
Abstract
Background:
Several studies have suggested that there are single nucleotide polymorphisms (SNPs) that can be considered potential biomarkers in the prognosis and therapeutic response of cancer patients. The present study investigated the association between ERCC1 rs3212986 and XRCC3 rs861539 polymorphisms and clinical toxicities induced by chemoradiotherapy (CRT) in cervical cancer.
Methods:
This hospital-based retrospective cohort study included 260 patients with cervical cancer, FIGO stages Ib2-IVa, who underwent CRT (cisplatin). Genetic polymorphisms analysis was performed by allelic discrimination with real-time polymerase chain reaction (RT-PCR).
Results:
Our results indicated a link between ERCC1 rs3212986 and the onset of late gastrointestinal toxicity (p = 0.038). Furthermore, using a recessive model (AA vs. CC/CA), we found that patients carrying AA homozygous genotype presented a fourfold increased risk of developing late gastrointestinal toxicity when compared with patients with the C allele (odds ratio = 3.727, 95% confidence interval, 1.199-11.588; p = 0.017). No association was found regarding the XRCC3 rs861539 polymorphism and any clinical toxicity event.
Conclusions:
This is the first study evaluating the relationship between these polymorphisms and clinical toxicities in cervical cancer patients submitted to CRT with cisplatin. These results may contribute toward a better understanding of the influence of genetic polymorphisms in genes associated with DNA repair in the clinical response to CRT of patients with cervical cancer.
Introduction
In 2012, cervical cancer was the fourth most commonly diagnosed cancer in women worldwide, with 528,000 new cases (1, 2). Therapeutic decisions should be based on patient characteristics (age, hemoglobin level), as well as on tumor characteristics (stage, tumor size, histological type and lymph node involvement). Current standard treatment of locally advanced cervical cancer is cisplatin-based concurrent chemoradiotherapy (CRT) (3). Although there is an improvement in survival rates, an increase in the incidence of toxicity in these patients is observed (3-5). In particular, there is concern that increased acute toxicity would lead to delays in radiotherapy (RT), whereas late toxicity remains to be quantified (6). Thus, more studies are needed to improve local control and to minimize the toxicity, and consequently, to improve the survival of patients.
The analysis of interindividual genetic variations can contribute to the early identification of a subgroup of patients that may benefit from therapy adjusted to the genetic information of the tumor, to increase the efficiency of treatment and to reduce toxicity (7). Recently, the role of polymorphisms in DNA repair genes has received special attention. Genetic polymorphisms in pathways of drug activity and metabolism or DNA repair may be associated with differential effects on toxicity (8). It is clear that cells are susceptible to DNA damage and that they contain DNA repair pathways that can be modified. Consequently, DNA damage is an important and even essential mechanism mediating toxicity in cells after cancer therapies, which, in turn, could alter protein expression and function in these cells. Thus, the targeting DNA damage and repair would likely provide a novel and important therapeutic approach for preventing or reversing toxicities associated with various cancer therapies (9).
One of the promising biomarkers for predicting therapeutic response is the excision repair cross-complementation group 1 (ERCC1) gene, a key protein involved in the processes of the nucleotide excision repair (NER) pathway, which is considered the main system to repair a wide variety of DNA damage, particularly bulky adducts, cross-linking and oxidative DNA damage (10-12). ERCC1 rs3212986 polymorphism is the most widely assessed and consists of a change of cytosine (C) to adenine (A) in the 3’-untranslated region at codon 504 (13-15). This polymorphism appears to be associated with changes in mRNA stability and can decrease DNA repair (16). In the literature, there are studies that have evaluated the role of this polymorphism in the risk for developing cancer, overall survival and treatment response (17-20). Although the relationship between this polymorphism and toxicities has not been studied in cervical cancer, results are available in tumoral models in lung cancer (8). Another studied gene is the X-ray repair complementing defective repair in Chinese hamster cells 3 (XRCC3) gene that is involved in the homologous recombination (HR) pathway and helps maintain chromosomal stability through the repair of DNA damage. Many polymorphisms in this gene have been identified, and the most studied polymorphism is XRCC3 rs861539 consisting of the single substitution of a cytosine (C) to thymine (T) at nucleotide 241, which leads to the replacement of threonine (Thr) by methionine (Met) (21, 22). The biological effect of this polymorphism is still controversial; however, it seems that its presence may lead to a reduction in DNA repair capacity (22, 23). Most studies have investigated the relationship between this polymorphism and the risk of developing neoplasia or adverse reactions induced by RT. Until now, there are no studies that associate this polymorphism with CRT toxicities in cervical cancer; however, it has been explored in other cancers, particularly in bladder cancer (24).
To the best of our knowledge, this is the first study that investigated the possible association between ERCC1 rs3212986 and XRCC3 rs861539 polymorphisms and clinical toxicities induced by CRT in cervical cancer patients.
Methods
Study population
This hospital-based retrospective cohort study included 260 patients diagnosed with cervical cancer, FIGO stage Ib2-IVa, who completed concurrent CRT with cisplatin in the Portuguese Institute of Oncology of Porto (Portugal) between February 2002 and October 2009. External RT was delivered with high-energy photon beams, with a total dose of 45 Gy given in 25 fractions within 5 weeks, using standard fractionation. Concurrently with external RT, 6 cycles of chemotherapy were administered to all of the patients as an intravenous infusion of once-weekly cisplatin 40 mg/m2. On completion of external beam RT, low-dose rate brachytherapy was performed. The patients in this study were selected consecutively according to the following inclusion criteria: women with cytological and histological diagnosis of cervical cancer, who were 18 years or older, with Ib2-IVa stage disease treated with concomitant CRT. We excluded patients who underwent surgery before concurrent CRT. All biological samples from patients were used with their prior knowledge and consent, following validation of informed consent, according to the Helsinki Declaration principles. The study was approved by the ethics committee of the Portuguese Institute of Oncology (CES.287/014). Clinicopathological characteristics of patients are summarized in Table I, as obtained from medical records.
Patients’ clinical characteristics (N = 260)
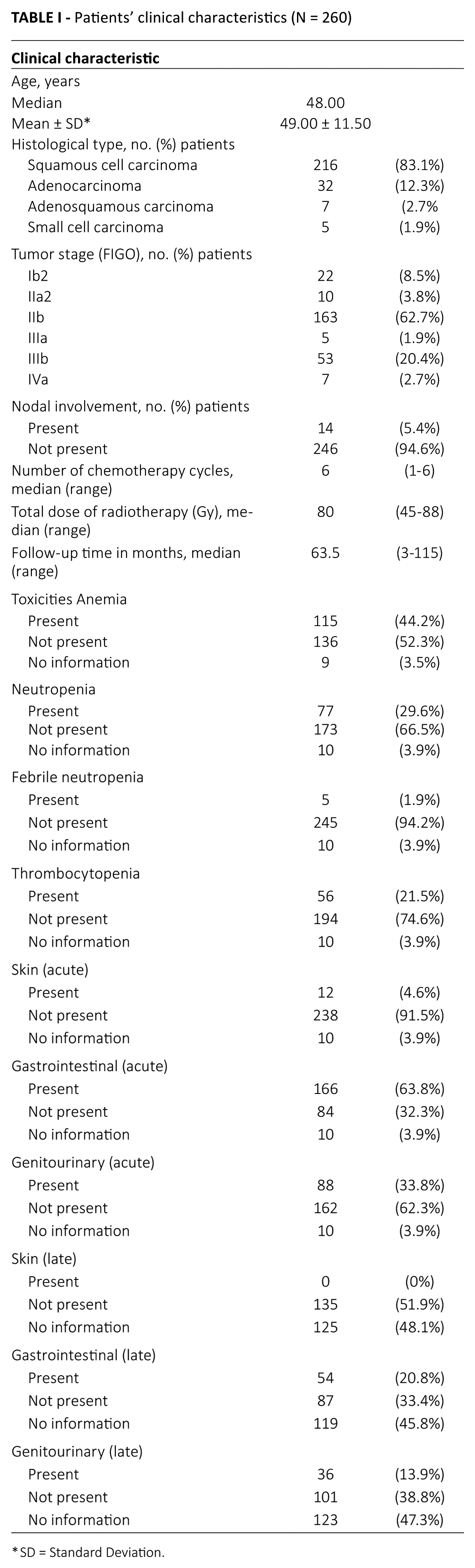
SD = Standard Deviation.
Genotyping
Genomic DNA was extracted from the white blood cell fraction of each study patient using the FavorPrepTM Genomic DNA Mini Kit (FABGK® 300), according to the manufacturer’s protocol.
These polymorphisms were selected according to the following criteria: there was scientific evidence from previous studies; public databases existed that provided information about the phenotypic risk and the biological effect of the polymorphism and the minor allele had a frequency of at least 10% to 20%.
The characterization of ERCC1 rs3212986 and XRCC3 rs861539 polymorphisms was performed by allelic discrimination using TaqMan technology (Applied Biosystems) with real-time polymerase chain reaction (RT-PCR). Amplification was detected and analyzed using ABI 7300 real-time equipment and the ABI 7300 Sequence Detection System software, version 1.2.3 (Applied Biosystems). PCR conditions were performed with a 6-μL final volume mixture containing 1 μL of DNA. Thermal cycling conditions were 10 minutes at 95°C followed by 45 cycles of 15 seconds at 92°C and 1 minute at 60°C. Quality control procedures implemented for genotype analyses included double sampling in about 10% of the samples to assess reliability and the use of negative controls. Two authors (S. S. and A. N.) evaluated the results independently.
Statistical analysis
Statistical analysis was performed using SPSS software, version 22.0. The Hardy-Weinberg equilibrium (HWE) was calculated using the goodness-of-fit Pearson test, comparing the genotype frequencies observed versus those expected. Analysis by Pearson chi-square (X2) test was used to compare the different categorical variables. For groups with fewer than 5 cases, the Fisher exact test was used as an alternative to the chi-square test. The association between ERCC1 rs3212986 and XRCC3 rs861539 and the risk for clinical toxicity was analyzed by logistic regression analysis, and the results are described using odds ratios (ORs) and 95% confidence intervals (95% CIs). A p value ≤0.05 was considered statistically significant.
Results
The analysis of the HWE in the study population according to the genotypes demonstrated that the observed genotype frequencies were statistically different from those expected for the polymorphism in the ERCC1 (p = 0.002) and similar to polymorphism in the XRCC3 (p = 0.891).
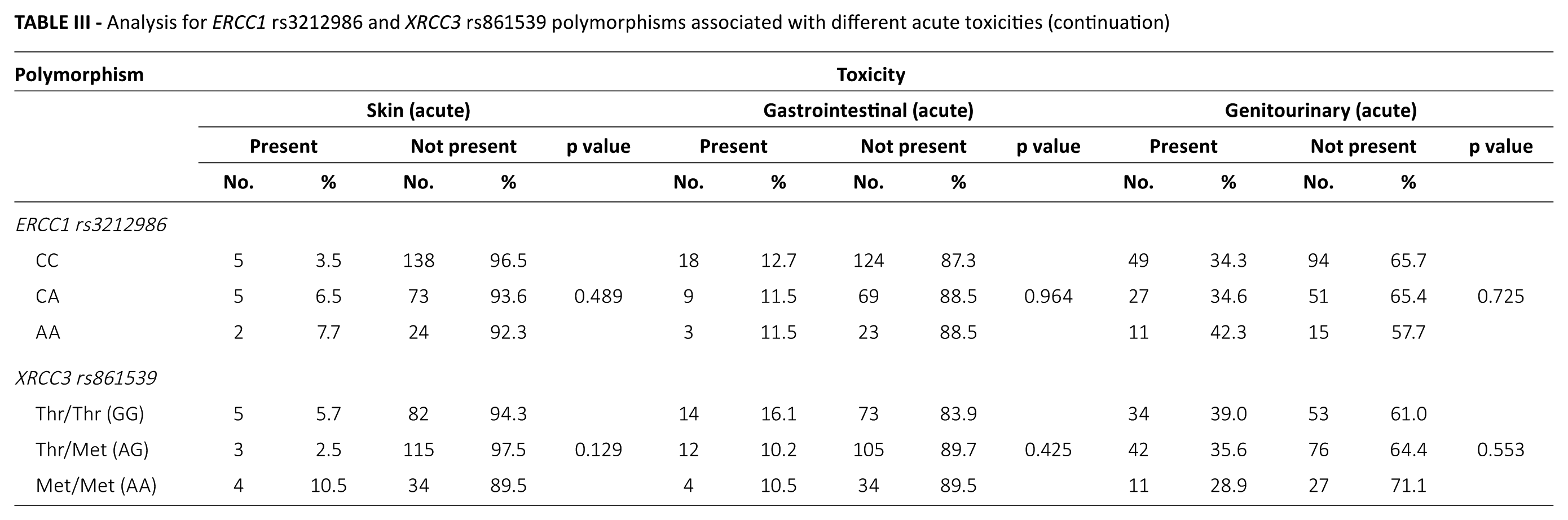
In this study, the following toxicities were assessed: anemia, neutropenia, febrile neutropenia, thrombocytopenia, skin (acute and late), gastrointestinal (acute and late) and genitourinary (acute and late). For the XRCC3 rs861539 polymorphism, no statistically significant differences were found between the different genotypes and various toxicities, including for anemia (p = 0.483), neutropenia (p = 0.573), febrile neutropenia (p = 0.757), thrombocytopenia (p = 0.789), acute skin toxicity (p = 0.129), late skin toxicity (no p value), acute gastrointestinal toxicity (p = 0.425), late gastrointestinal toxicity (p = 0.544), acute genitourinary toxicity (p = 0.553) and late genitourinary toxicity (p = 0.984).
Relative to the ERCC1 rs3212986 polymorphism, no statistically significant differences were found for the evaluated toxicities, including anemia (p = 0.456), neutropenia (p = 0.073), febrile neutropenia (p = 0.579), thrombocytopenia (p = 0.990), acute skin toxicity (p = 0.489), late skin toxicity (no p value), acute gastrointestinal toxicity (p = 0.964), acute genitourinary toxicity (p = 0.725) and late genitourinary toxicity (p = 0.719)). Nevertheless, for late gastrointestinal toxicity, there was a statistically significant association for this polymorphism (p = 0.038).
Of the 141 patients studied, 54 patients (38.3%) presented with late gastrointestinal toxicity and among this group, 27, 17 and 10 patients were carrying the genotype CC, CA and AA, respectively. The associations between the genotypes of the polymorphisms studied and different toxicities induced by CRT are shown in Tables II, III and IV.
Analysis for ERCC1 rs3212986 and XRCC3 rs861539 polymorphisms associated with different acute toxicities
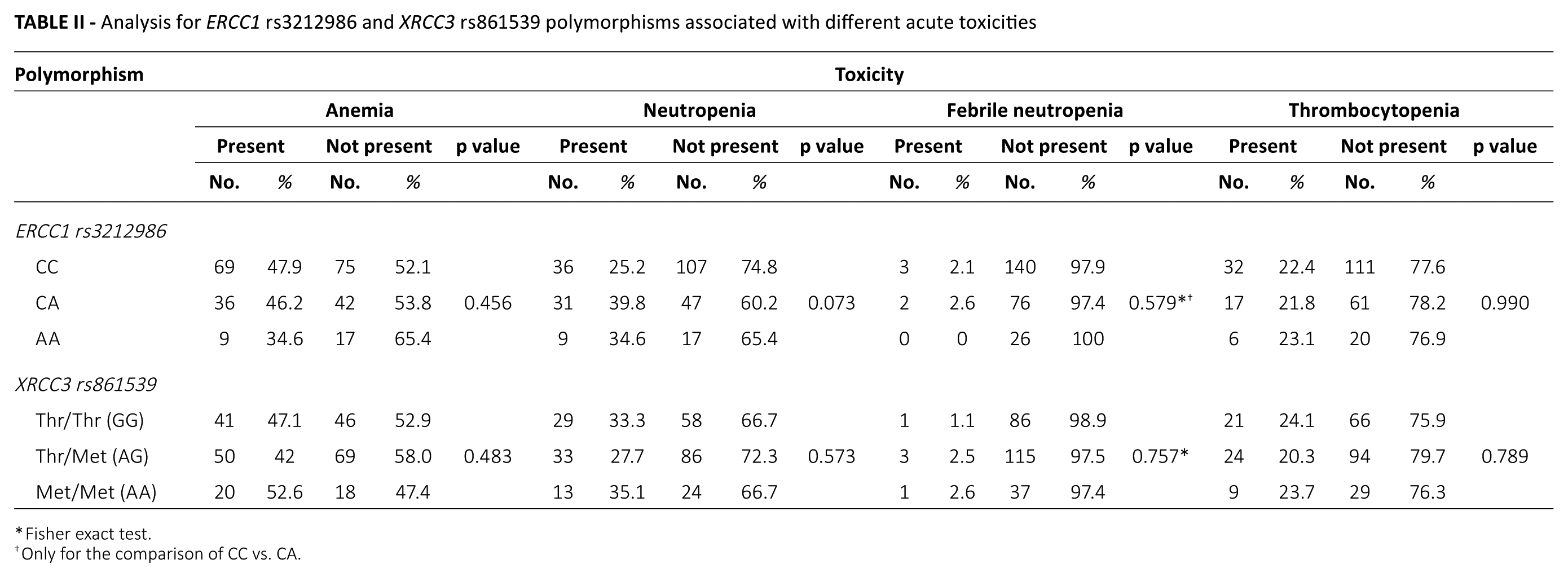
Fisher exact test.
Only for the comparison of CC vs. CA.
Analysis for ERCC1 rs3212986 and XRCC3 rs861539 polymorphisms associated with different acute toxicities (continuation)
Analysis for ERCC1 rs3212986 and XRCC3 rs861539 polymorphisms associated with different late toxicities
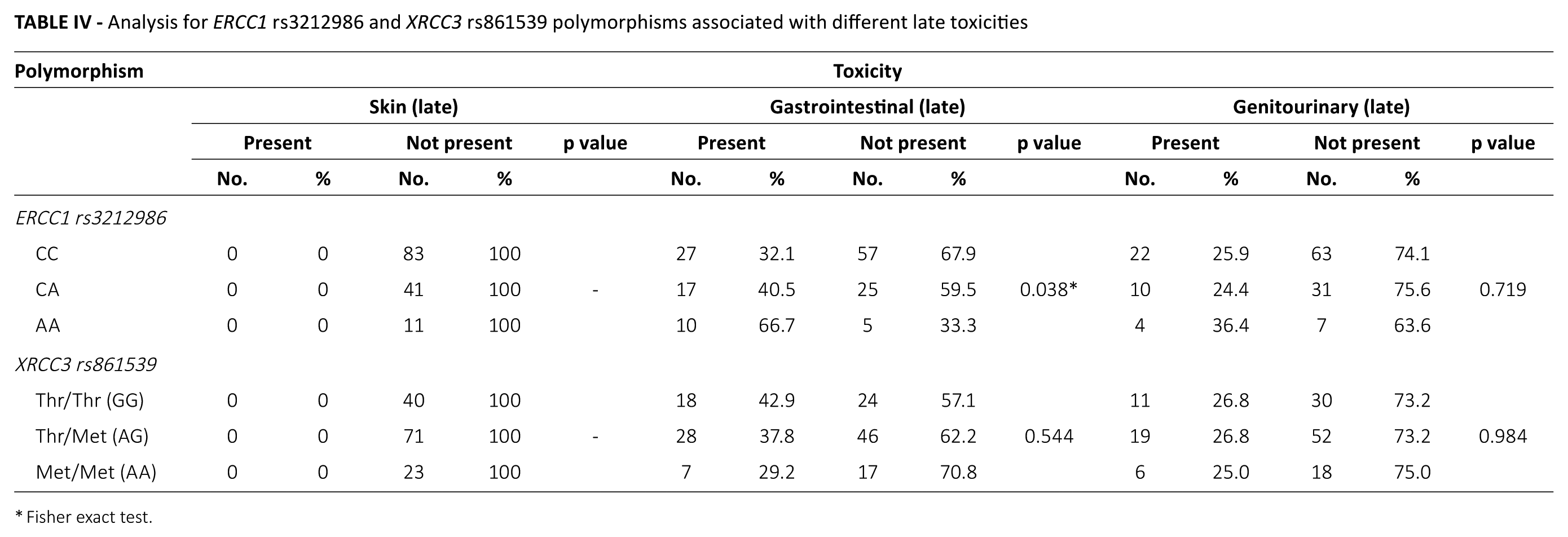
Fisher exact test.
Applying logistic regression, the risk of late gastrointestinal toxicity was significantly associated with homozygous AA genotype, for the recessive model in the ERCC1 rs3212986 polymorphism (AA vs. CC/CA). Thus, patients with homozygous AA genotype have a risk about 4 times higher of developing this type of toxicity compared with patients carrying the C allele (OR = 3.727, 95% CI, 1.199-11.588; p = 0.017). When adjusted for age and therapy response, we observed that the results were similar (OR = 3.693, 95% CI, 1.184-11.520; p = 0.024) (Tab. V).
Analysis of the association between ERCC1 rs3212986 and XRCC3 rs861539 polymorphisms and late gastrointestinal toxicity
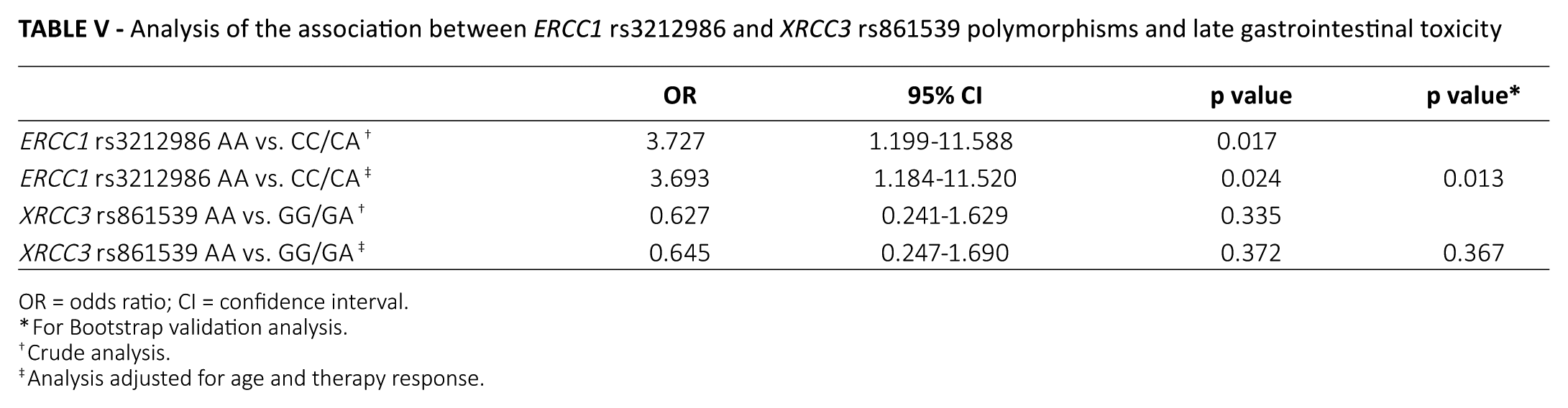
OR = odds ratio; CI = confidence interval.
For Bootstrap validation analysis.
Crude analysis.
Analysis adjusted for age and therapy response.
Discussion
In the literature, approximately 30% of patients experience acute hematological toxicities of grade 3 or greater, and about 1.5% of cases of genitourinary toxicity are acute of grade 3 or greater. Gastrointestinal toxicity is twice as high in grade in CRT-treated patients compared with those treated only with RT (25-27). Commonly, late gastrointestinal toxicities presented by patients include diarrhea and rectal bleeding (28). Apparently, the incidence and severity of these symptoms are associated with a complex interaction between genetic factors and treatment type (26, 29). Thus, it will be relevant to study a possible relationship between polymorphisms associated with DNA repair and the expression of toxicities originated by platinum agents and by ionizing radiation. DNA repair capacity may play paradoxical roles in carcinogenesis, in response to cancer treatment and in clinical toxicity (8). Therefore, these ERCC1 rs3212986 and XRCC3 rs861539 polymorphisms seem to have a lower DNA repair capacity, which has been associated with an increased sensitivity of the cells to drugs and radiation (10, 30).
There have been some reports on the associations between DNA repair gene polymorphisms and toxicity in CRT for lung, breast or bladder cancers (8, 24, 31-33). In cervical cancer, genetic polymorphisms have been studied in relation to the risk of cancer, overall survival and disease-free survival, but not in relation to clinical toxicity (22, 34). In this sense, this is the first study to evaluate the possible association between ERCC1 rs3212986 and XRCC3 rs861539 polymorphisms and the risk of developing toxicities in cervical cancer after CRT.
When analyzing HWE, we found that the observed genotype frequencies were not similar to those expected, for the ERCC1 rs3212986 polymorphism (p = 0.002). Despite the disequilibrium, the allele frequencies of the ERCC1 rs3212986 polymorphism were 74% and 26% for A and C alleles, respectively, and were identical to European allelic frequencies. Similarly, for the XRCC3 rs861539 polymorphism, allele frequencies were similar to those of Europe, with a frequency of approximately 59% of the G allele and 41% of the A allele. Among the genetic polymorphisms studied, the deviation from HWE was observed in analysis only of the ERCC1 gene. HWE deviations could arise through important biological mechanisms. Furthermore, this disequilibrium may be due to several features of the tested population, including mutation, random genetic drift, migration and natural selection (35-37). Moreover, in our study, genotype frequencies for ERCC1 polymorphism were similar to those reported in other studies for European populations (38, 39).
In the present study, the following toxicities were assessed: anemia, neutropenia, febrile neutropenia, thrombocytopenia, skin (acute and late), gastrointestinal (acute and late) and genitourinary (acute and late). For the XRCC3 rs861539 polymorphism, no statistically significant differences were found between the different genotypes and various toxicities analyzed. Gurská and colleagues evaluated the relationship between the radiosensitivity of tumor cells and this polymorphism, and depending on the cervical cancer cell lines used, they had opposite results (40). Furthermore, De Ruyck and colleagues analyzed the relation between the risk of developing adverse reactions to RT in patients who have been treated for gynecological tumors. For the XRCC3 rs861539 polymorphism, no statistically significant association was found between this polymorphism and higher risk for reactions in normal tissues (30).
For the ERCC1 rs3212986 polymorphism, we found statistically significant differences only in the association between the genotypes of this polymorphism and late gastrointestinal toxicity. When applying the recessive model (AA vs. CC/CA), it was found that patients with AA homozygous genotype revealed a greater risk of developing late gastrointestinal toxicity compared with patients with the C allele. There have been no studies investigating the role of this polymorphism and toxicity outcome in cervical cancer. However, Suk et al examined the influence of this polymorphism in lung cancer and found that the incidence of gastrointestinal toxicity of grade 3 and 4 was significantly higher in patients with at least 1 variant allele (AA or CA) that may be associated with an increased risk of developing this toxicity. The authors explained that this may be due to decreased mRNA stability and NER activity in susceptible tissues, leading to more severe toxicity. Also, the deficient NER activity would render tissue more susceptible to platinum-induced damage (8).
Similarly, one possible explanation for our results consists of a destabilization of mRNA caused by the ERCC1 rs3212986 polymorphism and a decrease of the respective protein expression levels, which can induce a decrease of damage repair and hence an increase in toxicity. It is known that this polymorphism affects the NER pathway, which can be crucial to repairing the damage of normal tissues during cytotoxic therapy and therefore to preventing treatment-related toxicity. Thus, this increased toxicity associated with the AA genotype may be correlated with the decrease of mRNA stability and the reduction of the NER pathway activity. Consequently, it will induce an increased toxicity and tissue susceptibility to damage caused by platinum.
So far, the exact mechanism by which this polymorphism affects mRNA stability is not known (8). Moreover, RT by itself can cause increased gastrointestinal toxicity and when added to chemotherapy the effect is stronger (41). Until now, there have been few studies that have investigated the influence of ERCC1 gene polymorphisms in DNA repair capacity and consequently in toxicity outcomes, such as gastrointestinal toxicity, in cancer patients. However, the results are very controversial. and it is necessary that more studies be undertaken (8, 41-44).
These results are still preliminary, so further studies are required in cervical cancer to clarify the mechanisms by which these polymorphisms influence the therapeutic response and toxicity. Major limitations of this study included its retrospective nature and the possibility for ascertainment bias, particularly with regard to toxicity outcomes. In the future, it would be helpful to perform functional tests quantifying ERCC1 and XRCC3 mRNA or evaluating protein expression, in order to establish the functional effect of these polymorphisms. Furthermore, it would be interesting to develop prospective studies to confirm the results obtained in this study.
Conclusion
In conclusion, our study suggests that the ERCC1 rs3212986 polymorphism may be associated with late gastrointestinal toxicity in cervical cancer patients submitted to platinum-based concomitant CRT, possibly owing to the altered DNA repair capacity caused by this polymorphism. In this way, it would be ideal to define risk profiles for the development of toxicities, which might be a useful tool for implementing strategies for the choice of treatment for each patient so as to decrease toxicities, increase treatment response rates and consequently improve overall survival and disease-free survival rates in cervical cancer patients.
Footnotes
Disclosures
Financial support: This work was supported in part by the Research Center of the Portuguese Institute of Oncology of Porto, Portugal (project no. CI-IPOP-22-2015). The authors also thank the Liga Portuguesa Contra o Cancro – Centro Regional do Norte (Portuguese League Against Cancer) for the financial support.
Conflicts of interest: The authors declare they have no conflicts of interest.