
Abstract
Aim
Findings from recent studies suggest that obesity may be associated with an increased risk of endometrial cancer, but several earlier studies were less conclusive. Here we strive to estimate this relationship in a meta-analysis of published data.
Methods
We searched Pubmed and Embase for studies on body mass index and the risk of endometrial cancer, published from 1989 to 2011. Data were independently extracted and analyzed using random or fixed effects meta-analysis depending on the degree of heterogeneity.
Results
Seven cohort studies and 11 case-control studies were included in the meta-analysis. Overall, the conditions of excess body weight ([EBW] defined as body mass index [BMI] ≥25 kg/m2), obesity (BMI ≥30 kg/m2) and overweight (25< BMI <30 kg/m2) were associated with an increased risk of endometrial cancer (relative risk [RR] for EBW=1.62, 95% confidence interval [CI], 1.39-1.89; for obesity RR=2.54, 95% CI, 2.11-3.06; for overweight RR=1.32, 95% CI, 1.16-1.50). Subgroup analyses showed that the positive associations were independent of study design, geographic locations, self-reported BMI, alcohol use, smoking habit, history of diabetes, hormone therapy, age at menarche, age at menopause, parity, and age at first full term pregnancy. However, there was no statistically significant association between EBW and endometrial cancer risk for measured BMI (for EBW RR=1.29, 95% CI, 0.66-2.53).
Conclusions
The findings from this meta-analysis strongly support that the conditions of EBW, overweight, and obesity are all associated with an increased risk of endometrial cancer. Also, the strength of the association increases with increasing BMI.
Introduction
The International Agency for Research on Cancer recently estimated that endometrial carcinoma is the most common gynecological cancer in the developed world (1). Endometrial cancer is the third most common cancer in women in Western countries, accounting for 6%-9% of all cancer types in women (2). It was estimated that in 2006 a total of 40,200 women in the US were affected by endometrial cancer (3), and that women in the US have a 2.6% lifetime risk of being diagnosed with this disease (4). Endometrial cancer is often diagnosed at an early stage, and has a high cure rate (5). Thus, enhancing the survivors’ quality of life is of high priority. Therefore, early intervention on modifiable risk factors for endometrial cancer is very important.
Obesity is an increasing problem in the US. About 65% of the population in the US is overweight and 30% of the population is obese, according to their body mass index (BMI) (6). Obesity affects more than 25% of adult women in the US and continues to increase in prevalence. Numerous epidemiological studies have demonstrated that obesity is a major risk factor for endometrial cancer (7). Although an average woman has a 3% lifetime risk of developing endometrial cancer, this risk raises to 9%-10% for obese women (8). However, the recently published studies on the association between excess body weight (EBW) and the risk of endometrial cancer have no consistent conclusion.
As to evaluate the association between EBW and the risk of endometrial cancer, we carried out a systematic review and meta-analysis of published cohort studies and case-control studies.
Materials and Methods
Search Strategy
We identified eligible studies (published up to the 15th of February 2011) by performing a comprehensive search in Pubmed and Embase. Research papers were selected using the following sets of keywords: “body mass index” or “BMI” or “obesity” or “adiposis” or “excess body weight”; “endometrial cancer” or “endometrial carcinoma” or “endometrial adenocarcinoma” or “endometrial tumor” or “endometrial neoplasm” or “EC”; “risk” or “incidence” or “mortality”. The search was performed on studies conducted on human subjects, with restriction on English language papers. We reviewed all abstracts obtained from our search for relevance, we manually reviewed bibliographies and review articles for additional citations, and obtained the full text of all potentially relevant articles. We did not consider abstracts or unpublished reports.
Inclusion and Exclusion Criteria
We evaluated all of the studies retrieved according to our selection criteria. The following criteria were used to include published studies: (i) the study had to be a cohort or case-control study examining exposure to EBW or high BMI and the incidence or mortality rates of endometrial cancer; (ii) the study had to contain an explicit definition of BMI, as well as of obesity and overweight conditions, with raw data for each group. The major reasons for exclusion of studies were: (i) no raw data available; (ii) duplicate studies; (iii) the data reported were not usable.
Data Extraction
Two investigators independently extracted the data, discussed disagreements, and reached consensus on all issues. From each study considered the following information was extracted using a standardized data-collection protocol: the first author's name, year of publication, country of origin, study design (cohort versus case-control), period of diagnosis, sample size, exposure measurement method (self-reported versus measured BMI versus diagnosis of obesity), exposure definitions (BMI definitions of overweight or obese), and variables for which the analysis was adjusted. Seven cohort studies and 11 case-control studies were included in the meta-analysis. All studies have a high quality evaluation, in each research, such as taking measures to control for confounding factors, describing the results of the lost object, having enough time to review. Some of the studies were published in high-impact journals (such as the Journal of the National Cancer Institute, Cancer Research, the International Journal of Cancer, and the International Journal of Epidemiology). For studies including subjects of different ethnic groups, when possible, data were separately extracted for each ethnic group. We did not define any minimum number of patients for a study to be included in our meta-analysis.
Exposure Definition
We defined body mass groups using the following BMI categories: normal weight (BMI ≥18.5 kg/m2 and <25 kg/m2), overweight (BMI ≥25 kg/m2 and <30 kg/m2), and obese (BMI ≥30 kg/m2). Combined overweight and obesity may be expressed as EBW (BMI ≥25 kg/m2). These groupings represented the divisions or quartiles most frequently reported in the articles included, and may somewhat differ from the BMI categories defined in other studies (9). For each study, we selected the BMI-cancer association that most closely approximated each of these categories and the date of BMI determination that was most commonly reported.
Statistical Analysis
The strength of the association between the EBW and the risk of endometrial cancer was measured by risk ratios (RRs) with 95% confidence intervals (CIs). Pooled estimates of the average RR were obtained by calculating a weighted average of the RRs from each study. Either the random-effects or the fixed-effects model were used for the meta-analysis. When the I2 statistic was >50%, a random-effects model was chosen, otherwise a fixed-effects model was used. Heterogeneity among studies was assessed using Q and I2 statistics, which test the total variation across studies that was attributable to heterogeneity rather than to chance (10). Funnel plots and test statistics were used to determine the existence of potential publication bias. All analyses were performed with Review Manager 5.0 software (The Cochrane Collaboration, Oxford, United Kingdom, 2008).
Results
Study Characteristics
There were 395 published papers relevant to the search terms. After screening the title, 192 papers were excluded. Thus, 203 potentially eligible studies were reviewed and, after this step, additional 185 studies were excluded, leading to a final number of 18 papers included. Of these, 7 cohort studies and 11 case-control studies were included in the pooled analyses (9, 11–27). The baseline characteristics of the selected studies included in the meta-analysis are summarized in Table I. Figure 1 describes the results of the systematic literature search papers.
Characteristics of Cohort and Case-Control Studies Included in this Meta-Analysis
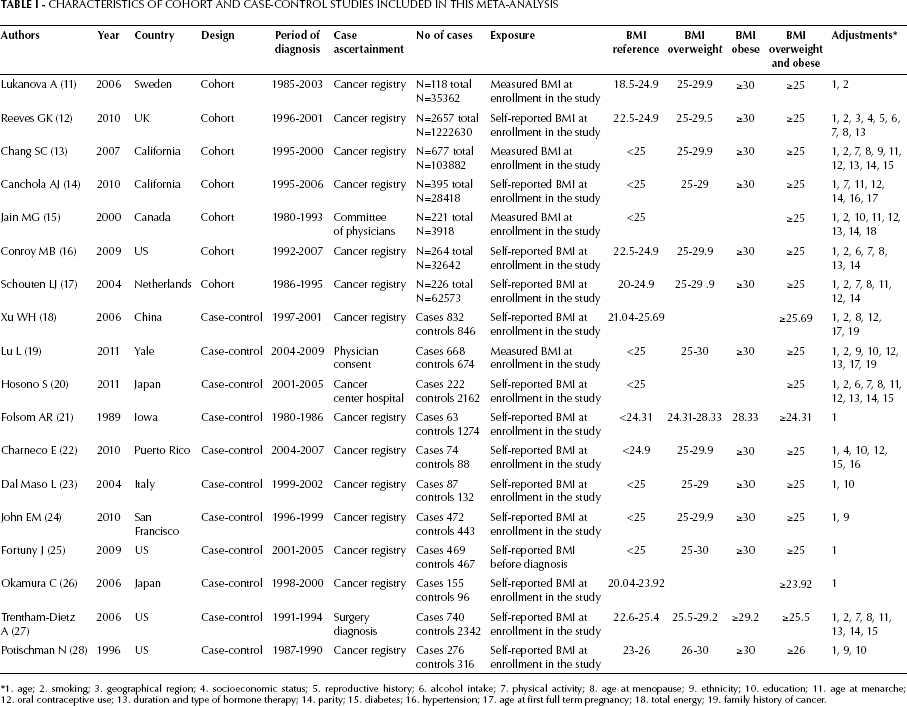
1. age; 2. smoking; 3. geographical region; 4. socioeconomic status; 5. reproductive history; 6. alcohol intake; 7. physical activity; 8. age at menopause; 9. ethnicity; 10. education; 11. age at menarche; 1 2. oral contraceptive use; 13. duration and type of hormone therapy; 14. parity; 15. diabetes; 16. hypertension; 17. age at first full term pregnancy; 18. total energy; 19. family history of cancer.

Results of the systematic literature search: number of studies and their inclusion or exclusion.
Meta-Analysis
The combined results of all the studies considered showed that there was a statistically significant association between EBW, overweight, or obesity and endometrial cancer risk (for EBW RR=1.62, 95% CI, 1.39–1.89; for obesity RR=2.54, 95% CI, 2.11–3.06; for overweight RR=1.32, 95% CI, 1.16–1.50). The strength of the association increased with increasing BMI (Tab. II, Figs. 2–4).
Statistical Results of Cohort and Case-Control Studies Included in the Meta-Analysis by Revman 5.0

no statistically significant correlation.
13 year was used as a cut-off point.
49 year was used as a cut-off point.
0 was used as a cut-off point.
20 year was used as a cut-off point.
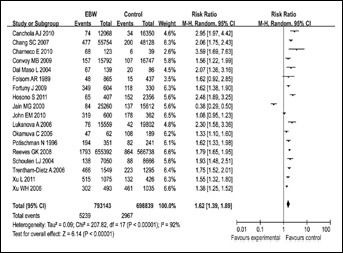
Forest plot for the association between EBW and endometrial cancer risk. Risk ratios derive from the random effects model by Revman 5.0.
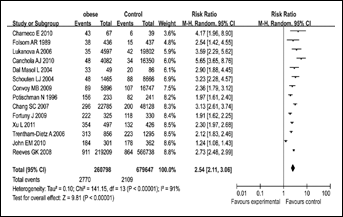
Forest plot for the association between obesity and endometrial cancer risk. Risk ratios derive from the random effects model by Revman 5.0.
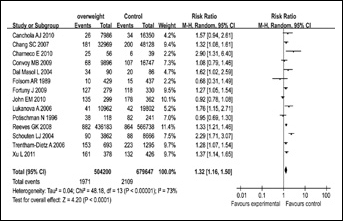
Forest plot for the association between overweight subjects and endometrial cancer risk. Risk ratios derive from the random effects model by Revman 5.0.
Subgroup Meta-Analyses
We then conducted subgroup meta-analyses by study design, geographic locations, BMI ascertainment, and possible confounders (e.g. alcohol use, smoking status, history of diabetes, hormone therapy [HT], age at menarche (≥13 year cf <13 year) (15), age at menopause (≥49 year cf <49 year) (13) (the study have shown the mean age at menopause in this population to be about 49–50 years, thus, age 49 was used as a cut-off point in subgroup analyses based on age in women), parity (>0 cf 0) (15) and age at first full term pregnancy) <20 year cf ≥20 year) (24)).
Analyses by Study Design
When stratifying for study design, we found that there was a statistically significant association between the conditions of EBW, overweight or obesity and endometrial cancer risk in studies with a cohort design (for EBW RR=1.62, 95% CI, 1.14–2.30; for obesity RR=3.11, 95% CI, 2.62–3.69; for overweight RR=1.47, 95% CI, 1.22–1.78) as well as in studies with a case-control design (for EBW RR=1.60, 95% CI, 1.39–1.84; for obesity RR=2.06, 95% CI, 1.61–2.63; for overweight RR=1.18, 95% CI, 0.96–1.45; for this last correlation there was no statistical significance).
Analyses by Geographic Locations and BMI Ascertainment
When stratifying for geographic locations, there was a statistically significant correlation between the conditions of EBW, overweight or obesity and endometrial cancer risk for Asians (for EBW RR=1.68, 95% CI, 1.35–2.09; for obesity RR=2.65, 95% CI, 1.34–5.24; for overweight RR=1.80, 95% CI, 0.89–3.67) and non-Asians (for EBW RR=1.59, 95% CI, 1.29–1.95; for obese, RR=2.52, 95% CI, 2.04–3.12; for overweight RR=1.29, 95% CI, 1.12–1.48). When stratifying for BMI ascertainment, there was a statistically significant correlation between the conditions of EBW, overweight or obesity and endometrial cancer risk for self-reported BMI (for EBW RR=1.70, 95% CI, 1.49–1.94; for obesity RR=2.46, 95% CI, 1.96–3.08; for overweight RR=1.29, 95% CI, 1.10–1.52) and for measured BMI (for EBW RR=1.29, 95% CI, 0.66–2.53; for obesity RR=2.84, 95% CI, 2.17–3.71; for overweight RR=1.38, 95% CI, 1.22–1.43).
Analyses by Confounders
When stratifying for the adjustment for confounders, there was a statistically significant correlation between EBW and endometrial cancer risk for a number of factors: alcohol use (for EBW RR=1.77, 95% CI, 1.52–2.07) or no alcohol use (for EBW RR=1.58, 95% CI, 1.29–1.94); smokers (for EBW RR=1.57, 95% CI, 1.27–1.93) or non-smokers (for EBW RR=2.69, 95% CI, 1.35–2.13); history of diabetes (for EBW RR=2.09, 95% CI, 1.72–2.54) or no history of diabetes (for EBW RR=1.50, 95% CI, 1.25–1.79); HT (for EBW RR=1.48, 95% CI, 1.11–1.98) or no HT (for EBW RR=1.69, 95% CI, 1.43–2.00), age at menarche (13 year was used as a cut-off point) (for EBW, RR=1.63, 95% CI, 1.01–2.64) or no age at menarche (for EBW RR=1.58, 95% CI, 1.39–1.80); age at menopause (49 year was used as a cut-off point) (for EBW RR=1.79, 95% CI, 1.56–2.06) or no age at menopause (for EBW RR=1.53, 95% CI, 1.17–2.00); parity (0 was used as a cut-off point) (for EBW RR=1.62, 95% CI, 1.07–2.44) or no parity (for EBW RR=1.56, 95% CI, 1.37–1.78); and, finally, age at first full term pregnancy (20 year was used as a cut-off point) (for EBW RR=1.70, 95% CI, 1.29–2.25) or no age at first full term pregnancy (for EBW RR=1.60, 95% CI, 1.33–1.93).
Test for Heterogeneity
Statistically significant heterogeneity was observed among the included studies (for EBW, x2=207.82, p<0.00001, I2=92%; for obesity, x2=141.15, p<0.00001, I2=91%; for overweight, x2=48.18, p<0.00001, I2=73%). In addition, we found evidence of an existing publication bias, as shown by the funnel plot in Figure 5.
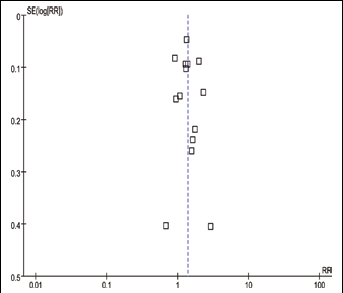
Funnel plot for all studies included in this meta-analysis of EBW by endometrial cancer risk (Revman 5.0).
Discussion
Obesity is one of the most common disorders in medical practice and is a major public health problem. A recent national survey in the US found that approximately 50% of women are overweight and 25% are obese. Previous studies have shown that obesity is associated with an increased risk of various types of cancers, among which cancers of the stomach (29–32), liver (33–37), ovaries (38–41), pancreas (42–45), and colon (46–49). Our analysis of published cohort and case-control studies also support a positive association between EBW, overweight or obesity and the risk of endometrial cancer. The strength of the association increased with increasing BMI values. Moreover, a previous review also confirmed such association with endometrial cancer (50).
In a subgroup analysis stratified on basis of the study design, we found a statistically significant link between EBW or obesity and the risk of endometrial cancer in cohort design and case-control design respectively. When stratifying the studies for either Asian or non-Asian populations, we found that the conditions of EBW, overweight and obesity were associated with a statistically significant increased risk of endometrial cancer among both Asians and non-Asians. Setiawan et al (51) showed that the interracial differences in endometrial cancer risk do not appear to be explained by differences in the distribution of known risk factors among women of different races/ethnicities.
This meta-analysis was based on data from prospective studies. Individual studies may have failed to control for potential confounders. Several studies adjusted their analysis for smoking status (11–13, 15–20, 27), alcohol consumption (12, 16, 19, 20), diabetes (13, 20, 22, 27), and/or HT (12, 13, 15, 16, 19, 20, 27), since these factors have been associated with the risk of endometrial cancer in epidemiological studies. We found that there was a statistically significant correlation between EBW and endometrial cancer risk for smoking subjects. Lindemann and colleagues (52) also reached a similar conclusion. We also found a statistically significant correlation between EBW and endometrial cancer risk for alcohol use. With regard to the history of diabetes, Saltzman et al (53) found that type 2 diabetes was associated with endometrial cancer in women with a BMI <35 but not in women with a BMI ≥35. A history of diabetes was associated with a twofold increased risk of endometrial cancer among hypertensive women, but no association was observed among non hypertensive women. Type 2 diabetes seems to be associated with endometrial cancer irrespective of the presence of other risk factors for this disease, except, possibly, hypertension and extreme obesity. We also found a statistically significant correlation between EBW and endometrial cancer risk for HT. In the European Prospective Investigation into Cancer and Nutrition cohort (EPIC), obesity was positively associated with endometrial cancer risk in postmenopausal women who never used HT, but was not associated with an increased risk in those who ever used HT (54). Age at menarche, age at menopause, parity, and age at first full term pregnancy are intrinsic confounders for the relationship between obesity and endometrial cancer. Therefore, ignoring these confounders could make the association between obesity and endometrial cancer less strong.
There are several potential mechanisms by which EBW may increase the risk of endometrial cancer. Weight gain is largely reflected in body fat accumulation. Excessive conversion of androstenedione to oestrone, and decreased serum levels of the sex hormone-binding globulin (SHBG), related to obesity, create an estrogen-rich environment that stimulates the development of endometrial cancer cells (55). Premenopausal obese women are likely to have anovulatory cycles and decreased levels of progesterone. In particular, obese women are exposed to prolonged unopposed estrogens during early adulthood and, as a result, might have an increased risk of endometrial cancer (56). In postmenopausal women, the mechanism of endometrial cancer development can be explained by the peripheral conversion of androgens into estrogens caused by an increase in peripheral fat stored. This hormonal alteration stimulates the proliferation of endometrial cells by inhibiting apoptosis, thus promoting angiogenesis (57). Other possible mechanisms may also involve: (i) insulin resistance and hyperinsulinemia (58); (ii) adiponectin (59); (iii) sex hormones, adipokines, inflammatory factors, and cytokines.
To our knowledge, the strengths of this study include: the consistency of a positive association between EBW and endometrial cancer across some high-quality studies with different patient populations; the report of an increasingly significant association with increasing BMI values; the definition of comparable BMI categories for each study; the ability to stratify by study design, geographic locations, and BMI ascertainment; and, finally, the ability to assess the effect of including only estimates adjusted for potential confounders.
In summary, this meta-analysis of prospective studies indicates that the conditions of EBW, overweight, or obesity are positively associated with the risk of endometrial cancer. Additionally, the strength of the association increased with increasing BMI. Nevertheless, more research is needed to unravel the underlying mechanisms of this association and to determine whether interventions aimed at lowering the body weight can decrease the risk of endometrial cancer.
Footnotes
Acknowledgments
The authors thank Juyi Li and Jilian Chen for the technical assistance and the whole medical department for the valuable discussions.