
Abstract
Background
Although the diagnosis and treatment of eighth cranial nerve (VIII CN) schwannoma (acoustic neuroma) has improved over the years, no factors capable of predicting tumor growth have been identified as yet. This study is a preliminary investigation of the expression in sporadic VIII CN schwannomas of Yes-associated protein (YAP), transcriptional coactivator with PDZ-binding motif (TAZ), and amphiregulin (AREG), a direct target gene of YAP and TAZ. The expression of YAP, TAZ and AREG was correlated with the volumetric dimensions of tumors on contrast-enhanced magnetic resonance imaging (ceMRI).
Methods
YAP, TAZ and AREG expression was assessed immunohistochemically in surgical specimens of 36 consecutive sporadic VIII CN schwannomas. 3D reconstructions of the tumors and their corresponding volumes in cm3 were obtained from measurements on ceMRI images using the OsiriX® software.
Results
We found a significant direct correlation between TAZ expression and VIII CN schwannoma volumes on latest preoperative ceMRI (p<0.0003). Mean TAZ expression was also significantly higher in VIII CN schwannomas with a volume ≥2.1 cm3 than in those with a volume <2.1 cm3 (p<0.0018). No significant correlations emerged for YAP or AREG expression and VIII CN schwannoma volume.
Conclusions
The immunohistochemical expression of TAZ (but not YAP or AREG) correlated significantly with schwannoma volume measured on ceMRI. Further investigations are needed to identify the biological factors influencing tumor proliferation (ideally secreted proteins like AREG) that might be detected using non-invasive approaches (i.e., blood samples).
Introduction
The outcome of treatment for eighth cranial nerve (VIII CN) schwannoma has continued to improve gradually over the years, mainly because imaging enables early diagnosis and proactive therapy when hearing-preservation surgery is feasible. Ideally, the goal has been to preserve nerve function with “zero” morbidity. The treatment for medium–large-size tumors (1) is well established, while the management of small acoustic schwannomas remains controversial, the options being a wait-and-scan policy or proactive surgery in an attempt to preserve hearing. The former approach is preferred nowadays for tumors that are not growing, or when hearing preservation is not the goal. While it cannot ensure long-term hearing preservation, the rationale behind this conservative attitude lies in recent evidence of a considerable proportion of small tumors (up to 1 cm in the cerebellopontine angle [CPA]) not growing significantly (2-5). Serial imaging enables growth to be monitored, but there are currently no known factors capable of predicting the trend of a tumor's growth, and whether or not proactive treatment would be appropriate.
Molecular changes occur in neoplasms before any morphological changes become visible. Among the current issues influencing decisions concerning the treatment of VIII CN schwannomas, the use of tumor biomarkers is an intriguing and unexplored possibility. YAP (Yes-associated protein) and its paralog TAZ (transcriptional coactivator with PDZ-binding motif) are the primary downstream effectors of the Hippo signaling pathway (6). They are transcriptional cofactors with pivotal roles in several organs, especially in determining their size, and in regulating cell proliferation and apoptosis. Alongside these physiological functions there is growing evidence of YAP and TAZ activity being associated with tumorigenesis, tumor growth, epithelial-mesenchymal transition, sternness, metastasis, and chemoresistance (6-10). YAP and TAZ move from the cytoplasm to the nucleus, where they become linked to various promoter-specific transcription factors and thus become transcriptionally active. Among the several partners of YAP and TAZ, members of the TEA domain (TEAD) transcription factor family are the most common in regulating gene expression: TEAD transcription factors also regulate cell proliferation and apoptosis (11-15). Amphiregulin (AREG) is a member of the epidermal growth factor family that was initially characterized as a schwannoma-derived growth factor expressed in response to androgen in the SC2G murine cell line. AREG is produced and secreted by normal keratinocytes and acts as an autocrine growth factor. AREG binds ErbB-1, which is essential for epithelial development in the skin, lung and gastrointestinal tract. It was recently demonstrated that AREG is a direct target gene of YAP and TAZ (16, 17).
Predicting the growth of vestibular schwannomas (in particular small ones) may orient therapeutic decisions, affording the best prognosis in terms of reducing perioperative morbidity and achieving high functional (facial nerve and hearing) preservation rates. This is the first study to have investigated YAP, TAZ and AREG expression in a consecutive surgical case series of sporadic VIII CN schwannomas. The expression of YAP, TAZ and AREG was correlated with the volumetric dimensions of VIII CN schwannomas measured on high-resolution contrast-enhanced magnetic resonance images (ceMRI).
Methods
Patients
The study was conducted on surgical specimens from 36 patients (17 men and 19 women with a mean age of 51.8 ± 12.4 years, median 50 years) with primary sporadic VIII CN schwannoma treated by the same team of surgeons at our institution between 2012 and 2014. Twenty-nine patients underwent surgery within 6 months of their tumor being diagnosed, and 7 after a mean observation period of 23.5 months (range 6-58 months) to assess tumor growth. In 4 cases, hearing-preservation surgery via a retrosigmoid approach (4, 5) was preferred, while the translabyrinthine approach was adopted for the other 32 patients. Our institutional indications for the management of sporadic acoustic neuroma are summarized in Table I.
Institutional recommendations on sporadic acoustic schwannoma management
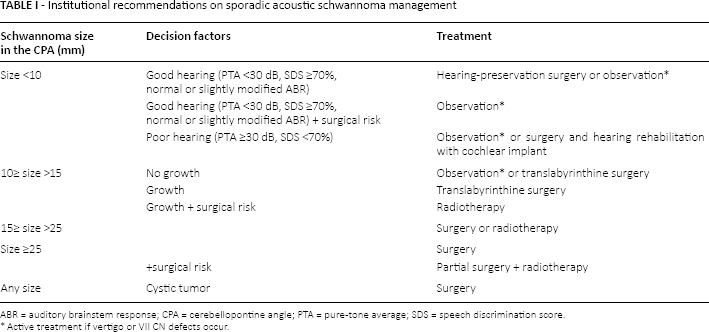
ABR = auditory brainstem response; CPA = cerebellopontine angle; PTA = pure-tone average; SDS = speech discrimination score.
Active treatment if vertigo or VII CN defects occur.
Most patients had hearing loss on presentation, which was isolated in 17 cases and associated with other otological symptoms (tinnitus, fullness) in 7; 3 patients presented with isolated tinnitus; one with vertigo; and 7 with vertigo associated with other symptoms (hearing loss, fullness or tinnitus). One patient had no symptoms, and the schwannoma was an incidental finding on a ceMRI scan done for other reasons.
All patients were diagnosed by high-resolution ceMRI of the brain and CPA. The cases managed by means of hearing-preservation surgery via a retrosigmoid approach and retrolabyrinthine meatotomy also underwent preoperative high-resolution bone CT scan. Complete resection was accomplished in all cases.
The sporadic VIII CN schwannomas were classified as: purely intrameatal (4 cases); small, up to 1 cm in the CPA (8 cases); medium-sized, 1-2.5 cm in the CPA (19 cases); and large, more than 2.5 cm in the CPA (5 cases).
Final pathological examination confirmed the preoperative diagnosis of schwannoma in all cases.
Immunohistochemistry
Original sections stained with hematoxylin and eosin, and corresponding formalin-fixed and paraffin-embedded (FFPE) samples of the tumors resected from each patient were retrieved from the archives of the Surgical Pathology and Cytopathology Unit at the University of Padua and reviewed by 2 pathologists (A.F. and R.C.). The most representative FFPE block was selected for immunohistochemical analysis.
Immunohistochemical staining was done automatically using the Bond Polymer Refine Detection kit (Leica Biosystems) in the BOND-MAX system (Leica Biosystems) on 4-μm-thick consecutive sections from each tumor, as described elsewhere (18, 19), with the primary antibodies against YAP (mouse monoclonal, clone 2F12; Sigma-Aldrich; working dilution 1:800, 30 minutes, citrate buffer); TAZ (rabbit polyclonal; Sigma-Aldrich; working dilution 1:750, 30 minutes, citrate buffer); and AREG (mouse monoclonal, clone G-4; Santa Cruz Biotechnology; working dilution 1:100, 30 minutes, EDTA buffer). Sections were then slightly counterstained with hematoxylin. Appropriate positive and negative controls were run concurrently.
Only nuclear immunoreactions were considered for YAP and TAZ, and cytoplasmic immunostaining for AREG. The percentage of positive neoplastic cells was assessed jointly by 2 pathologists (A.F. and R.C.).
Volumetric radiological measurements
The anatomical size of the lesion was calculated from measurements obtained on ceMRI using the open-source OsiriX® software. DICOM data were stored in the OsiriX PACS (2.8-GHz Intel Core 2 Duo 24″ iMac, Apple Inc.). The software can calculate the volume of a solid lesion starting from a series of 2D regions of interest (ROIs). The tumor's boundaries were outlined manually with the “pencil” tool, selecting one ROI for each slice on the axial planes and taking care to avoid the inclusion of perilesional edema. Then the 3D tumor volume was reconstructed using the multiplanar reformation (MPR) computer volume application, and the corresponding volume in cm3 was obtained. The dimensions of each patient's tumor were estimated on their MR images, preferably analyzing the same type of sequence, choosing the T2w or T1w post-gadolinium image that facilitated the tumor's measurement. The radiological assessment was retrospective and the images were obtained at different hospitals, so not all the analyses were performed using the same sequences.
Statistical analysis
The following statistical tests were applied, where applicable: one-way analysis of variance after Bartlett's test for equal variances and the Mann-Whitney 2-sample rank-sum test. The correlation between 2 measures was determined using Pearson's correlation coefficient. In the event of multiple testing, the Bonferroni-adjusted significance level was applied.
A volume of 2.1 cm3 was chosen as the cutoff for binarizing the continuous variable schwannoma size at the last ceMRI before surgery. This cutoff coincided with the 75th percentile of the pooled schwannoma volumes calculated.
A p value <0.05 was considered significant. The STATA™ statistical package 8.1 (StataCorp) was used for all analyses.
Results
Immunohistochemical evidence
YAP and TAZ expression levels showed marked variability among the schwannomas considered, ranging from absent in some cases to as high as 90% of immunoreactive cells in others. The mean percentages of positive cells were 35.6% ± 30.0% for YAP and 33.9% ± 27.8% for TAZ (Fig. 1A and 1B).

Representative photomicrographs of immunohistochemical reactions in the present series of schwannomas. YAP (
For AREG, the percentage of immunoreactive cells ranged from 0% to 70% (Fig. 1C). Seven tumors were AREG positive with less than 10% of positive cells, while immunostaining was negative in 14 cases. The mean percentage of immunoreactive cells was 11.2% ± 17.3%.
YAP expression and radiological evidence
The OsiriX-based calculation generated a mean volume of 1.7 ± 2.0 cm3 in our series of sporadic VIII CN schwannomas. The statistical analysis ruled out any significant correlation between YAP expression and VIII CN schwannoma volume on the last preoperative MRI (Pearson's correlation coefficient −0.25, p<0.92).
TAZ expression and radiological evidence
The statistical analysis revealed a significant direct correlation between TAZ expression and VIII CN schwannoma volume on the last preoperative MRI (Pearson's correlation coefficient 0.56, p<0.0003). One-way ANOVA showed significantly higher mean TAZ expression in VIII CN schwannomas ≥2.1 cm3 in volume than in those with a volume <2.1 cm3 (p<0.0018) (Tab. II).
Expression of YAP, TAZ and AREG in VIII CN schwannomas, and their calculated volumes

AREG expression and radiological evidence
The statistical analysis ruled out any significant correlation between AREG expression and VIII CN schwannoma volume on last preoperative MRI (Pearson's correlation coefficient −0.17, p<0.31).
Relationships between YAP, TAZ and AREG expression levels
In our cohort of 36 VIII CN schwannomas, the statistical analysis found no significant correlation between the expression levels of YAP and TAZ (Pearson's correlation coefficient −0.22, p<0.19), YAP and AREG (Pearson's correlation coefficient −0.026, p<0.88), or TAZ and AREG (Pearson's correlation coefficient −0.24, p<0.45).
Subcohort of patients whose tumor growth rate (cm3/month) was calculated on MRI
For the 8 patients who underwent ceMRI twice or more preoperatively, the VIII CN schwannoma growth rate was calculated as:

and was 0.3 ± 0.04 cm3/month. The statistical analysis ruled out any significant correlation between tumor growth rate and the expression levels of YAP (Pearson's correlation coefficient −0.17, p<0.67), TAZ (Pearson's correlation coefficient −0.23, p<0.57), or AREG (Pearson's correlation coefficient −0.01, p<0.97).
Discussion
In acoustic schwannoma, early diagnosis is currently the key to ensuring lasting cure with the lowest possible morbidity. The aim of treatment is to preserve the VII and VIII CNs, and other more general functional aspects, at their pretreatment levels. A conservative wait-and-scan policy would gain considerably if it were possible to identify some factors capable of predicting tumor growth. For the time being, observation and radiology are the only options for assessing tumor growth and deciding when surgery is warranted. A rational clinical approach relies on monitoring of schwannoma growth and deciding appropriate treatment, also as regards its timing. It would be extremely useful to establish which biological factors influencing the neoplasm's proliferation in the tissues might be detected or measured by minimally invasive means (such as a blood sample).
Tumor size depends on cell number and is regulated by pathways that communicate extra- and intracellular signals for gene transcription. For our investigation into VIII CN schwannoma growth, YAP and TAZ seemed promising because they form the main output of the Hippo signaling pathway, which has been shown to play a crucial part in determining organ size (6, 14, 15). Using a set of more than 40 human schwannomas (NF2 disease or sporadic tumors), Boin et al (20) analyzed the status of several major signaling pathways previously found to be regulated by moesin-ezrin-radixin-like protein (merlin). Merlin also participates in Hippo signaling in mammalian cells (21), and has been shown to regulate the expression and localization of YAP in schwannoma cells (22). Boin et al (20) concluded that proliferation of the tumor cells investigated would correlate with the activation of a signaling network linked to the Hippo effector YAP and several of its target genes. TAZ is a paralog of YAP, sharing about 50% of its sequence with the latter. TAZ has a similar topology and, like YAP, acts as a transcriptional coactivator (23). Yang et al (17) reported that TAZ overexpression in human mammary epithelial cells promotes epithelial-to-mesenchymal transition and, in particular, some invasive structures in 3D cultures. Wang et al (24) found that TAZ overexpression induces epithelial-to-mesenchymal transition in neuroblastoma too, increasing the tumor cells' invasive capacity. AREG is a member of the epidermal growth factor family, a direct target gene of YAP and TAZ. It is a secreted protein that was found to promote cell proliferation and inhibit cell apoptosis in a variety of tumors, and it could have an important role in the extracellular matrix or blood circulation. AREG can be secreted into the patient's blood system, and its level can be detected non-invasively and quite simply (17). Han et al (25) recently used immunohistochemistry to test YAP, TAZ and AREG expression in hepatocellular carcinoma, and the level of secreted serum AREG was assayed by enzyme-linked immunosorbent assay (ELISA). Multivariate analysis showed that YAP expression was an independent prognostic factor significantly correlated with the overall survival of hepatocellular carcinoma patients. The specificity of serum AREG in the diagnosis of hepatocellular carcinoma was higher than that of alpha fetoprotein. The authors suggested that serum AREG might be used as a serological biomarker of hepatocellular carcinoma.
The main strengths of the present study are that (i) only sporadic VIII CN schwannomas were considered; (ii) the series of tumors was consecutive; (iii) the indication for surgical treatment was decided by the same surgical team; (iv) the surgical treatment was performed by the same team; (v) the histological diagnosis was confirmed by the same pathologists; and (vi) the immunohistochemical results were assessed jointly by 2 pathologists. In addition, the anatomical size of the lesions was established from measurements on MRI images, using software that enables 3D reconstruction of the tumor volume. Such computer-assisted volume calculation can presumably identify the boundaries of the lesion more precisely, even in the case of asymmetrical shapes impossible to approximate to a regular solid. It also helped to compensate for the risk of accuracy being limited when a tumor was not aligned with the conventional planes of MR images, or when an ellipsoid was not a plausible representation of the lesion. The main weaknesses of the present study concern its retrospective setting, the limited number of cases available (especially for the purpose of calculating tumor growth rate), and the lack of a second validation cohort to confirm the results.
From a clinical viewpoint, complete resection was achieved in all cases of the present series and no recurrences were observed. The study identified a significant direct correlation between TAZ expression and VIII CN schwannoma volume, and ruled out any significant correlations between YAP or AREG expression and VIII CN schwannoma volume. No significant correlations emerged between the immunohistochemical expression levels of YAP, TAZ and AREG in the tumor tissue. Although the Hippo pathway controls the expression and activity of both YAP and TAZ (26, 27), it is worth noting that TAZ expression correlated directly with sporadic VIII CN schwannoma cell proliferation, while YAP expression did not – a finding consistent with recent evidence suggesting that these molecules have a functional redundancy, or a partly different function and regulatory capacity (10). Indeed, recent findings indicated that several factors (such as kinases, adaptor proteins, microRNAs, post-transcriptional modifications, and even still poorly understood mechanical stimuli) selectively control TAZ and/or YAP expression, cellular localization, and activity (28). These factors seem to be context dependent and few data concerning schwannoma have become available to date (22, 29). The absence of any correlation between TAZ and AREG expression might also depend on specific schwannoma settings. TAZ probably promotes the transcription of other target genes in this type of tumor.
Conclusions
In this preliminary study, the immunohistochemical expression of TAZ (but not YAP or AREG) correlated significantly with schwannoma volume measured on MRI. To enable the rational planning of either early surgery or a wait-and-scan policy on the grounds of proper monitoring of sporadic VIII CN schwannoma growth, further investigations are needed on larger prospective series, using randomization and blinding methods (30), to identify easily and non-invasively measurable biological factors influencing tumor proliferation. The signaling network controlled by the Hippo effector TAZ deserves further study. Generally speaking, proteomic strategies are a powerful approach for seeking clues and may be able to shed light on the mechanisms promoting tumor growth in sporadic VIII CN schwannoma.
Footnotes
Acknowledgments
The authors thank Frances Coburn for correcting the English version of this paper.
Financial support: This study was partly supported by grant No. 60A07-0199/14 to G. Marioni from the University of Padua, Italy.
Conflict of interest: None.