expression as markers of response to treatment (particularly EGFR-directed agents) in LSCC.
Introduction
The Surveillance Epidemiology and End Results (SEER) Cancer Statistics Review of global prevalence counts for invasive cancers alone (1975-2008) concluded that laryngeal squamous cell carcinoma (LSCC) was the 15th most common human malignancy in the United States (1). The European Cancer Observatory 2008 data for the European Union (with 27 member states) indicated that LSCC ranked as the 21st most common human malignancy (1).
The most important adverse prognostic factor for LSCC is the presence of cervical lymph node metastases. It has been well established that the development of cervical metastases negatively impacts both regional control and survival. The laryngeal supraglottic area is richly supplied with lymphatics, and when all stages are considered, carcinomas of the supraglottic region metastasize in 25%-75% of cases (2). Supraglottic carcinoma is believed to differ from the disease originating in the glottis, in terms of invasive and metastatic potential and lymph drainage.
It is crucial to investigate the clinicopathological parameters and biomarkers that might reflect the biological tendency of primary LSCCs (particularly in the supraglottis) to develop cervical lymph node metastases. The events associated with local invasion, and with regional and distant metastasization by an epithelial tumor like LSCC include loss of adhesion to surrounding tumor cells and basement membrane, production of enzymes and mediators that facilitate the incursion of malignant cells into the subjacent connective tissue, attachment to extracellular membrane molecules, neovascularization, entry and exit of carcinoma cells to and from the circulation via attachment to endothelial cell ligands, and the repetition of this cascade at a metastatic site (3).
Cortactin is a ubiquitous multidomain protein that is related to the regulation of the actin cytoskeleton, podosome and lamellipodia formation, integrin signaling, axon guidance, and degradation of the extracellular matrix (ECM) (4). It is involved in tumor progression and the formation of metastases because of its role in cell mobility (5, 6). The cortactin locus CTTN is located in the 11q13 region, which is frequently amplified in human cancer. The highest frequencies of amplification have been found in adenocarcinoma of the breast or colon (7), and in squamous cell carcinoma of the esophagus or head and neck region (8). Amplification of 11q13 has often been associated with a poor prognosis, a higher pathological stage, lymph node and distant metastases and shorter survival (4). Cortactin interacts with numerous binding partners, and its activity is also regulated by several posttranslational modifications (4, 9). Cortactin is phosphorylated at tyrosine residues in response to signaling downstream by various upstream receptors, including integrin- and cadherin-adhesion receptors and growth factor receptors. Several nonreceptor tyrosine kinases have been implicated in the phosphorylation of cortactin, including Src family kinases, ABL family kinases, FER and Syk (9). Interestingly, tyrosine phosphorylation of cortactin occurs as a gradual process, started by tyrosine 421 (tyr421), then continued by tyrosine 466 (tyr466). How tyrosine phosphorylation affects cortactin function is a highly complex issue, reflecting the array of diverse physiological processes in which cortactin participates. There is a positive correlation, however, between the level of cortactin phosphorylation and its ability to induce cell migration (5).
The primary aim of the present investigation was to study the immunohistochemical expression and subcellular localization of cortactin and phosphorylated cortactin (residues tyr421 and tyr466) in primary supraglottic LSCCs and their cervical lymph node metastases. A secondary aim was to see how cortactin and phosphorylated cortactins relate to the conventional clinicopathological parameters and prognosis for LSCC.
Materials and methods
Patients
The study was approved by our Otolaryngology Section’s in-house ethics committee. It was conducted in accordance with the principles of the Helsinki Declaration. Before undergoing surgery, all patients signed a detailed informed consent form.
The study concerned 38 consecutive cases of LSCC treated with primary surgery. As in the recommendations adopted for LSCC at our institution (10), all patients (29 men, 9 women; mean age 63.7 ± 7.5 years) had undergone microlaryngoscopy with laryngeal biopsy, upper aerodigestive tract endoscopy, neck ultrasonography (with or without fine needle aspiration cytology), head and neck contrast-enhanced computerized tomography (CT), and/or magnetic resonance imaging, chest X-ray and liver ultrasonography.
All patients underwent laryngeal surgery at the Otolaryngology Section of Padova University, with unilateral or bilateral cervical lymph node dissection in 31 cases. Pathological staging, and the characteristics of primaries and metastases warranted postoperative RT in 13 cases according to current guidelines. Table I provides details of patients’ clinicopathological features, partly based on the seventh edition of the TNM Classification of Malignant Tumors (11). No distant metastases (M) were detected at diagnosis. As previously reported (10), the clinical follow-up after treatment (adjustable to patients’ individual characteristics) was scheduled as follows: (i) once a month for the first year; (ii) every 2 months in the second year; (iii) every 3 months in the third year; (iv) every 4 months in the fourth year; (v) every 6 months in the fifth year; and (vi) every 12 months thereafter. Neck ultrasonography and chest X-rays were also performed at least yearly. Contrast-enhanced CT of the neck, total body positron emission tomography (PET-CT), chest CT and liver ultrasonography were repeated as necessary. The mean follow-up was 71.7 ± 40.4 months.
Cortactin, p-Y421-cortactin and p-Y466-cortactin expression vis-à-vis classical clinicopathological and prognostic variables in supraglottic LSCC
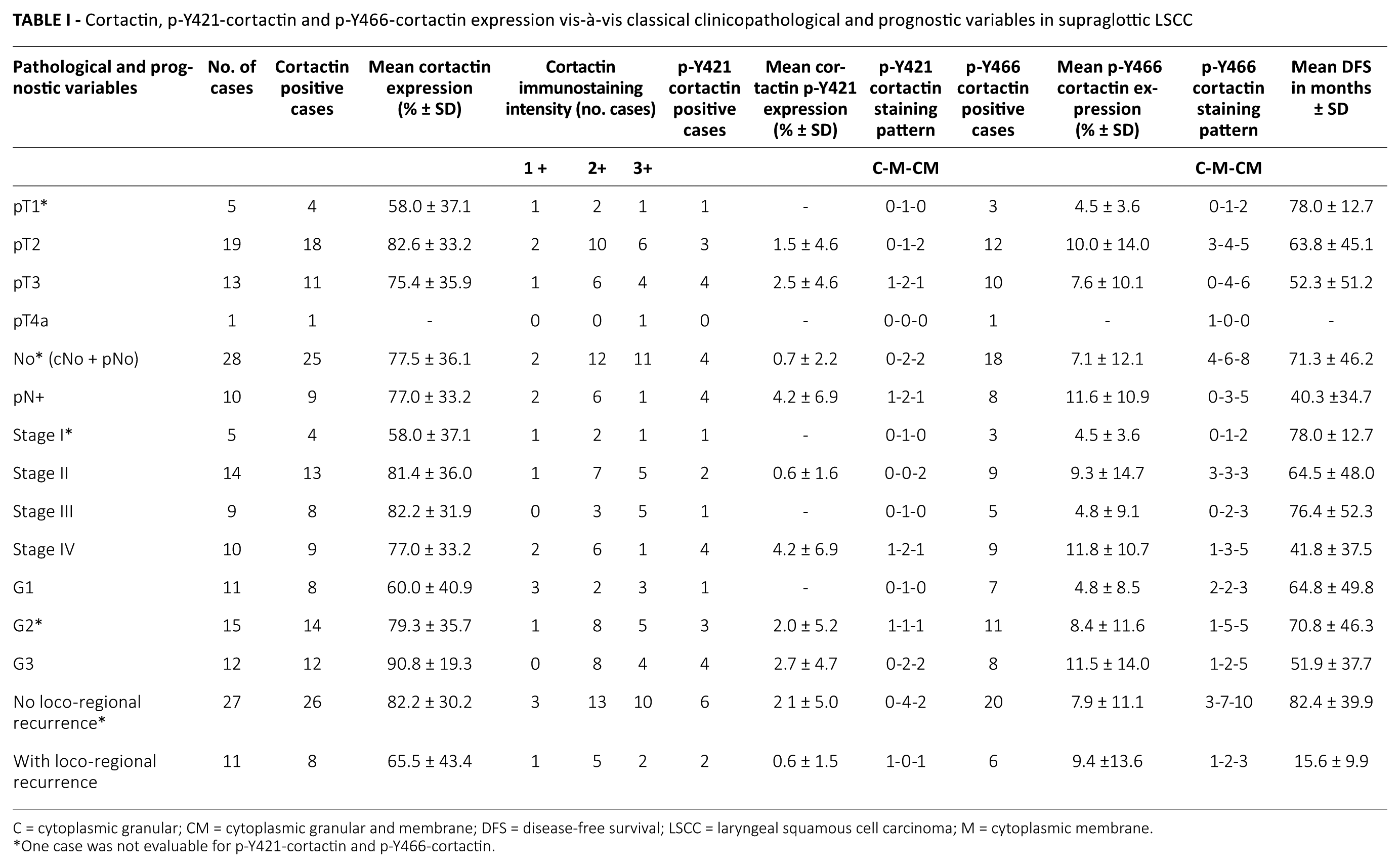
C = cytoplasmic granular; CM = cytoplasmic granular and membrane; DFS = disease-free survival; LSCC = laryngeal squamous cell carcinoma; M = cytoplasmic membrane.
One case was not evaluable for p-Y421-cortactin and p-Y466-cortactin.
Immunohistochemistry
Sections were obtained for immunohistochemical examination from 48 tissue blocks (38 primary supraglottic LSCCs and 10 lymph node metastases). Immunohistochemistry was performed on 4-μm-thick formalin-fixed and paraffin-embedded (FFPE) sections. Staining was done automatically (BondmaX; Menarini, Florence, Italy) using the Bond Polymer RefineDetection kit (Leica Microsystem, Wetzlar, Germany) with rabbit anti-cortactin antibody (monoclonal EP1922Y; working dilution 1:200, 30 minutes, citrate buffer; Abcam, Cambridge, UK), rabbit anti-phospho-Y466 cortactin (p-Y466 cortactin) antibody (polyclonal; working dilution 1:200, 30 minutes, citrate buffer; Abcam, Cambridge, UK) and rabbit anti-phospho-Y421 cortactin (p-Y421 cortactin) antibody (polyclonal; working dilution 1:100, 30 minutes, citrate buffer; Abcam, Cambridge, UK). Sections were then slightly counterstained with hematoxylin. Appropriate positive and negative controls were run concurrently.
In primary and metastatic carcinomas, the cytoplasmic expression of cortactin, p-Y466-cortactin and p-Y421-cortactin was scored jointly by 2 pathologists (S.B. and E.V.) given no clinical information about the cases involved. Cortactin cytoplasmic staining was scored quantitatively in terms of the percentage of positive cells; staining intensity was also judged as: 1+ = weak, 2+ = moderate, and 3+ = strong. The percentage of positive cells was also used to assess p-Y421-cortactin and p-Y466-cortactin expression in primary and metastatic carcinomas. The subcellular pattern of p-Y466-cortactin and p-Y421-cortactin location was analyzed in primary LSCC.
Statistical analysis
The statistical analyses were run using Fisher’s exact test, the Mann-Whitney U-test and the Kruskal-Wallis test, as appropriate. Spearman’s rank correlation was used to assess the relationships between the levels of cortactin, p-Y466-cortactin and p-Y421-cortactin.
The log-rank test and Cox’s regression model were used to analyze disease-free survival (DFS) in months, after stratifying patients in light of the pathological and immunohistochemical variables considered.
The principle of bootstrapping is to generate a large amount of samples by resampling the original data with replacement (12, 13). In our case, for selected variables (cortactin expression and p-Y466-cortactin expression in primary LSCC) we performed the F-test statistics.
A p value <0.05 was considered significant. The Stata™ 8.1 (Stata Corp, College Station, TX, USA) statistical package was used for all analyses.
Results
Patients’ clinical outcomes
Twenty-seven of the 38 patients with supraglottic LSCC experienced no disease recurrence after surgery, while 11 relapsed after a mean 15.6 ± 9.9 months.
Fisher’s exact test ruled out any significant differences in the distributions for pT (p = 1.00), grade (p = 0.69), lymph node status (N0/N+) (p = 0.11), or stage grouping (p = 0.54), between the 2 subgroups of patients with and without locoregional carcinoma recurrences. The log-rank test showed a significant difference in DFS (in months) when patients were stratified by lymph node status (N0/N+) (p = 0.05), but not if they were stratified by pT (p = 0.90), pathological grade (p = 0.51) or stage (p = 0.30).
Cortactin expression and pathological and prognostic features of supraglottic LSCC
While cortactin staining was limited (1+) in the cytoplasm of the normal laryngeal epithelium, it was stronger (2+ or 3+) in most of the carcinoma cells (Tab. I). Cortactin expression was also assessed in both nonmetastatic and metastatic lymph nodes obtained from the same series of patients with LSCC. Cortactin staining was found in the cytoplasm of the germinal centers of nonmetastatic lymph nodes, and it was always intense (+3) in the cytoplasm of carcinoma cells in the metastases.
Thirty-four of the 38 supraglottic LSCCs were immunohistochemically cortactin-positive (Fig. 1A-C), while 4 showed no cortactin immunoreactivity. The mean cortactin expression was 77.4% ±35.4% (median 100%). In the 34 cortactin-positive cases, staining intensity was classified as 2+ in 18 cases, 3+ in 12, and 1+ in 4. Nine of the 10 lymph node metastases were cortactin-positive (mean expression 85% ± 32.0%, median 100%).
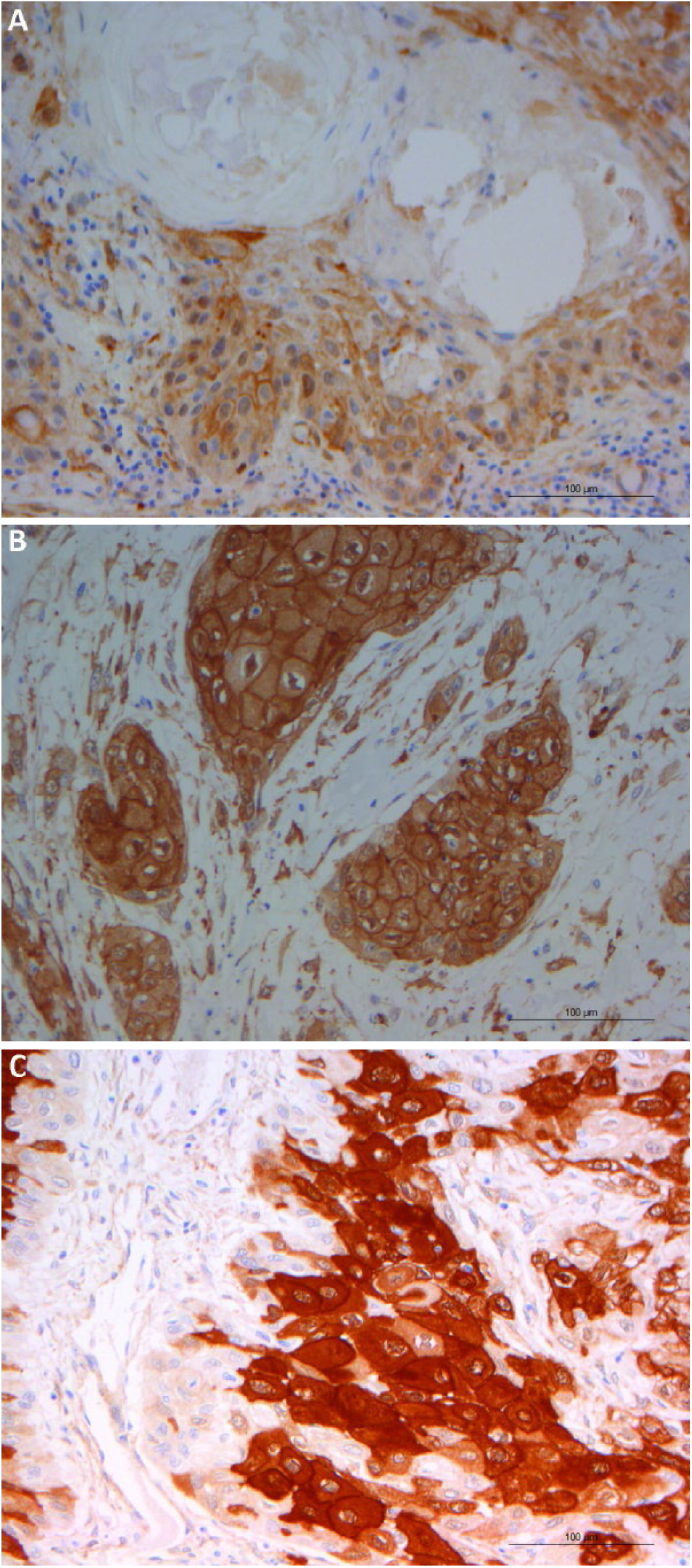
Cortactin expression in laryngeal squamous cell carcinoma (LSCC) by pathological grade: (
The Mann-Whitney U-test found significant differences in cortactin expression between the LSCC cases stratified by grade (G1 vs. G2-3, p = 0.03) (Fig. 1A-C), but not by pT (p = 0.82), N status (p = 0.60), stage (p = 0.16) or disease relapse after treatment (p = 0.20). Cox’s regression model revealed no significant differences in DFS (in months) when patients were distributed by cortactin expression in their LSCC (p = 0.16; hazard ratio [HR] = 0.98; 95% confidence interval [CI], 0.97-1.0). The Mann-Whitney U-test disclosed a significant difference in cortactin immunostaining intensity when patients were distributed by pathological grade (p = 0.037) but not by pT (p = 0.16), lymph node status (p = 0.52), stage (p = 0.16) or disease recurrence (p = 0.20). Cox’s regression model ruled out any significant differences in DFS when patients were distributed by cortactin-staining intensity (p = 0.60; HR = 0.75; 95% CI, 0.26-2.19).
For pN+ patients, statistical analysis (Mann-Whitney U-test) showed no significant differences for cortactin expression in lymph node metastases when patients were distributed by pT (p = 0.13), grade (p = 0.19), stage (p = 0.61) or disease relapse (p = 0.88) (Tab. II). In this same subcohort, Cox’s regression model revealed no significant differences in DFS when patients were distributed by cortactin expression in lymph node metastases (p = 0.24; HR = 0.98; 95% CI, 0.95-1.01).
Cortactin, p-Y421-cortactin and p-Y466-cortactin expression in lymph node metastases (n = 10) vis-à-vis classical pathological and prognostic variables
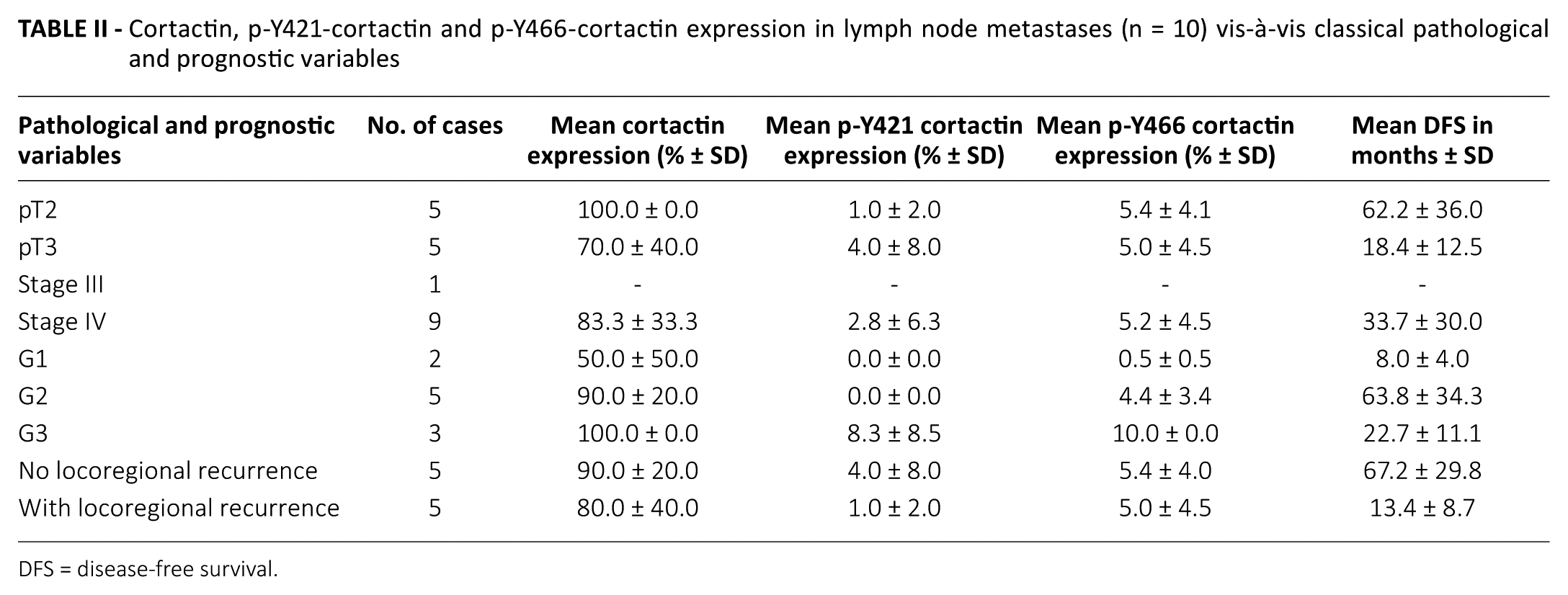
DFS = disease-free survival.
Phosphorylated cortactin expression and pathological and prognostic features of LSCC
In the normal tissue, p-Y466-cortactin weakly stained the cytoplasmic membrane (1+), and moderately stained the finely granular cytoplasm (2+) of the basal compartment (Tab. I). It showed the same subcellular staining pattern in the carcinoma cells, but with a higher intensity (3+) (Fig. 2A). In the normal laryngeal tissue, p-Y421-cortactin showed weak (1+) nuclear staining confined to the basal compartment, while immunostaining (2+) in the carcinoma cells was mainly cytoplasmic and membranous (Fig. 2B). The expression of pY421 and pY466 p-cortactin was also assessed in nonmetastatic and metastatic lymph nodes. In nonmetastatic lymph nodes, both p-Y466- and p-Y421-cortactin showed cytoplasmic staining in germinal center cells, and nuclear staining in small lymphocytes; in metastatic lymph nodes, the neoplastic cells showed strong (3+) cytoplasmic and membranous immunostaining (Fig. 2C, D).
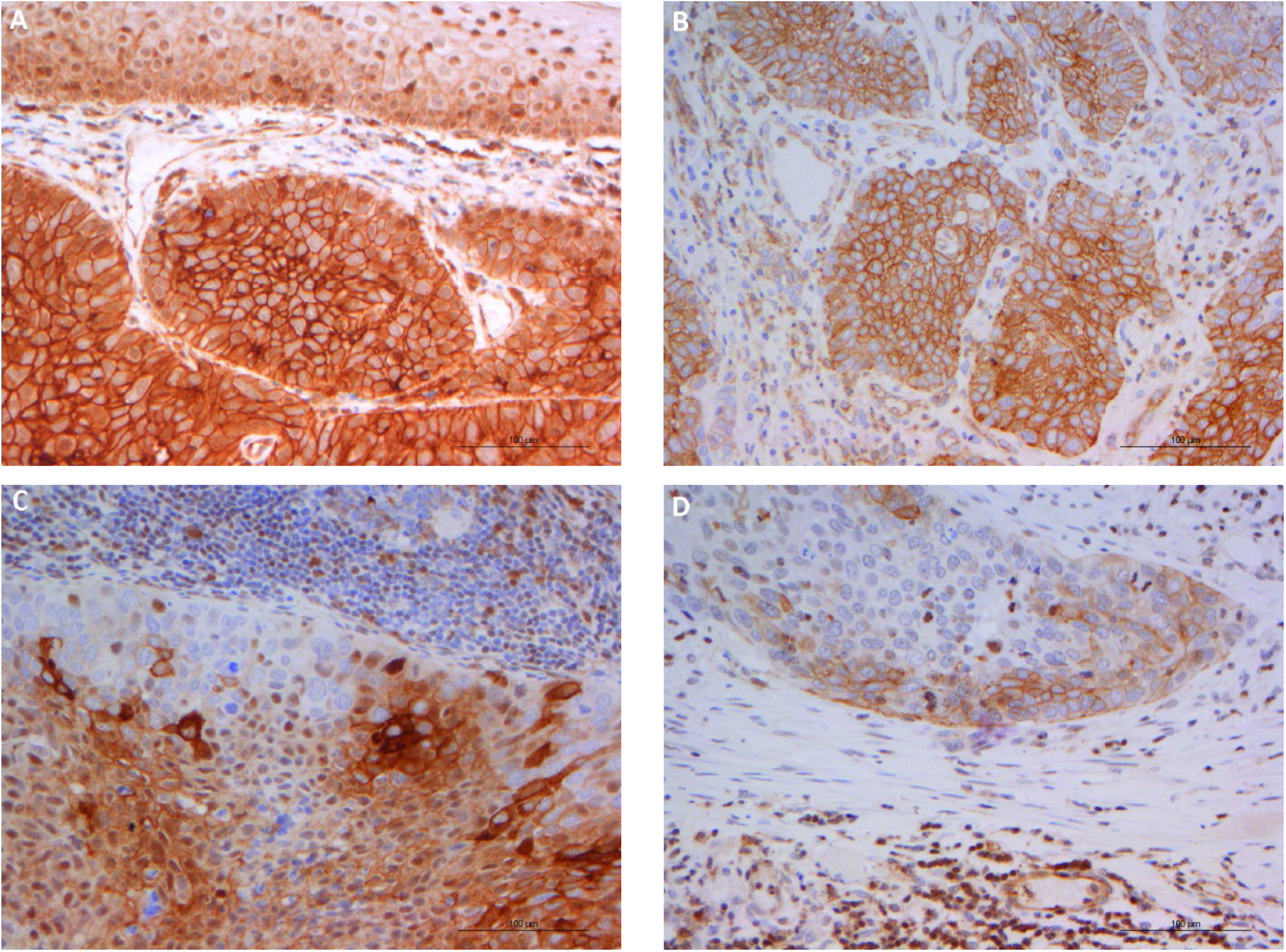
(
Twenty-six of the 38 patients with LSCC were immunohistochemically p-Y466-cortactin-positive, 11 showed no such immunoreactivity, and one was not evaluable due to fixation artifacts. The mean p-Y466-cortactin expression was 8.4% ± 11.9% (median 2.0%). In LSCC, the subcellular pattern of p-Y466-cortactin staining was cytoplasmic granular and membranous in 13 cases, only membranous in 9, and only granular in 4. With the Mann-Whitney U-test, p-Y466-cortactin expression in LSCC was not significantly associated with pT (p = 0.88), grade (p = 0.27), N status (p = 0.16), stage (p = 0.33) or disease recurrence (p = 0.48). Fisher’s exact test ruled out any association between p-Y466-cortactin immunostaining pattern in LSCC and pT (p = 0.87), grade (p = 0.69), N status (p = 0.44), stage (p = 0.73) or disease relapse (p = 1). As for the 10 neck lymph node metastases, 8 specimens were positive for p-Y466-cortactin, and 2 were negative (mean expression 5.2% ± 4.3%; median 5.0%). When p-Y466-cortactin expression in neck lymph node metastases was analyzed, a marginally significant association emerged with grade (Mann-Whitney U-test, p = 0.05), but not with pT (Mann-Whitney U-test, p = 0.82), stage (Mann-Whitney U-test, p = 0.58) or carcinoma recurrence (Mann-Whitney U-test, p = 0.82) (Tab. II).
Only 8 of the 38 patients with LSCC were positive for p-Y421-cortactin, while 29 were negative, and one was not evaluable due to fixation artifacts. The mean p-Y421-cortactin expression was 1.6% ± 4.3% (median 0%). Its staining pattern in laryngeal carcinoma cells was only membranous in 4 cases, cytoplasmic granular and membranous in 3, and only cytoplasmic granular in 1. Using the Mann-Whitney U-test, LSCC p-Y421-cortactin expression was not significantly associated with pT (p = 0.39), grade (p = 0.18), N status (p = 0.07), stage (p = 0.43) or carcinoma recurrence (p = 0.66). Fisher’s exact test found no associations between p-Y421-cortactin-staining pattern in LSCC and pT (p = 1.00), grade (p = 1.00), N status (p = 1.00), stage (p = 1.00) or disease relapse (p = 0.21). Among the 10 neck lymph node metastases, only 2 specimens were p-Y421-cortactin-positive (Tab. II).
Statistical relationship between cortactin and phosphorylated cortactin expression
In supraglottic carcinoma specimens, Spearman’s rank correlation test found a significant direct correlation in the expression levels between cortactin and p-Y466-cortactin (ρ = 0.35, p = 0.031), and between p-Y466-cortactin and p-Y421-cortactin (ρ = 0.60, p = 0.001), but not between cortactin and p-Y421-cortactin (ρ = 0.10, p = 0.52).
In the subcohort of pN+ patients (10 cases), the Mann-Whitney U-test ruled out any significant differences in the mean expression levels of cortactin (p = 0.35), p-Y466-cortactin (p = 0.27) and p-Y421-cortactin (p = 0.52) between the primary supraglottic carcinomas and the corresponding neck lymph node metastases.
Bootstrapping analysis for cortactin expression and p-Y466-cortactin expression in primary LSCC
F test ruled out any significant differences in terms of cortactin expression and p-Y466-cortactin expression in primary LSCC comparing N0 and N+ patients (p = 0.97 and p = 0.33, respectively).
Furthermore, from a prognostic viewpoint, F test did not find any significant difference in LSCC cortactin and p-Y466-cortactin expressions between patients who developed and those who did not develop recurrence of disease after treatment (p = 0.22 and p = 0.77, respectively).
Discussion
The survival rates and prognosis are still not satisfactory for LSCC patients with advanced disease. The high rates of relapse and metastasis associated with LSCC, combined with its resistance to chemotherapy, lead to poor treatment outcomes. There is a need for appropriate molecular markers (14) to consider together with conventional prognostic factors in order to stratify LSCC cases in terms of their metastatic potential and recurrence risk.
Given the marked propensity of supraglottic LSCC to invade and spread through lymphatic vessels, assessing the expression of cell adhesion molecules might have a key role in predicting the behavior of this disease. Since cell–cell and cell–stroma interactions play an important part in carcinogenesis, investigating cell adhesion molecules in surgical LSCC specimens could help us to identify potential targets for therapy too. There is also evidence to suggest that loss of epithelial adhesion would have a role in the development of metastasis (15). Among several molecules involved in cell adhesion, cortactin has aroused interest because of its ubiquitous presence in cell motility structures such as the lamellipodia and invadopodia (4).
Cortactin gene amplification was found to be related to poor prognosis in head and neck squamous cell carcinoma (HNSCC) (16). Cortactin mRNA expression (17) and protein expression (18) have been associated with lymph node metastasis rate and disease-specific mortality. Cortactin expression was investigated in laryngeal epithelial precursor lesions with a view to predicting progression toward malignancy, and the combined assessment of cortactin and focal adhesion kinase (FAK) proved quite reliable in terms of prognostic value and sensitivity (15). Unfortunately, the main available clinical studies on the role of cortactin in head and neck carcinogenesis have some clinical limitations. Most of them have considered head and neck cancer globally, not specific subsites (8, 15-18). They have often investigated cortactin expression as a potential biomarker of the transformation of premalignant lesions, rather than as a prognostic indicator in terms of cancer recurrence rate and survival (19). They have also failed to consider the role of cortactin’s isoforms and their intracellular expression. Focusing on LSCC, Gibcus et al (20) applied immunohistochemical analysis to cyclin D1, Fas-associated protein with death domain (FADD) and cortactin, in a series of 106 cases: cortactin expression proved the best predictor of disease- specific survival in late-stage LSCC.
The role of cortactin phosphorylation, and of the tyrosine kinases involved, has recently attracted attention because phosphorylation of the tyrosine residues 421, 466 proved necessary to initiate in vitro actin polymerization in invadopodia – a step essential to ECM degradation and tumor cell invasion (21). There is in vivo evidence of cortactin phosphorylation on tyrosine residues being associated with bone metastasis in mouse breast cancer cells (22), but little is known as yet about the prognostic role of cortactin and its phosphorylated isoforms in clinical settings.
In the present study we focused on the biological and prognostic significance of the intensity of expression and intracellular localization of cortactin and its phosphorylated isoforms in supraglottic LSCC. The main strength of this study was in the homogeneity of the series of patients considered: (i) they all underwent primary laryngeal surgery; (ii) their surgical treatment was performed consecutively by the same team; (iii) a standardized follow-up protocol was implemented for all patients; (iv) only squamous cell carcinomas located in a single head and neck structure (the larynx) and at a single site (the supraglottis) were considered; and (v) only surgical specimens (not biopsies) of LSCC were assessed. Cortactin and phosphorylated cortactin (residues tyr421 and tyr466) expression was also measured in 10 lymph node carcinoma metastases.
The main weaknesses of our study, on the other hand, concern its retrospective setting and the limited number of cases considered. Furthermore, the completeness of the present study could definitely be increased by the use of quantitative analysis by real-time PCR; we are currently evaluating this further development of investigations into the role of cortactin in laryngeal carcinoma in a larger series.
Our statistical analysis failed to identify a prognostic role (in terms of recurrence rate or DFS) for the expression of cortactin and its isoforms in supraglottic LSCC, also applying, when applicable, bootstrapping analysis. On immunohistochemistry, 34/38 supraglottic LSCCs and 9/10 lymph node metastases were cortactin-positive, with a mean expression of 86.5% ± 24.7% and 94.4% ± 15.7%, respectively. In our cohort of LSCCs, cortactin expression was definitely higher in the cytoplasm of carcinoma cells than in the adjacent normal laryngeal mucosa. Cortactin up-regulation in LSCC supports the conviction that inhibiting cortactin functions could have selective effects on this malignancy. Our statistical analysis identified significant differences in cortactin expression between LSCC cases stratified by pathological grade, but not by pT, N status, stage or recurrence rate. P-Y466-cortactin was seen in nearly 70% of primary LSCCs and lymph node metastases, and the prevalent patterns were cytoplasmic (granular) and membranous in primary tumors, and only membranous in metastases. The association between p-Y466-cortactin expression in neck lymph node metastases and pathological grade was of marginal statistical significance. P-421-cortactin was found in a lower proportion of cases (approximately 20% of primary LSCCs, and 20% of lymph node metastases), and the prevalent pattern was only membranous in both primary tumors and metastases, suggesting a different functional role in the course of pathway as well as a progressive phosphorylation.
It has been claimed that cortactin could activate the epidermal growth factor receptor (EGFR)-ERK signaling pathway (7). Cortactin has also been described as having a role in receptor-mediated endocytosis, and during receptor internalization, its overexpression inhibits the ubiquitylation-mediated degradation of EGFR, resulting in a sustained ligand-induced EGFR activity (23). High levels of EGFR are a common finding in HNSCCs and have been associated with a poor prognosis and resistance to cytotoxic agents, including ionizing radiation (24). The significantly higher expression of cortactin in carcinoma cells than in the adjacent normal laryngeal mucosa, together with its involvement in the EGFR pathway, support a potential role for this protein as a target for LSCC therapy. There are already reports of cortactin overexpression promoting resistance to the EGFR kinase inhibitor gefitinib in HNSCC. These findings indicate that cortactin may have multiple roles in the progression of LSCC and should be considered as a possible marker of response to treatment, and to EGFR-directed agents in particular (25), and also used to improve the radiosensitivity of HNSCC.
Further, well-designed prospective studies in larger series are needed to confirm our results and test the correlation between the expression and subcellular localization of cortactin, p-Y466-cortactin, p-Y421-cortactin and EGFR, in LSCC. Prospective studies could also be designed to investigate the role of cortactin overexpression in resistance to anti-EGFR therapies.
Footnotes
Acknowledgements
The authors thank Frances Coburn for correcting the English version of this paper.
Disclosures
Financial support: This study was partly supported by grant no. 60A07-4802/15 (to G.M.) from the University of Padova, Italy.
Conflict of interest: The authors declare that they have no conflict of interest.