
Abstract
Purpose
To report long-term experience with intravitreal anti–vascular endothelial growth factor treatment for radiation maculopathy.
Methods
From 2005-2015, 120 consecutive patients underwent intravitreal anti-VEGF therapy for radiation maculopathy. Inclusion criteria included a diagnosis of uveal melanoma treated with plaque radiotherapy and subsequent macular radiation vasculopathy (exudate, retinal hemorrhage, intraretinal microangiopathy, neovascularization, edema). Anti-VEGF therapy involved continuous injections in 4- to 12-week intervals with doses of 1.25 mg/0.05 mL, 2.0 mg/0.08 mL, 2.5 mg/0.1 mL, or 3.0 mg/0.12 mL of bevacizumab as well as 0.5 mg/0.05 mL or 2.0 mg/0.05 mL of ranibizumab. Goals were maintenance of visual acuity and normative macular anatomy. Safety and tolerability (retinal detachment, hemorrhage, infection), visual acuity, central foveal thickness on optical coherence tomography imaging, and clinical features of radiation maculopathy were analyzed.
Results
Progressive reductions in macular edema, hemorrhages, exudates, cotton-wool spots, and microangiopathy were noted. At last follow-up, 80% remained within 2 lines of their initial visual acuity or better, with a mean treatment interval of 38 months (range 6-108 months). Kaplan-Meier analysis of the probability of remaining within 2 lines of initial visual acuity was 69% at 5 years and 38% at 8 years of anti-VEGF therapy. Discontinuation of therapy was rare. Relatively few acute or long-term side effects were noted, allowing for good long-term patient accrual.
Conclusions
Continuous intravitreal anti-VEGF therapy in patients with radiation maculopathy was well-tolerated and preserved vision. In most cases, reductions or resolution of retinal hemorrhages, cotton-wool spots, and retinal edema were noted for up to 10 years.
Introduction
Radiation maculopathy (RM) is a common sight-limiting complication of ophthalmic radiation therapy (1, 2). It occurs after irradiation for tumors or inflammation of the choroid, retina, orbit, and paranasal sinuses (3–4–5–6–7–8). The risk of RM is related to total dose, radiation dose rate, the presence of synchronous systemic diseases (e.g., diabetes), and the use of radiation sensitizers (e.g., chemotherapy) (9–10–11–12–13–14–15–16–17). Past experience suggests that radiation retinopathy is a progressive disease typically characterized by vascular incompetence (with secondary retinal edema), vascular closure (with secondary retinal ischemia), and resultant loss of vision. Left untreated, this process typically evolves over 1-2 years, leaving most patients with poor vision or legally blind (2, 18).
Laser photocoagulation has been used to treat intraocular radiation vasculopathy. Typically, panretinal photocoagulation was employed to salvage eyes with radiation-related neovascular glaucoma, focal laser for radiation-induced retinal neovascularization, and circumferential laser to prevent or delay RM (19–20–21–22).
Selective antibody blocking of vascular endothelial growth factor (VEGF) has been termed anti-VEGF therapy. Anti-VEGF drugs have been injected intravenously, intravitreally, and subconjunctivally to decrease vascular permeability and inhibit the formation of blood vessels (23–24–25–26–27–28–29–30–31–32). Known risks include endophthalmitis, glaucoma, vitritis, and thromboembolic events (e.g., stroke, myocardial infarction). In general, intravitreal injection offers a relative reduction of systemic side effects in exchange for ocular risks (33–34–35–36). In the published literature, there exist no reports of efficacy and toxicity related to long-term administration of intravitreal anti-VEGF agents for RM.
In 2005, we started investigation of intravitreal anti-VEGF therapy (bevacizumab) for plaque brachytherapy-associated RM and radiation optic neuropathy (RON) (23, 25, 29, 37–38–39). Then, in 2011, we reported on intravitreal anti-VEGF therapy for external beam radiation–associated RM (26). Encouraged by those results, in 2013 we reported that recalcitrant RM responded to high-dose intravitreal ranibizumab (40). This study presents our 10-year clinical experience with intravitreal anti-VEGF therapy (bevacizumab and ranibizumab) for treatment of RM associated with ophthalmic plaque radiation therapy.
Methods
Inclusion criteria
A total of 120 consecutive charts of patients treated with intravitreal anti-VEGF therapy for RM between 2005 and 2015 were reviewed. Initial entry criteria included a diagnosis of uveal melanoma treated with plaque brachytherapy, development of radiation-induced maculopathy (defined as macular hemorrhages, cotton-wool spots, microaneurysms, or macular edema), and subjective decrease in visual acuity (VA) or symptoms of metamorphopsia. Patients underwent plaque brachytherapy over 5-7 days with palladium-103 (n = 118, 98%) or iodine-125 (n = 2, 2%) isotopes. Although 58 patients received prior laser demarcation or focal retinal laser to treat, prevent or delay RM, all demonstrated progressive RM despite this treatment prior to inclusion in this study. While our analysis for side effects from intravitreal injection included all patients, our analysis of the efficacy of periodic intravitreal anti-VEGF treatment was based on patients who had received 3 or more injections, with an initial VA of 20/200 or better and at least 6 months of follow-up.
Main outcome measures
Main outcome measures were changes in clinical features of retinopathy (on comparative indirect ophthalmoscopic examination, fundus photography, and/or fluorescein angiography), VA (using Early Treatment Diabetic Retinopathy Study [ETDRS] charts), and central foveal thickness (CFT) on optical coherence tomography (OCT) using Optos (Marlborough, MA, USA; formerly OTI, Miami, FL, USA) and Spectralis (Heidelberg Engineering; San Francisco, CA, USA) devices.
Best-corrected VA, ophthalmoscopy, fundus photography, fluorescein angiography, and OCT were employed to establish baseline characteristics. These examinations were subsequently repeated to monitor the safety and efficacy of treatment.
Methods of intravitreal injection
Methods of intravitreal injection (aseptic technique) have evolved. Currently, we anesthetize with a drop of topical proparacaine followed by initial betadine. After 30 seconds, these are followed by 2 additional drops of topical viscous lidocaine applied 2-5 minutes apart. An additional drop of betadine 5% is placed 30 seconds prior to injection. In order to minimize secondary corneal abrasions, eyelid speculums are only used for those who cannot allow digital retraction. In this series, either bevacizumab (1.25 mg/0.05 mL, 2.0 mg/0.08 mL, 2.5 mg/0.1 mL, or 3.0 mg/0.12 mL [as commercially available] in a tuberculin syringe) or ranibizumab (0.5 mg/0.05 mL or 2.0 mg/0.05 mL [non-commercially available pilot study]) was introduced at an angle through the pars plana through a 30-G needle (36). Optic nerve perfusion and VA were normalized prior to discharge. Injections were repeated every 4 to 12 weeks, modulated based on changes in VA and clinical features.
Treatment goals
Treatment goals were preservation of macular anatomy and VA. This required dose escalation when objective findings (OCT, VA, or fluorescein angiography) or VA worsened. Dose escalation was accomplished by injecting larger dose volumes or decreasing time intervals between injections. That is, treatment intervals are first shortened to 4 weeks while maintaining the lowest dose, then increased dose/dose volumes are employed when the 4-week intervals fail to control the RM.
This study adhered to the tenets of the Declaration of Helsinki and the Health Insurance Portability and Privacy Act of 1996 and was approved by the institutional review board of The New York Eye Cancer Center.
Statistical methods
The primary outcome measure was the time of diagnosis of a reduction in VA of 3 or more ETDRS lines of vision. Thus, patients who did not experience loss of 3 lines or more were censored at the time of their last follow-up. Product-limit estimates (Kaplan-Meier estimates) of the event and event-free probabilities were obtained for the group as a whole, for the subset of patients with a known radiation dose, and by radiation dose quartile.
After assessing functional form and the validity of the proportional hazards assumption, a Cox proportional hazards regression model was used to examine the relationship between time to loss of 3 lines or more lines of vision and the radiation dose to the fovea. The change in hazard associated with an increase of 1 Gy was estimated (hazard ratio), as was its 95% confidence interval. The Cox proportional hazards model was also used to obtain event-free probabilities at the radiation dose quartiles observed in the data.
Results
Over the last 10 years, 120 patients with RM secondary to ophthalmic plaque irradiation were treated with intravitreal anti-VEGF therapy. We began our experience by offering consecutive patients off-label treatment with intravitreal anti-VEGF therapy despite their VA, or length of time with RM and subsequent vision loss.
In this early phase of our experience, a subset of patients (n = 15) dropped out of treatment after only 1-2 injections. These patients could not tolerate intravitreal injections or there was not an appreciable improvement in VA or clinical findings. Though this subset dropped out before they received 3 intravitreal injections, they were observed for subsequent complications. However, due to their short treatment interval, they were excluded from the analysis of VA and CFT. Of these, 7 (7/15, 47%) began with VA worse than 20/200. An additional 6 patients underwent less than 3 injections but were lost to follow-up (<6 months follow-up) and were excluded.
Patient demographics
A total of 99 patients were available for analysis of the main outcome measures of VA and CFT. Their mean age at time of injection was 64 years (range 33-89 years). There were 56 women, 45 right eyes, 9 patients with diabetes, and 38 patients with hypertension. By 7th edition American Joint Committee on Cancer criteria for T-size category, there were 48 T1, 35 T2, 14 T3, and 1 T4 tumors (unknown = 1). We report on a mean treatment interval of 38 months (range 6-108 months) and a mean observation period from the time of initial tumor staging to final follow-up visit of 6.75 years (range 11-130 months) (Tab. I).
Summary of findings of 99 patients with radiation maculopathy and posterior uveal melanoma treated with intravitreal anti-VEGF therapy
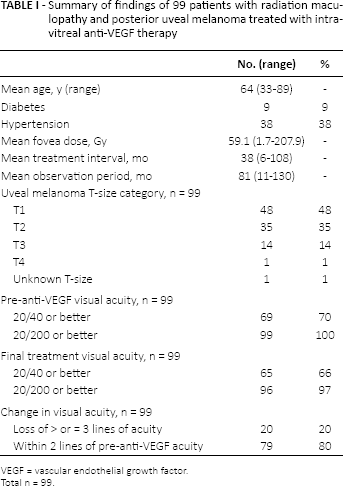
VEGF = vascular endothelial growth factor.
Total n = 99.
Microangiopathy
Anti-VEGF therapy was associated with a general trend towards initial decreased vascular permeability (Fig. 1). This was qualitatively evidenced by sharpening of blood vessel edges and decreased edema on fluorescein angiography as well as resolution of hemorrhages and exudates. Cotton-wool spots had a longer latency to response, but there was a general trend towards thinning, then resolution of this finding.
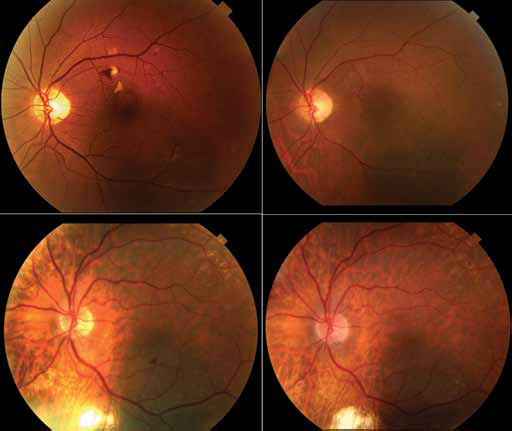
Two cases of long-term anti–vascular endothelial growth factor (VEGF) suppression of radiation maculopathy. Fundus photographs. Top left: Initial presentation of a subfoveal choroidal melanoma with radiation-related retinal hemorrhages and cotton-wool spots. Top right: After 9 years of continuous anti-VEGF therapy, the retinal hemorrhages and cotton-wool spots have improved, though retinal telangiectasias and microaneurysms have evolved over time. The visual acuity was maintained at 20/20. Bottom left: Initial presentation of a subfoveal choroidal melanoma with radiation-related retinal hemorrhage. Bottom right: After 7 years of continuous anti-VEGF therapy, the retinal hemorrhages and macular edema have improved. Visual acuity is maintained at 20/20.
While under treatment, re-emergence of hemorrhages and cotton-wool spots was atypical and treated with dose escalation. Despite these clinical improvements, most patients developed retinal microaneurysms, capillary nonperfusion, and retinal telangiectasias over time (Fig. 1). Focal retinal laser photocoagulation was required to control focal edema and/or neovascularization (n = 8/99, 8%) while under continuous anti-VEGF treatment. However, in all 8 cases, despite focal laser coagulation, significant retinal edema persisted and the treatment dose and treatment interval were maintained (dose could not be reduced and interval could not be lengthened).
Exudation and macular edema
Initial reduction of macular edema was the most consistent and reproducible finding, and was typically accompanied by improvements in VA. In general, patients would experience a period of time (several months to several years) of suppressed macular edema, followed by its re-emergence. At that point, dose escalation was employed to suppress progressive macular edema over time (Fig. 2).
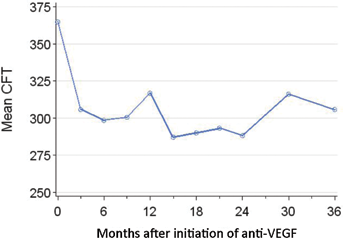
Line graph shows the mean central foveal thickness (CFT) as measured by spectral-domain optical coherence tomography (OCT) imaging over time. There is an initial decrease in CFT followed by a plateau and a late rise. Sixty-three patients are included in this graph due to the advent and availability of spectral-domain OCT imaging.
Optical coherence tomography imaging
Macular edema was best seen on OCT imaging, which typically revealed a thickened macular retina containing hyporeflective fluid-filled cysts. Initial postintravitreal bevacizumab OCT/scanning laser ophthalmoscope imaging revealed thinning of the macular retina with restoration of the normal macular contour. Due to the availability of the spectral-domain technology (post-2005), there were 63 patients with initial central foveal thickness values. At their 3-month treatment interval, 87% were stable (n = 15/63, within 10 μm of their initial CFT) or improved (n = 39/63, with a reduction in central foveal thickness of >10 μm). The mean initial CFT was 364.9 µm (n = 63, SD 134.26, range 150-873); at 2 years of treatment, the mean CFT was 288 µm (n = 32, SD = 66.2, range 163-472), and at 4 years, mean CFT was 382.8 µm (n = 8, SD = 239.2, range 215-774) (Fig. 2).
Progressive macular edema over time prompted dose escalation. In that dose escalation was not available until 2011, higher doses were not offered to all patients at each interval. By 2 years of treatment, 32% (n = 24/74) had undergone dose escalation; by 5 years of treatment, this increased to 73% (n = 33/45) on dose escalation. In addition, at last treatment visit, 51% (n = 50/99) were on baseline dose of either 1.25 mg bevacizumab (n = 44) or 0.5 mg ranibizumab (n = 6), while 49% (n = 49/99) required dose escalation to 2.0 mg (n = 21), 2.5 mg (n = 21), or 3.0 mg (n = 6) bevacizumab and 2.0 mg ranibizumab (n = 1).
Visual acuity
Due to the complex nature of management in this cohort, VA results are presented as gain or loss of 1, 2, 3, or more lines of EDTRS best-corrected vision.
For the entire cohort (n = 99) measured at the time of their last treatment examination, 20% (n = 20/99) lost 3 or more lines of VA compared to their pre-anti-VEGF VA, doubling their minimum angle of resolution. Thus, at last follow-up, 80% remained within 2 lines of their pre-anti-VEGF VA or better. Kaplan-Meier analysis of the probability of remaining within 2 lines of pre-anti-VEGF VA was 94.7% at 1 year, 69% at 5 years, and 37.7% at 8 years of anti-VEGF therapy (Fig. 3). Prior to anti-VEGF therapy, 69 (n = 69/99, 69%) had VA better than or equal to 20/40 and 99 (n = 99/99, 100%) were better than or equal to 20/200. At their last treatment examination, 65 (n = 65/99, 65%) had VA better than or equal to 20/40 and 96 (n = 96/99, 96%) were better than or equal to 20/200. However, there was a trend towards patients discontinuing therapy once their VA became <20/200.
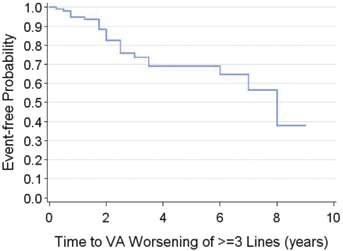
Kaplan-Meier analysis of the probability of remaining within 2 lines of initial visual acuity (VA) was 69% at 5 years and 38% at 8 years of anti–vascular endothelial growth factor therapy. In this series, n = 20/99 (20%) lost ≥3 lines from their baseline VA.
Radiation dose
Uveal melanomas were treated with palladium-103 or iodine-125 ophthalmic plaque brachytherapy over 5-7 consecutive days as per the guidelines of The American Brachytherapy Society Ophthalmic Oncology Task Force (13). In this series, the mean foveal dose was 59.1 Gy (range 1.7-207.9).
Radiation dose to fovea
Radiation dose to fovea has been shown to be a risk factor for RM (16). Of the 20 patients who lost 3 or more lines of VA, their mean fovea dose was 78.5 Gy (range 12.5-207.9, 1 unknown dose) with a mean follow-up interval of 41.2 months (range 9-96 months). Of the 79 patients with stable or improved VA, mean fovea dose was 55.1 Gy (range 1.7-148.1, 4 unknown doses) with a mean follow-up of 35.7 months (range 6-108 months). However, using a Cox model, this difference was not found to be statistically significant (chi-square test p value = 0.23). The hazard ratio was 1.006 (95% CI 0.996-1.016) for every 1 Gy increase in radiation.
Long-term safety and tolerability
Side effects
Acute side effects include local conjunctivitis and blepharitis (related to topical betadine or anesthetics), corneal abrasion, transient vision loss related to high injection volumes (typically 0.1 mL and above), and 1 case of endophthalmitis. In general, immediate postinjection transient loss of vision was treated with close observation to recovery. Anterior chamber paracentesis was rarely required (n = 2, in the same patient). No treatment-related retinal detachments or vitreous hemorrhages occurred. Long-term side effects include ocular hypertension (n = 6), typically treated with topical ocular hypotensive agents 48 hours prior to intravitreal injection. Only one patient underwent enucleation (after anti-VEGF treatment was electively stopped by the patient). After 2 years of successful intravitreal anti-VEGF therapy, he was lost to follow-up and returned 2 years later (off treatment) with pain, neovascular glaucoma, and vitreous hemorrhage. Despite local tumor control, enucleation was performed for the blind, painful eye.
We report no bleeding, neuropathy, dyspnea, arrhythmias, hypertension, swelling, or mood changes, as has been reported with the use of systemic bevacizumab. There were 4 deaths during the 10-year observation period: 2 patients died of metastatic melanoma, 1 of cardiac disease, and 1 of pulmonary disease.
Long-term patient retention
Long-term therapy of 4- to 12-week interval intravitreal injections can be a burden to both the patient and treating physician. Our longest interval of treatment is 9 years (at regular 4-week intervals). However, we found that most patients (76%, n = 75/99) have elected to continue treatment. Patients typically state that the benefit of retaining functional VA outweighs the burden of monthly injections. Of the 24 who have ceased treatment, 4 stopped due to patient preference, 11 due to eventual poor vision (worse than 20/200), 1 due to enucleation, and 2 were lost to follow-up. Since 2005, post-treatment complete resolution of RM (without relapse) was rare (n = 2).
Discussion
Long-term suppression of RM with preservation of vision can be achieved with periodic intravitreal anti-VEGF therapy. In this study, treatment was well-tolerated and typically involved dose escalation (decreased time intervals and increased dose) based on objective findings over time. Objective findings of long-term suppression of macular edema, cotton-wool spots, and retinal hemorrhages suggest that periodic intravitreal anti-VEGF therapy effects a long-term disruption of the biologic process known as radiation vasculopathy. As in most noninfectious diseases, pharmacologic suppression offers delay from relatively acute organ failure.
Visual acuity outcomes after ophthalmic radiation therapy have been historically poor (13, 41). The most common cause of irreversible vision loss has been due to RM. For example, The Collaborative Ocular Melanoma Study (COMS) found that 45% of irradiated eyes were 20/200 or worse within 3 years after iodine-125 plaque therapy (this statistic includes eyes that did not develop RM) (42). In comparison, our study reports on a series of patients selected to exhibit progressive RM and thus likely to lose their vision. In our high-risk cohort, 80% achieved stable or improved vision for a mean follow-up of more than 3 years. These findings stand in stark contrast to our experience and that of the COMS (42).
Previous studies exist showing that RM is treatable with intravitreal anti-VEGF therapy. But all these studies have been limited to follow-up of less than 2 years (26, 27, 30, 37, 40, 43–44–45). In fact, few long-term studies of intravitreal anti-VEGF therapy exist. Recently, Peden et al (46) reported on a series of 109 eyes with age-related macular degeneration (AMD) using a continuous fixed-interval dosing regimen over 7 years. They found that 93.2% of eyes had stable or improved vision and that continuous therapy results in more favorable VA outcomes than sporadic, as-needed (treat and extend) therapy (46).
Alternative treatment regimens have been considered due to treatment burden, cost, and concerns with possible retinal pigment epithelium (RPE) atrophy resulting from long-term VEGF suppression of the RPE. However, our clinical experience over 10 years suggests that almost all anti-VEGF suppressed RM is slowly progressive and that complete resolution (without relapse) of RM was rare (2%). Similarly, secondary enucleation was also rare (n = 1), only seen in one patient whose retinal ischemia severely worsened, leading to neovascular glaucoma after he voluntarily stopped anti-VEGF treatment (47).
Limitations of our study are mostly due to the 10-year span and evolution of techniques/technology over time. This resulted in a retrospective, uncontrolled, all-inclusive study design providing difficulties with respect to outcome assessment. For example, 15 patients were excluded from the outcome assessments (of VA and CFT) due to receiving only 1-2 injections before discontinuation. Though we had an intention to treat, the results clearly demonstrated that only sustained suppression of this progressive disease is effective. In addition, dose escalation was only offered in the last 4 years of the study due to the availability of higher doses of anti-VEGF medications. We chose to report only OCT findings over the last 5 years due to the superiority of the spectral-domain versus the prior time-domain technology and their relative abilities to measure central foveal thickness. Finally, due to the numerous factors affecting VA outcomes, we reported on how foveal radiation dose (and not tumor location) affected VA.
Radiation maculopathy is a chorioretinal vasculopathy that is (at first) clinically evident as intraretinal hemorrhages, cotton-wool spots, and edema (48–49–50). Untreated RM edema typically results in edema, ischemia, scarring with symptoms of metamorphopsia, and vision loss (2). This study suggests that continuous periodic intravitreal anti-VEGF therapy offers suppression of RM edema and long-term preservation of vision.